
Abstract
We compared the use of telemonitoring in patients with chronic obstructive pulmonary disease (COPD) and adult patients with cystic fibrosis (CF). Seventy patients (51 CF and 19 COPD) were enrolled in two studies of six months' duration. Patients used a personal data assistant (PDA) attached to a spirometer to score symptoms and to perform daily spirometry. Criteria for diagnosis of exacerbations of COPD and CF were pre-defined. When exacerbations were detected, patients were offered treatment according to a pre-designed protocol. Thirty-two (63%) CF patients and one (5%) COPD patient withdrew from the studies due to lack of adherence to daily recording. For those who remained in the study, COPD patients recorded more study days (139) than CF patients (113), P = 0.03. The median number of exacerbations detected during the study was greater in COPD than in CF patients, although this was not significant. The median number of device-detected exacerbations in the COPD group was significantly greater than in the CF group, P = 0.024. When compared to a parallel period in the previous year, the number of hospitalisations for COPD exacerbations was reduced, whereas the number of intravenous antibiotics in CF patients did not differ. Adherence to telemonitoring was much greater for COPD than CF patients and the results appear to be more favourable for COPD patients than for CF patients.
Introduction
Telemonitoring has been advocated as a method of monitoring ill health in patients with chronic respiratory disease. 1–2 The aim is the early detection of disease deterioration and the management of acute exacerbations, thus avoiding hospitalisation. Daily monitoring has long been performed using a paper diary in patients with chronic obstructive pulmonary disease (COPD) 3–4 and cystic fibrosis (CF). 5–6 The problem with this approach is that exacerbations can only be diagnosed retrospectively upon receiving the diaries. For the timely management of exacerbations, communication systems that allow reporting of symptoms and lung function tests that can be visualised by clinicians in realtime have been suggested. 7
