
Abstract
We conducted a systematic review of large, well-conducted randomised trials designed to evaluate the effectiveness of telemonitoring on patients with congestive heart failure (CHF). Two people reviewed 125 articles independently and selected 13 articles for final review. These studies concerned 3480 patients. The follow-up period of the studies was 3–15 months. Pooled estimate results showed that there was an overall reduction in all-cause mortality (P = 0.02). There was no overall reduction in all-cause hospital admission (P = 0.84), although there was a reduction in CHF hospital admission (P = 0.0004). There was no reduction in all-cause emergency admission (P = 0.67). There was no significant difference in length of stay in hospital, medication adherence or cost. Telemonitoring in conjunction with nurse home visiting and specialist unit support can be effective in the clinical management of patients with CHF and help to improve their quality of life.
Introduction
Congestive heart failure (CHF) is a common chronic condition with a prevalence of about 13% among those aged 85 years or above. 1,2 Telemonitoring in CHF improves health outcome for patients and reduces the number of hospitalisations. 3,4 However, many studies consider nurse telephone support and home-based telemonitoring as equivalent, and either report combined outcomes or present results synonymously. 5 Telephone support typically comprises patient follow-up, education and counselling delivered via a telephone call made by a specialist nurse. However, patients receiving this usually have only mild to moderate CHF symptoms (New York Heart Association, NYHA class I-II). Telemonitoring involves home care of patients using specialist telecare devices and is often done for patients with severe symptoms of heart failure (NYHA class III-IV). 5
A review which differentiated these approaches and determined the effectiveness of each separately concluded that a technology-based approach to patient home monitoring (telemonitoring) was more effective. 6 In other systematic reviews, telemonitoring has been compared to a number of alternative approaches, including patient education, specialist (clinician or cardiologist) follow-up, nurse home visiting and telephone support. 7–10 The general conclusion is that telemonitoring alone is insufficient to reduce readmission rates and improve quality of life, and must be integrated with nurse visits and specialist follow-up. Most reviews conclude that there is a lack of well conducted large trials that evaluate the effectiveness of telemonitoring versus usual care.
We have conducted a systematic review to identify suitable studies and from these have assessed the effectiveness of telemonitoring on primary and secondary outcomes.
Methods
Data acquisition
We conducted a systematic review of randomised controlled trial (RCT) studies that were designed to evaluate the effectiveness of telemonitoring on patients with CHF. We searched the following databases: Medline, Cinhal, British Nursing Index, ACM, Scopus, Safari, HMIC, IEEE and Springerlink. We used combinations of the search terms shown in Table 1. Synonyms of near equivalent terms in the columns were combined through the OR operator, and these search terms were combined with the AND operator to determine candidate publications.
Search terms used in the systematic review
We searched for publications between January 1969 and October 2009, and our searches were conducted between December 2008 and October 2009. The title and abstract of each resulting publication in our list was checked according to the inclusion and exclusion criteria described below. References from the selected articles were checked to identify any further relevant publications.
Inclusion/exclusion criteria
Our inclusion criteria were:
The studies were randomised controlled trials that included an intervention arm and a control arm at least; The control arm had a clear definition of usual care; The patients only had CHF; The trials had at least 50 patients. There was no specific description of the care provided to patients in the control arm; Only telephone support was used for follow-up, that is, no telemonitoring equipment was used; Patients were not monitored at home, for example those transferred to a residential care facility from hospital.
