
Abstract
A store-and-forward teleconsultation network was developed as a web application in order to provide second opinions on retinal diseases. The system provided automatic notification messages to the referring doctor and the consulted ophthalmologist by mobile phone message (SMS) and email. Images in the electronic medical record (EMR) could be examined in detail using special magnification software. Of the 19 ophthalmologists who agreed to participate, 17 used the teleconsultation network during the pilot trial (89%). During the four-week study period, a total of 52 EMRs containing 82 images were uploaded by the participating ophthalmologists. In 46 cases (89%), a second opinion was provided by the consulted ophthalmologist. Thirty-three of the cases (72%) were related to macular diseases and anti-VEGF (vascular endothelial growth factor) ophthalmology drugs. At the end of the study period, 18 of the participating ophthalmologists evaluated the cases, using a three-point score (poor, good, very good) for Access, Acceptability, Image Quality and Medical Efficacy. Most cases were rated as very good or good for all four variables. Successful use of the network in future will depend on various technical, policy and human factors. The latter is particularly important and appropriate motivations need to be found in order to promote teleconsultations.
Introduction
We have developed a pilot teleconsulation network in ophthalmology for second opinion and follow-up of retinal and macular diseases. The teleconsultation network was based on a Web Application Platform developed with IBM Lotus Notes Database technology. Webpages were developed in English to provide an electronic medical record (EMR) for each case with boxes for patient data, medical history, images and the physician's request for a second opinion (Figure 1). Progressive magnification using a Javascript function facilitated the study of any images in the EMR (Figure 2). Special care was taken to ensure ease of use and user friendliness. The database and applications were stored in a data warehouse in Milan (Datasys Network, IBM Business Partner). This ensured uninterrupted availability and data security.