We have recently completed two prospective feasibility studies in patients with COPD 8 and CF. 9 The two studies had similar entry criteria, methods of recording and outcome measures. However, the rate of technology utilisation by patients and the dropout from the studies were markedly different. We have examined the similarities and differences between COPD and CF patients for daily recording and the effects on diagnosis of exacerbations and hospitalisation rates.
Methods
The telemonitoring device (Figure 1) was based on a mobile-enabled personal digital assistant (PDA). 8–9 The PDA could be attached to a handheld spirometer (Vitalograph, Buckinghamshire, UK) with a special cable (E-san Ltd, Oxford, UK). Two software packages written by E-san were installed on the PDA, which allowed patients to access and enter data for their symptoms and spirometry.
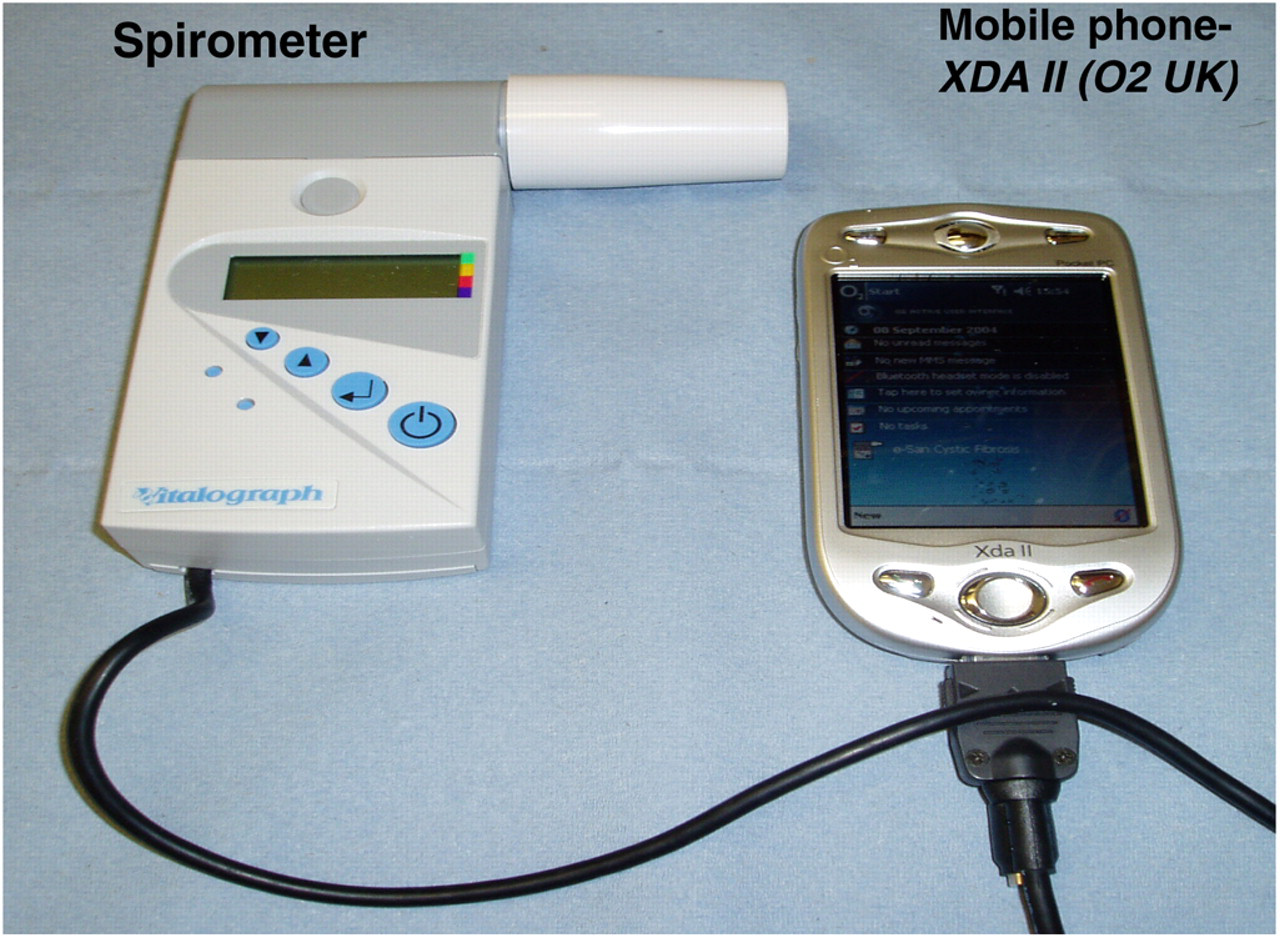
The telemonitoring device: a mobile-enabled PDA with an attached spirometer
All patients were trained in how to use the handheld spirometer and nose clips. During the two studies, research teams were available for clinical support and a technical helpline was available for solving technical problems.
Design of studies
The two studies were prospective of six months' duration. Patients were asked to record their symptoms and spirometry once per day in the evening. For the COPD group, the symptom score was graded on a five-point scale for each symptom, whereas for CF patients the score was graded on a four-point scale (Tables 1 and 2).
Symptom questionnaire for the COPD group. Each symptom was scored on a scale from 1 (less symptoms) to 5 (more symptoms)
Symptom questionnaire for the CF Group. Each symptom was scored on a scale from 1 (less symptoms) to 4 (more symptoms)
As COPD patients were treated for exacerbations in primary care (by their family doctor) as well as secondary care (hospital), patients were asked if they had visited a medical professional that day (Yes/No) and if they had a medication change that day (Yes/No). A similar question was not necessary for the CF patients because their care was only provided in hospital where reliable records were held.
For spirometry, the individual highest reproducible FEV1 of three attempts was selected. After recording FEV1, the information was sent to the research centre where it was read immediately.
Reading and managing symptoms
A time-score plot was designed for each patient. Each symptom score and the best FEV1 value were plotted daily (Figure 2).