We excluded studies where:
Data extraction
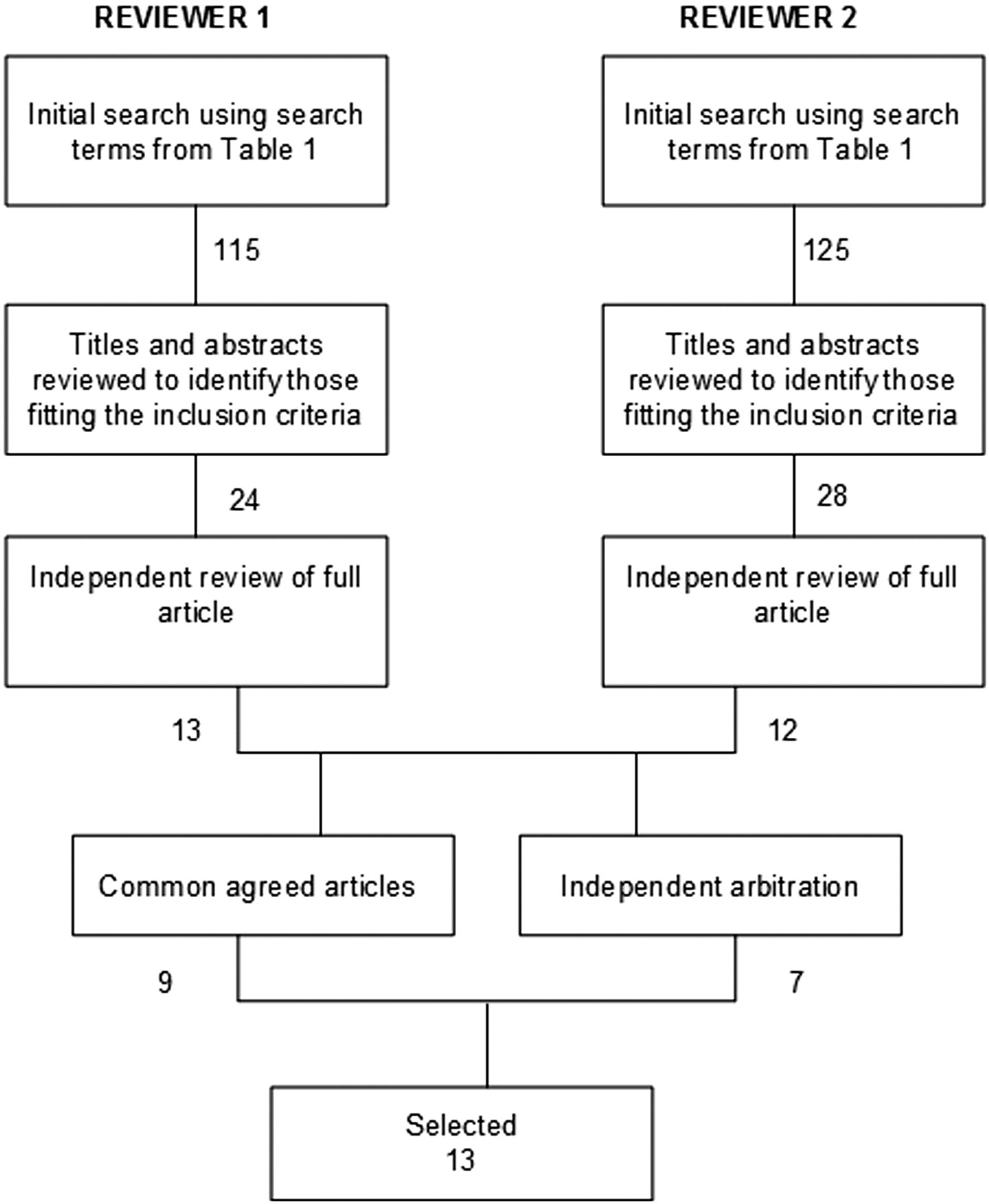
The primary searches were made by two investigators independently. The abstracts of all the potential publications were read independently by each investigator and only publications that met the selection criteria were retained. Full articles were reviewed independently by each researcher and publications that did not meet the selection criteria were excluded. The independent lists were combined and arbitration was used to select publications where there was not common agreement.
Statistical analysis
Meta-analysis was performed using the RevMan 5 statistical package (Review Manager Version 5) from the Cochrane library. Cochrane's test was used for statistical heterogeneity and the presence of publication biases was assessed by means of funnel plots. The pooled effect estimates for binary variables were expressed as risk ratios (RR) with 95% confidence intervals (CI). Risk ratio, also known as relative risk, is defined as ‘the probability of an event in the treatment group divided by the probability of an event in the control group’. 11 Values of confidence intervals less than 1 represent a significant result at the 5% level.
Results
The search process resulted in 13 publications being retained for meta-analysis (Figure 1).