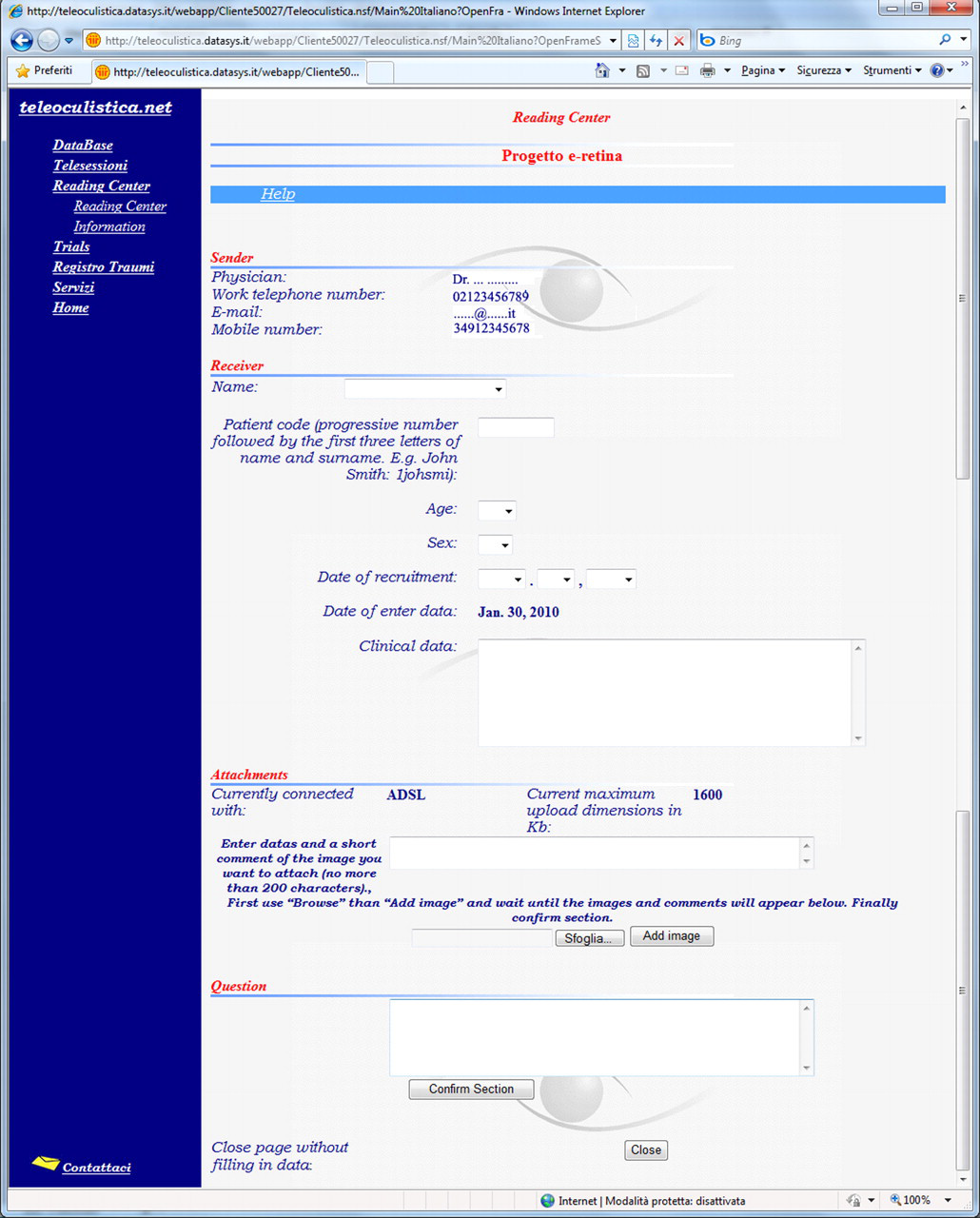
The electronic medical record used in the teleconsultation network
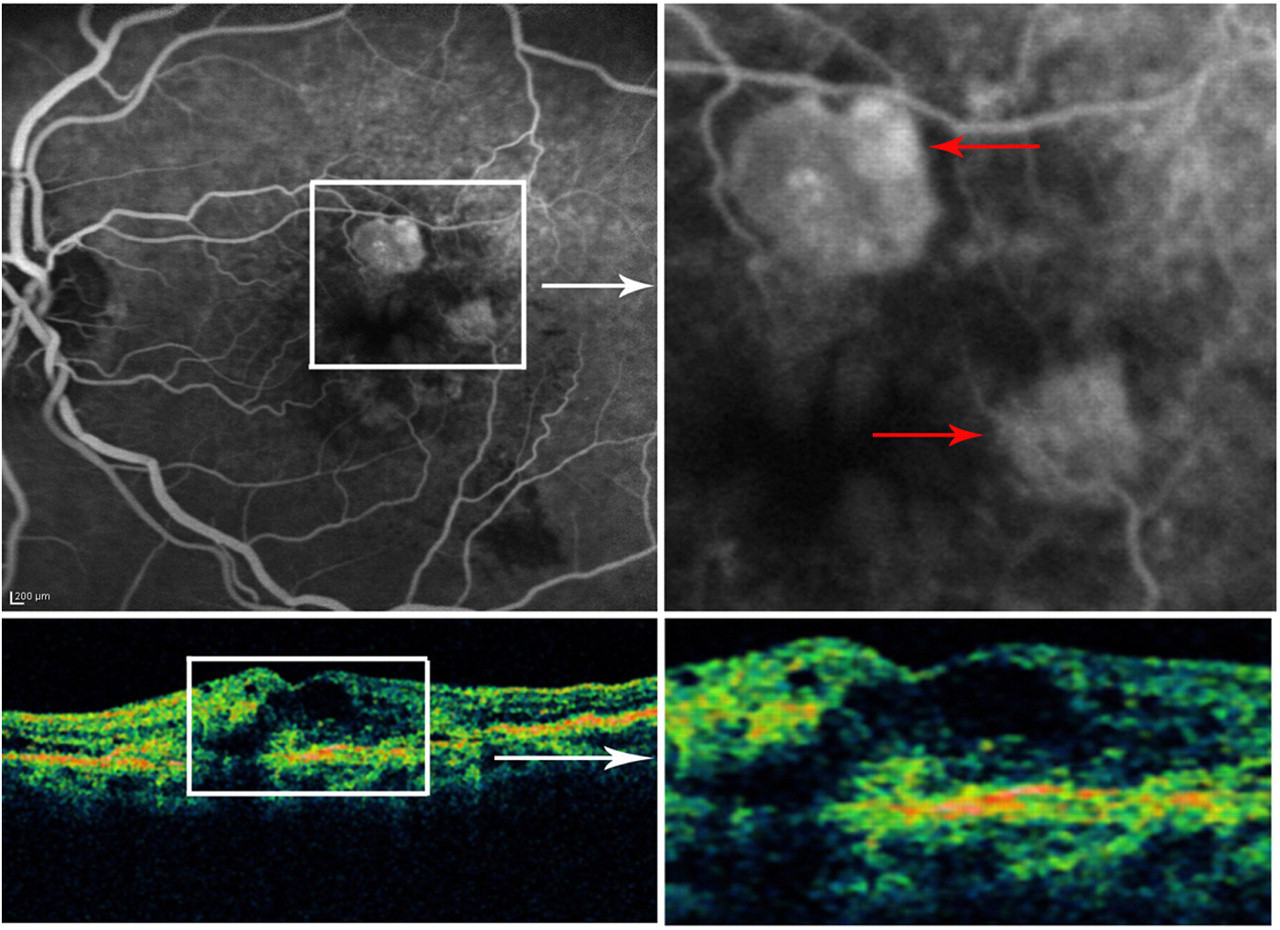
The web-based magnification function allowed detailed study of the images. The upper half of the figure shows fluorescein angiography (top left) with a magnified region (top right). The lower half shows the corresponding optical coherent tomography (bottom left) with its magnified region (bottom right). In this case, pathological neovessels in age-related macular degeneration (arrows) need to be destroyed with anti-VEGF drugs
Using a standard PC, EMRs and images can easily be inserted by ophthalmologists into the main database via the web. The system functions in asynchronous mode (store and forward). When the referring ophthalmologist completes an EMR and requests a second opinion, the consulted ophthalmologist is notified by an automatic mobile phone message and by email; the messages provide a direct link to the website. When the consulted ophthalmologist provides an answer, the consultant ophthalmologist is notified in the same manner.
Privacy and confidentiality for the viewing of medical data were guaranteed by: (1) use of a personal user name and keyword authentication to access the database; (2) use of the patient's initials (rather than their name) together with a sequence number known only by the consultant ophthalmologist to identify the EMR; and (3) permission granted by the patient to request a second opinion.
The aim of the present study was to evaluate the efficacy of teleconsultation for second opinions and follow-up in retinal and macular diseases.
Methods
Once the network was ready, 22 retinal/macular disease specialists working in the region of Varese, a city in the Lombardy region, were invited to take part in the study. A letter about the project was sent to them and 19 of them accepted the invitation. A meeting was then organized to explain the teleconsultation network and to collect the ophthalmologists' data to be used in the system. Following this, the ophthalmologists were able to use the teleconsultation network. Any ophthalmologist, after filling in the EMR, could ask for a second opinion from any of the other 18 ophthalmologists on the panel. The person requesting an opinion made the choice of who to consult. A help desk was available to assist with problems.