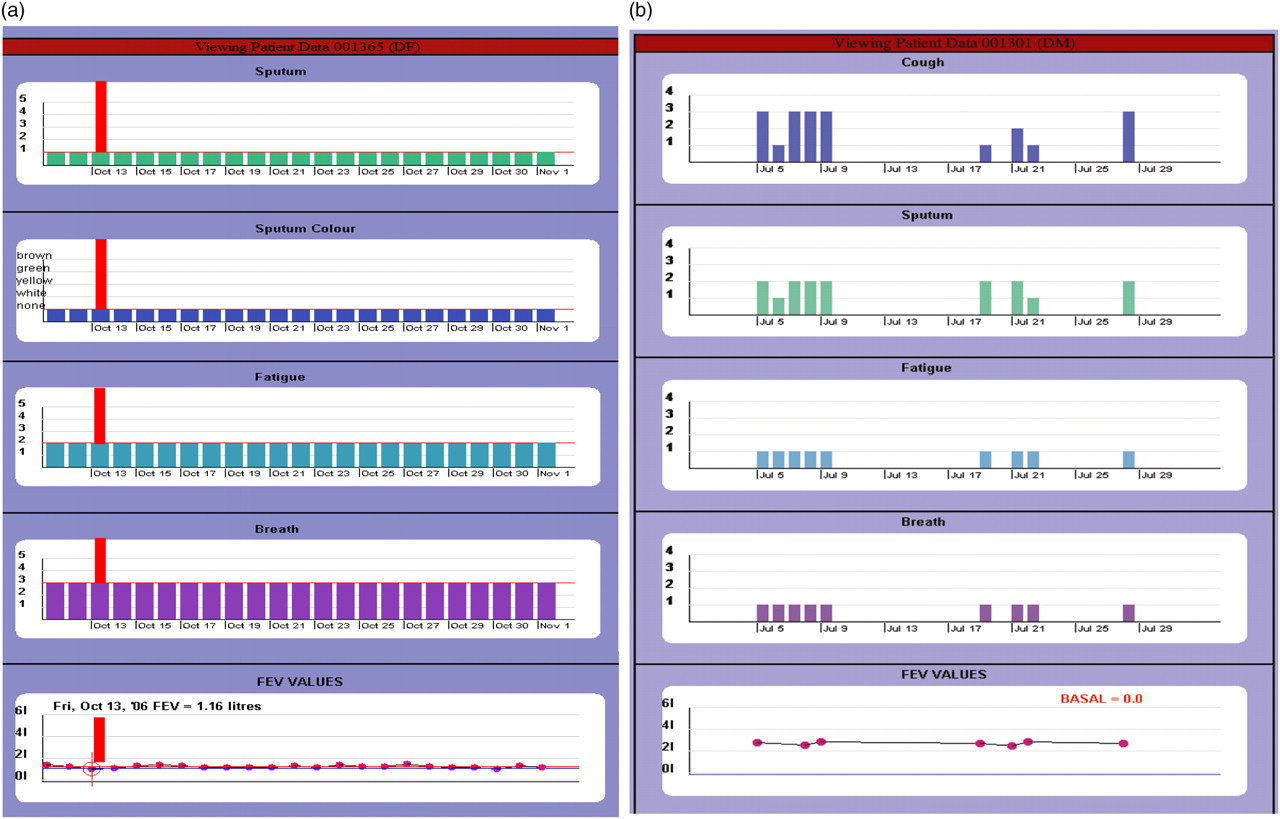
Time-symptom graphs. The vertical column is the score for each symptom. The bottom panel is the FEV1. For each day, one column score and one corresponding value for FEV1 is recorded. (a) (left hand panels): a recording from a COPD patient showing an exacerbation detected by reduced FEV1 but not in increase in symptom scores. The horizontal line (colour coded to differentiate between symptoms and FEV1) is the baseline. (b) (right hand panels): a recording from a CF patient who was withdrawn from the study due to lack of recording
To establish a baseline of symptoms and FEV1 all patients entered an exacerbation-free run-in period of 14 days where they recorded symptom score and lung function as described above. Baseline values were the median symptom score and the mean FEV1 value recorded during the 14-day run-in period. If an exacerbation occurred during this period, the run-in period was re-started 14 days later. Patients who had two exacerbations during the run-in period were excluded from the study. Once the run-in period was successfully completed, the baseline automatically appeared on the patient's time-score plot and the patient entered the study.
Recordings of all patients were viewed each day by members of the research team. When an exacerbation was detected, action differed between the two groups. The COPD patients were asked by telephone to take a pre-provided standby treatment, and patients with CF were invited to the hospital and were treated by either oral or intravenous (IV) antibiotics according to the severity of exacerbation.
When data were not sent for two successive days, the research team contacted the patient by telephone to remind them and/or to offer assistance (through the technical team) if applicable.
Acute exacerbations
Acute exacerbations were defined differently in the two groups.
Acute COPD exacerbation was regarded as being present if at least one of the following was encountered:
An increase of at least one degree of two symptom scores and/or a decline in FEV1 ≥10% from baseline for ≥2 successive days. The increase in two symptoms over two days was chosen in accordance with previous studies which used this definition.
3–10
A patient presenting with symptoms they felt to be those of acute exacerbation and seeking help that resulted in them being given a course of antibiotics and/or prednisolone.
When an exacerbation was detected a vertical red line appeared automatically on the plotting screen for ease of reference (Figure 2). On detecting an exacerbation, one of the researchers would contact the patient and advise them to start treatment with medications that were pre-provided.