Data extraction method
Study characteristics
Of the 13 RCTs, four were three-arm studies. In studies with more than two arms, only intervention arms that specifically included telemonitoring of patients were included. Second intervention arms with nurse-only support and/or telephone support were excluded as these were not deemed equivalent to a telemonitoring intervention.
Intervention
Telemonitoring of patients with CHF requires equipment to be installed in the patient's home and requires some form of communication. In most studies, a telephone connection was used. In some studies broadband was used for the communication and this was also employed for a video link. Ten studies used physiological monitoring that included daily measurement of body weight, heart rate, blood pressure and an electrocardiogram (ECG). In two of these studies, only daily body weight was transmitted but the patient also gave answers to simple questions regarding their HF symptoms, such as ease of breathing. The data received were analysed by a health-care worker, often a nurse, to determine the severity of the condition and whether appropriate action should be taken. In cases where assessment of measurements indicated deterioration in the condition of the patient, the cardiologist or the doctor was informed of the need for intervention. Otherwise, the patient continued according to the usual study pathway.
Patient inclusion criteria and baseline characteristics
Clinical eligibility criteria for patients for all the studies were a diagnosis of CHF, LVEF <40% and NYHA class I-IV. Some studies applied additional eligibility criteria, including patients with at least one hospitalisation related to CHF or only patients under the care of a specialist nurse or cardiologist. 12,13 The mean age of the patients in the studies included in the review was 55–85 years.
Only six of the 13 studies included full details of co-morbidities, primary cause of CHF and pharmacological intervention in the baseline characteristics of patients participating in the study. 12,14–16 The studies found the most common co-morbidities associated with CHF patients were hypertension, diabetes, myocardial infarction, chronic obstructive pulmonary disease, stroke, valve disease or atrial fibrillation. One study included chronic renal failure as a co-morbidity. 15
The causes of CHF included cardiomyopathy (with idiopathic being the most common form), coronary artery disease, hypertension, valve-related and alcohol-related. Pharmacological interventions commonly used included angiotensin-converting enzyme (ACE) inhibitors, angiotensin receptor blockers (ARB), beta-blockers, digoxin, digitalis, warfarin, loop diuretics, aldosterone antagonist, aspirin and statin. Only one of the studies reviewed included smoking habits of patients to establish or assess its impact on rate of CHF. 16
The follow-up period ranged from 3 to 15 months. Most studies had a follow-up period of 12 months.
Outcomes measured
All studies identified primary outcomes and secondary outcomes. Mortality (10 papers) and hospital admission (6 papers) were the most common primary outcomes. Secondary outcomes included quality of life, cost, adherence behaviour and visits to other health providers.
Ten studies reported mortality (Figure 2) as the primary outcome. 12–21 Five of these ten studies reported significant reductions in mortality and were large scale studies that had more than 80 patients in each group. 13,14,16,17,21 A study by Antinocelli et al. was an exception, which despite being a small scale study showed a significant reduction in mortality. 20 A pooled estimate of the results from the ten studies showed an overall reduction in all-cause mortality (0.77, P = 0.02). Funnel plots did not indicate bias, although there was some evidence of heterogeneity (I2 = 51%, P = 0.03).

Effect of telemonitoring on all-cause mortality
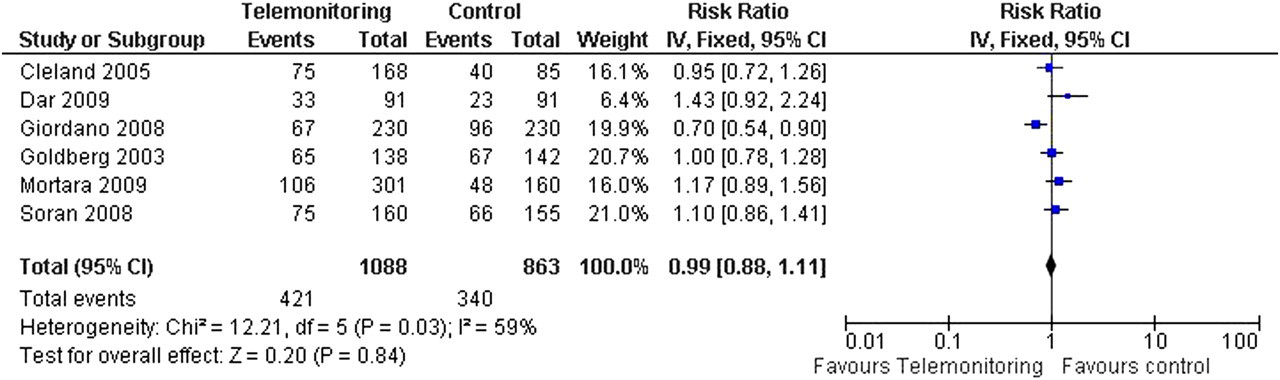
Six studies reported all-cause hospital admissions (Figure 3) as the primary outcome. 14–17,22 None reported a significant reduction and the pooled estimates supported this (0.99, P = 0.84). In contrast, some reduction in CHF hospital admission (Figure 4) was reported in the same studies. Pooled estimates showed a small reduction (0.73, P = 0.0004). Bias was unlikely but the possibility of heterogeneity could not be ruled out in all-cause hospital admission (I2 = 59%, P = 0.03). There was little evidence of heterogeneity for CHF (I2 = 0%, P = 0.44).