Four weeks later all data were collected and another meeting was organized for the participating ophthalmologists. The panel evaluated four variables for each case:
Access to the network (in terms of whether the right care had been provided in a timely manner); Acceptability of the technology; Quality of the images; Medical efficacy (in terms of whether better therapy had been delivered as a result of the teleconsultation).
A three-point classification (poor, good, very good) was used. Ethics permission for the study was not required.
Results
Of the 19 ophthalmologists present at the initial meeting, 17 used the teleconsultation network over the four-week study period (89%). The reasons for non-participation were reported as personal problems with the technology or insufficient time for the project due to work problems. Eighteen ophthalmologists were present at the final meeting.
The number of EMRs inserted into the system increased during the study (Figure 3). Seventeen out of 19 ophthalmologists uploaded clinical data into the teleconsultation network. There was a total of 52 EMRs (an average of 2.7 per ophthalmologist) with a total of 82 images. The mean image size was 645 kBytes (range 57 to 4564). The mean image resolution was 846 × 1386 pixels (range 459 × 422 to 1893 × 1422 pixels). The image format most commonly used was JPEG.

Number of cases handled by the teleconsultation network during the four-week study
In 46 cases (89%) a second opinion was provided by the ophthalmologist who was consulted (Figure 4). Thirty-three out of the 46 (72%) second-opinion requests were for macular diseases and related anti-VEGF (vascular endothelial growth factor) drugs. Six cases did not receive an answer: in four cases the answer was not given because further information was required and in two cases it was due to time being too short to give a satisfactory answer. On one occasion the second opinion arrived after four days, so the referring ophthalmologist decided to prescribe therapy without waiting for the consulted ophthalmologist's answer.