Effect of telemonitoring on all-cause hospital admission
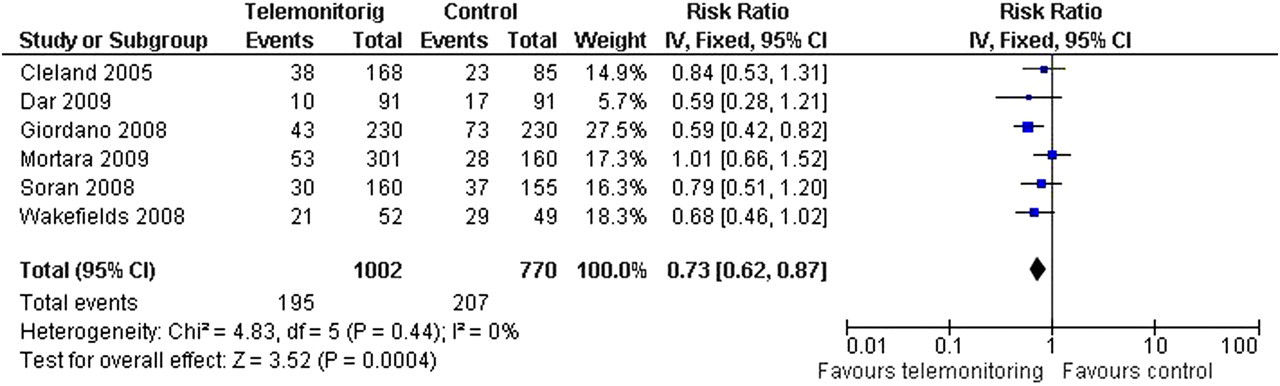
Effect of telemonitoring on CHF hospital admission
Seven studies provided the number of emergency visits (Figure 5) as a secondary outcome. Soran et al. observed no significant difference in emergency visits among the patients in treatment and control arm (P = 0.43). 17 Similar findings were reported by other studies. 16,18,19 In studies by Dar et al. and Dansky et al. lower emergency contacts were observed; however, a study by Cleland et al. reported an increase in emergency room visits. 14,15,23 Data for pooled results were extracted from four studies only (out of seven) and showed no significant reduction in the risk of emergency admission between the groups. There was significant heterogeneity (I2 = 82%, P = 0.001).
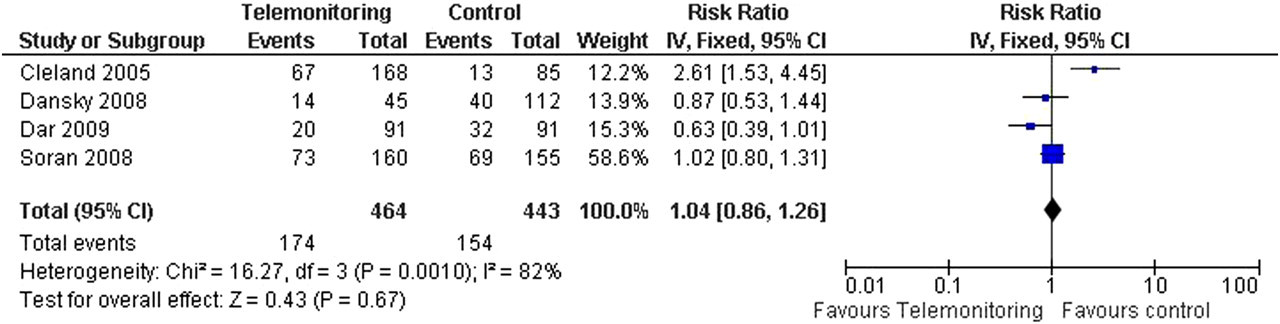
Effect of telemonitoring on all-cause emergency visits
A total of nine studies evaluated the effect of intervention on length of stay in hospital due to exacerbated CHF event and/or any cause hospitalisation among the patients in studies. Out of the nine studies, seven studies reported no difference in hospital length of stay due to the CHF-related hospitalisation or to any-cause hospitalisation 12,15–20 However, two of the nine studies reported a reduction in length of stay among patients in the home monitoring group when hospitalisation due to CHF was evaluated. 7,21
Discussion
The systematic review and meta-analysis permitted rigorous statistical evaluation of the benefits of using telemonitoring compared with usual care. Risk ratios for mortality rates and hospital readmission were calculated for each study to determine the value of telemonitoring.
Hospital admissions
Studies that monitored hospital admissions at different times during the study showed that the risk of admission changes from being in favour of intervention in the earlier stages to having no effect on reducing hospital admissions towards the end. This is consistent with the degenerative nature of CHF and a period of intervention that was similar to the time course of the disease, especially for some studies with an extended intervention period. 24 Therefore, as the length of time with the disease increases, so will the likelihood for treatment and hence hospital visits.
Consequently, the time of comparison can affect the perceived benefit of intervention. Four of the seven studies reported on CHF-related admissions only at the 12-month point. Of these, three reported that intervention at this point was beneficial over usual care in reducing readmissions of patients. The two studies that reported admissions at the six-month interval had opposing conclusions – with risk ratios 0.99 24 and 1.12. 15 One study reported results at 15 months, 14 with a risk ratio of 1.01 (95% Cl: 0.71 to 1.04). This trend in results would indicate that although intervention might have an initial improvement, it does not affect readmission in the long term.
There was no significant difference between the intervention and usual care groups for all-cause hospitalisations.
Mortality
Reduction in mortality was observed in most studies at the endpoint and thus treatment was favoured, with greatest effects being most evident in the larger studies. However, mortality rate varies during the period of a study, and studies did not report mortality rate for common time points. Five studies reported mortality rates for times other than the endpoint. 14,16–18,20 Of these five, only two studies found a reduction in mortality at the earlier point. 14,18 Moreover, in studies where a higher proportion of patients with NYHA class III or IV were recruited, a higher incidence of mortality and hospitalisation was reported. In such cases, normalisation between studies for severity may be required.
Furthermore, two of the studies 14,16 concluded that although mortality was reduced, this was not accompanied by increasing resource utilization. It might be concluded that patients were living for longer and experiencing a better quality of life. Qualitative measures might provide further insight.
Qualitative aspects of the studies
Each paper commented on aspects of the study using qualitative statements in place of quantitative results.
Early detection and feedback
The feedback mechanism of telemonitoring was consistently an important finding. Having early detection of symptoms via daily vital signs permitted medication dose titration specific for the patient at all times through the study period, with inaccurate titration of medicine being seen as one of the causes for worsening cases of CHF. 18,20,24 In addition, hospital admission was planned and managed, and faster discharge was evident; the reassurance of having the telemonitoring system allowed the patient to return home earlier than usual. 15 It is possible that this extra level of organisation and consistency of care could explain user satisfaction and hence medical adherence. The feedback gained by the patient was found to promote self-management. 8 This feedback was especially useful to newly diagnosed patients who were not aware of the symptoms they might encounter and their significance. The feedback was seen to reassure as well as assist in administering the correct dosage of medication. 11
Education and self management
All participants in the intervention groups received training in the use of equipment. 11,16,22 Some studies included specific education for the patients about their disease. 11,13–15,17,18 The effect of the education given to both nurses and patients on the disease was an important finding in the studies. Some studies have promoted self-efficacy behaviours and strategies, with some seeking to reinforce by giving health diaries to patients to record their symptoms as well as behaviours. 15,18,20 For example, vital sign measurements are needed for those newly diagnosed with CHF. However, it is still important to provide education and information on the disease to patients who are in other stages of the disease.