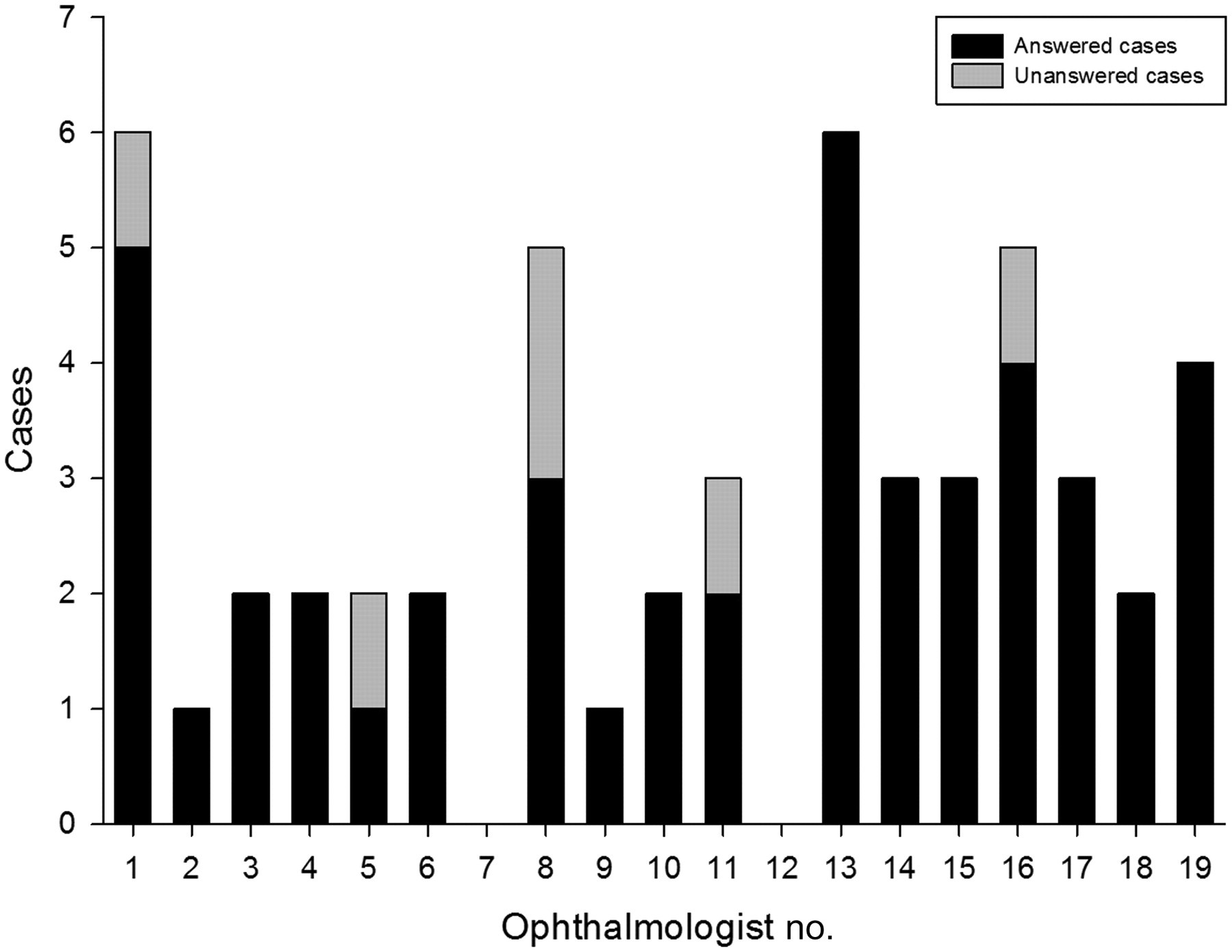
Total number of clinical cases uploaded (y-axis) by each of the 19 ophthalmologist (x-axis) at the time of the final meeting
The most common errors when using the teleconsultation network were incorrect image-file format, repeated uploading and the failure to push the confirm button. Two ophthalmologists were initially unable to upload four images due to their inability to use the system correctly or because of technical problems; all the images were then inserted on the same day with the assistance of the help desk. The help desk assisted ophthalmologists to upload data in a total of seven cases.