CHF nurses currently spend significant periods of time advising patients on self-management. Eliminating the travel time component by using tele-education could help reduce workload. 19 Furthermore, providing knowledge to the patients allows them to take greater responsibility for their own care and management, increases patient empowerment and can help reduce reliance on the nurse.
Medication adherence
Only three studies out of 11 evaluated the effectiveness of telemonitoring on adherence by patients with their treatment and to medication. Cleland et al. and Goldberg et al. reported no significant difference, whereas Antonicelli et al. reported improved compliance with treatment in the telemonitoring group. 14–16,20
Quality of life
Quality of life of the patients was generally seen to improve when compared to quality of life scores taken at the start of the study. 16 Most studies reported a larger improvement in the intervention group. 14,16,19,20 However some studies evaluating quality of life had no significant data supporting the improvement of health for patients in the intervention arm. 12,14,16–20
In those studies where quality of life scores were not measured directly, other measures indicated a positive effect on the quality of life. The Minnesota Living with Heart Failure (MLHF) and Short Form (SF-36) questionnaire were used in all to measure quality of life. Some studies reported that certain aspects of awareness were improved. For example, Balk et al. reported that knowledge about CHF was significantly higher among patients in the intervention group (P < 0.001). 12 Woodend et al. reported significant differences on the vitality subscale of SF-36 at one month (P = 0.022), three months (P = 0.017) and one year (P = 0.009). 19 Similarly, Wakefield et al. noted that improvement was achieved over time by using the MLHF. 18 Antonicelli et al. reported a significant difference in the health perception score of the SF-36 (P = 0.046). 1 Only two studies assessed anxiety and depression scores. 14,24 Only one study, running for six months, did not find an effect on quality of life. 15
Acceptance of telemonitoring equipment
Six studies determined acceptance of telemonitoring by patients and all showed high levels. Cleland et al. and Soran et al. showed that 96% of patients were highly satisfied and 97% complied with the system. 14,17 In addition, Balk et al. and Dar et al. further observed that age, sex and ethnicity had no effect on use of the equipment and its acceptance. 12,14 Woodend et al. concluded that patients found the technology easy to use. 19
None of the studies reported on acceptance of the technology by the medical professionals involved or their views on its effectiveness in relation to their workload.
Cost
Six studies mentioned a cost-analysis of a telemonitoring intervention versus usual care but provided no breakdown about how the overall cost was estimated. 12–15,18,19 Four of these concluded that costs were reduced in the intervention group, and two studies found no significant difference between the two groups. 12–15,18,19
Limitations of the studies reviewed
Each of the studies identified limitations and observed that these might have affected or biased the results.
Patient recruitment
Several studies were deemed to be too small, i.e. less than 50 patients, to be of statistical significance. Some studies had low patient numbers due to the highly selective inclusion criteria, 20 and seven commented that patient numbers were fewer than originally planned despite strong recruiting efforts being made. 12,14,16,18,20 In some cases the setting of the study gave rise to an unrepresentative population, for example with unbalanced race and ethnicity. 24 This restricts the generalizability of the results, and also excludes the study from meta-analysis.
Generalisation of results was often perceived as a problem in the studies reviewed. For example, in one study, the patients were under the care of organisations with comprehensive CHF management, which might not generally be the case, with hospitals having different protocols. 13 In another study, the ten Home Health Agencies used to recruit patients each adopted a different type of intervention. 23 In another study, the nurse and the patient communicated via a medical service centre, and not directly, potentially weakening the comparison with studies having direct nurse-patient contact. 10
Usual care
The definition of care and usual care varied significantly between studies and this causes difficulties in comparing results. We therefore adopted a definition for a minimum common level of usual care for the purposes of our exclusion criteria to ensure comparability of results. However, significant differences remained. In each case, usual care differed depending on the area, organisation and hospital where the study was conducted, and whether they were a specialist CHF department.