In the final audit meeting, ‘Access’ was assessed as very good in 83% of cases. ‘Acceptability’ was assessed as very good in 77% of cases. However, four ophthalmologists admitted that they were not skilled computer users. ‘Image quality’ was assessed as very good in 92% of cases. Some ophthalmologists said it was difficult at times to view the images, probably due to the low quality or low resolution of some of their monitors (Figure 5). Finally, ‘Medical efficacy’ was assessed as very good in 77% of cases (Table 1).

Angiography image correctly viewed (left); same image viewed with an old monitor with resolution of less than 1024 × 768 pixels and an old browser (right). The image quality became even worse using the magnification software
The panel's scores for the four characteristics of the teleconsultation network. The values shown are the percentage of the cases (n = 52) with a given rating
The project provided each of the 17 ophthalmologists with 17 Continuous Medical Education (CME) credits from the Italian National CME Commission through the CME Provider (Aldo Torreggiani, T&C Consulting SRL, Milano, Italy).
Discussion
Based on our experience of tele-ophthalmology, including clinical trials, reading centres and epidemiological registers, 1–3 we created and evaluated a pilot teleconsultation network for the exchange of opinions in ophthalmology. The choice of retinal and macular diseases was dictated by the ophthalmology community's interest in the diagnosis and treatment of these diseases. In fact, most of the requests for a second opinion (72%) were linked to macular diseases and related anti-VEGF drug follow-up. 4,5
In 46 cases (89%), a second opinion was given by the consulted ophthalmologist (Figure 4); we consider this proportion to be high. Most ophthalmologists on the panel submitted cases and most of them responded when asked for an opinion.
The network is a method of utilizing the experience and skills of specialists. The concepts that govern the network are participation, responsibility and transparency. The level of authority and leadership for each participant is based on what they actually contribute to the network itself. 6,7 One of the aims was to ensure that each ophthalmologist on the panel might interact and effectively collaborate with other specialists with the aim of learning from the experiences of others so as to improve professional skills and ultimately assist patients.
The success of a project like this depends on various technical, policy and human factors. For example, the ophthalmologists need a reliable and user-friendly computer to access the teleconsultation network. Difficult, complex teleconsultations might make the physician abandon the project. Fortunately, the acceptability of the system was rated as very good in three-quarters of cases. The help desk was rarely consulted. The policy of involving ophthalmologists from various working environments, with different qualifications, from the same area of northern Italy (university, public and private hospitals, public care centres, private offices), made the results of the project more trustworthy. Finally, the human factor is also of fundamental importance. Most of the ophthalmologists of the panel knew each other, and this was important in creating a group spirit during the initial meeting. Nonetheless, on two occasions the second opinion arrived very late or too late (four days later in one case). In a teleconsultation network the human factor is crucially important. Lack of interest on the part of the physician is likely to produce delays and inefficient teleconsultations. To overcome this barrier, the right motivating factors should be found, such as reimbursement policies and different ways of considering the time necessary for patient care.
In conclusion, we feel that the physician-to-physician teleconsultation network in ophthalmology worked well in the pilot phase. The future use of the network depends on various technical, policy and human factors. The latter is particularly important and appropriate motivations need to be found in order to promote teleconsultations. Telemedicine has the potential to change health care, and to alter conventional physician-to-physician and physician-to-patient relationships.
Footnotes
Acknowledgements
We thank the participating ophthalmologists: Paolo Barosi, Marco Bianchi, Maurizio Chiaravalli, Francesca Contini, Simone Donati (University Hospital); Maria Vittoria Bettini, Anna Corbetta, Maddalena Dugnani, Geraldo Gennari, Gianco Merlo, Davide Misan, Giorgio Francesco Pacelli, Alessandro Penne, Fausto Prandini, Giuseppe Trabucchi (Public Hospitals/Healthcare); and Matteo Dell'Acqua, Claudio Longo, Federico Marcoli (Private Hospitals/Healthcare). We are grateful to Francesco Sicurello, Antonio Speziali, Valerio Tartaglia and Michael John for their assistance. We thank Marco Caraglia and Anna Ponzianelli for their support. The work was funded by an Educational Grant from Novartis Farma S.p.A. Italy.