Usual care in the control arm differed when, for example, in two studies, the routine clinical visits were conducted by primary care doctors, with telephone support available by nurses during office hours, 12,15 whereas in two other studies, routine clinical visits were made by specialist nurses. 14,20
In the majority of studies, patients in the control arm continued to receive the same level and type of care, and this was the most popular definition for usual care. In some of the studies usual care consisted of providing extensive information on the disease and educational packs and training to the patient. 16,17 The purpose of this approach was to enable the patient to monitor their own symptoms and have the same level of understanding as patients in the intervention arm and know when they should call upon assistance. This would introduce bias, as psychology theories show that education and knowledge provide benefits by encouraging control and patient self-regulation of their health symptoms. 25 One study therefore provided weighing scales to both the study arm and the control arm, with patients in the control arm being asked to record and monitor their weight, and check against the information provided for anomalous readings, with guidance of when they needed to take action. 17 The remaining studies did not define what constituted usual care in the control arm. 13,18,19,23,24
The differences between both the definition of usual care, and how usual care was carried out, posed limitations in the review. Usual care was used as the control, yet it differed between studies. Certainly the differences between the level of knowledge and involvement of the patient would affect their view of their disease as well as the way they understood their self-management and thus medical adherence. Therefore, the definition of usual care is important to the understanding of the difference between the two groups as well as between studies.
Intervention
Intervention was not the same in all studies, with differences in the type of monitoring. The MOTIVA system (Philips, Enthovan, Netherlands) was considered the most advanced, as it not only collected vital sign readings and sent these trans-telephonically, but also displayed medication reminders, motivational messages, health-related surveys and educational messages via the patient's TV screen. 12 Most studies intended to take daily readings of vital signs. 13,15–18,23 In one study, the monitor was used to administer health-related questions to detect any adverse patient symptoms. 16 However, some studies failed to achieve daily monitoring. 18,23
Differences also existed in the approach to interpreting data and contacting the patient. Generally data was interpreted by the nurses responsible for contacting the patient. However, in one study a medical service centre was used for initial data screening as there were insufficient nurses to make the required three contacts per week. 12
Two studies incorporated videoconferencing as part of the intervention arm, although both encountered problems. In one study, so many of the videoconferencing contacts had technical problems (76%) that eventually the video equipment was abandoned and contact was made instead via telephone. 18 This was also the case in the study by Woodend et al. where problems with the videoconferencing equipment were encountered, leading to greater reliance on the telephone. 19
Conclusion
The meta-analysis showed that telemonitoring can reduce CHF hospital admission over a 12-month period, and this agrees with the results from previous systematic reviews. 7,8,10,26 Our analysis also showed that mortality was reduced, which is again consistent with findings from other systematic reviews. 4–6 We can therefore conclude that patients were living longer without increasing their use of health-care facilities. We believe that our results are stronger than those of previous reviews, as the number of participants in studies previously reviewed was much smaller. 4,5,27
We were unable to perform a quantitative analysis on quality of life. Qualitative analysis of the studies showed that the intervention had a positive effect on the quality of life of the patient. Evidence included the effect of early detection and the feedback mechanism which allows accurate titration of medical dose. Another systematic review found a similar result. 5 The qualitative analysis also showed that hospital admission could be managed, patients could be discharged early, and patients were reassured of close contact.
Some of the studies reported cost reductions in the telemonitoring arm. However none of them provided sufficient information on cost or health benefit to allow analysis of cost-effectiveness or cost-benefit. We note that none of the studies determined the views of the medical professionals or the impact on workload, and we recommend that these should be considered in technology-based interventions.
The studies reviewed reported limitations, particularly with regard to the lack of numbers of patients, and made the general recommendation that further studies with a much larger number of patients would be needed. However, in our meta-analysis, we were able to analyse a sufficiently large cohort to obtain significant results. These showed that intervention patients lived longer, with a reduced amount of time in hospital and an improved quality of life. These are favourable outcomes for CHF patients and support the wider use of telemonitoring.
Footnotes
Acknowledgements
We thank MATCH (Multidisciplinary Assessment Technology Centre for Healthcare) and Brunel University for their support.