Acute CF exacerbation was defined as a worsening of three symptoms or a decline in FEV1 for three successive days. This was based on the definition of exacerbation produced in a consensus document by the US CF Foundation which was later summarised in two reports by Fuchs et al.
11 and Ramsey et al.
12
An exacerbation was regarded as having occurred if one of the following criteria was met:
An increase of at least one degree of three symptom scores over three successive days; A decline of at least 10% in FEV1 alone for three successive days; An increase of at least one degree of two symptoms and a decline in FEV1 of equal to or more than 10% for three successive days.
CF exacerbations were also regarded as being present when a patient presented with symptoms that they recognised to be those of exacerbations even if their diary recording did not meet any of the three previous criteria.
On detecting a CF exacerbation, patients were invited to hospital and therapeutic decisions were made by a consensus between them and their clinicians. Options of management were to treat with oral antibiotics, with IV antibiotics or to monitor the symptoms. Standby courses of antibiotics were not routinely provided for this group.
Patients who presented with symptoms of exacerbations not detected by the device were evaluated and treated in the same way as above.
COPD group
Patients were included from respiratory outpatient clinics at Bristol Royal Infirmary. The inclusion criteria were: diagnosis of COPD; aged 40 years or over; more than 10 pack-years of cigarette smoking (one pack-year is the consumption of one pack per day for one year); FEV1 <80% predicted; FEV1/FVC <70%; and free from COPD exacerbations for two weeks prior to entering the study. Patients who had a diagnosis of asthma or bronchiectasis or had any co-morbidity serious enough to shorten life to less than one year or had undergone lung surgery were excluded. Patients living outside the mobile phone network area and/or who had a significant cognitive problem were also excluded.
Hospitalisations were compared with the same six months in the previous year. The total number of exacerbations could not be compared with the previous year because most of these exacerbations were diagnosed and treated by the patients' general practitioners (family doctors) and reliable data could not be obtained easily.
CF group
Patients were invited from the adult and paediatric CF units at the University Hospital, Bristol. CF patients were included in the study if they were aged 12 years or over with FEV1 below 80% predicted values. Exclusion criteria were patients living outside the mobile phone network area, terminally ill patients or patients on the lung transplant waiting list.
The number of CF exacerbations requiring intravenous antibiotics during the six-month study period for each patient was compared with the same six months in the previous year. All of the CF patients that participated were being treated in hospital (where their case notes were available). Reasons for not comparing hospitalisation rates in the CF groups are discussed below.
For both COPD and CF patients, withdrawal criteria were: inability of patients to record for more than 60% (8 days) of the run-in period or failure to record for two successive weeks despite reminders from the research team. Both studies were approved by the appropriate ethics committee.
Statistical analysis
Comparisons between the two groups for age and baseline FEV1 were made using two-sided t-tests. The average days of recording and number of exacerbations of the COPD and CF groups were compared using the Mann-Whitney U test. Comparing the number of hospitalisations for COPD patients in the year of the study with the previous year was made using Wilcoxon matched pair tests. The same test was used to compare the number of IV antibiotics between the year of the study and the previous year in CF patients.
The number of patients recruited in each group out of those who were screened and the number of patients who were withdrawn from the study in each group were compared using contingency tables using chi-squared tests and relative risk values.
Results
From 2004–2007, a total of 89 patients were screened (67 CF and 22 COPD). Out of those, 70 patients (51 CF and 19 COPD) were enrolled. Patients with COPD were older and had worse FEV1 than CF patients (Table 3).
Demographic data
The rate of withdrawal and the number of study days not recorded by patients were greater in CF than in COPD patients (Table 4). A total of 32 (63%) CF patients and one (5%) COPD patient were withdrawn from the study due to lack of adherence; this difference was significant (P < 0.0001).
Outcome of the study
*X 2 = 18.4, relative risk = 0.53, 95% confidence interval = 0.38–0.72
For those who remained in the study, CF patients recorded an average of 113 days (63% of total study days) compared to 139 days (77%) for COPD; this difference was significant (P = 0.03) (see Table 4 and Figure 3).

The number of days recorded in the two groups. The boundary of the box closest to zero indicates the 25th percentile, a line within the box marks the median, and the boundary of the box farthest from zero indicates the 75th percentile. Whiskers (error bars) above and below the box indicate the 90th and 10th percentiles
The median number of exacerbations detected during the study was greater in COPD than in CF patients although this was not significant. The median number of device-detected exacerbations in the COPD group was significantly greater than in the CF group (P = 0.024) (see Table 4 and Figure 4).
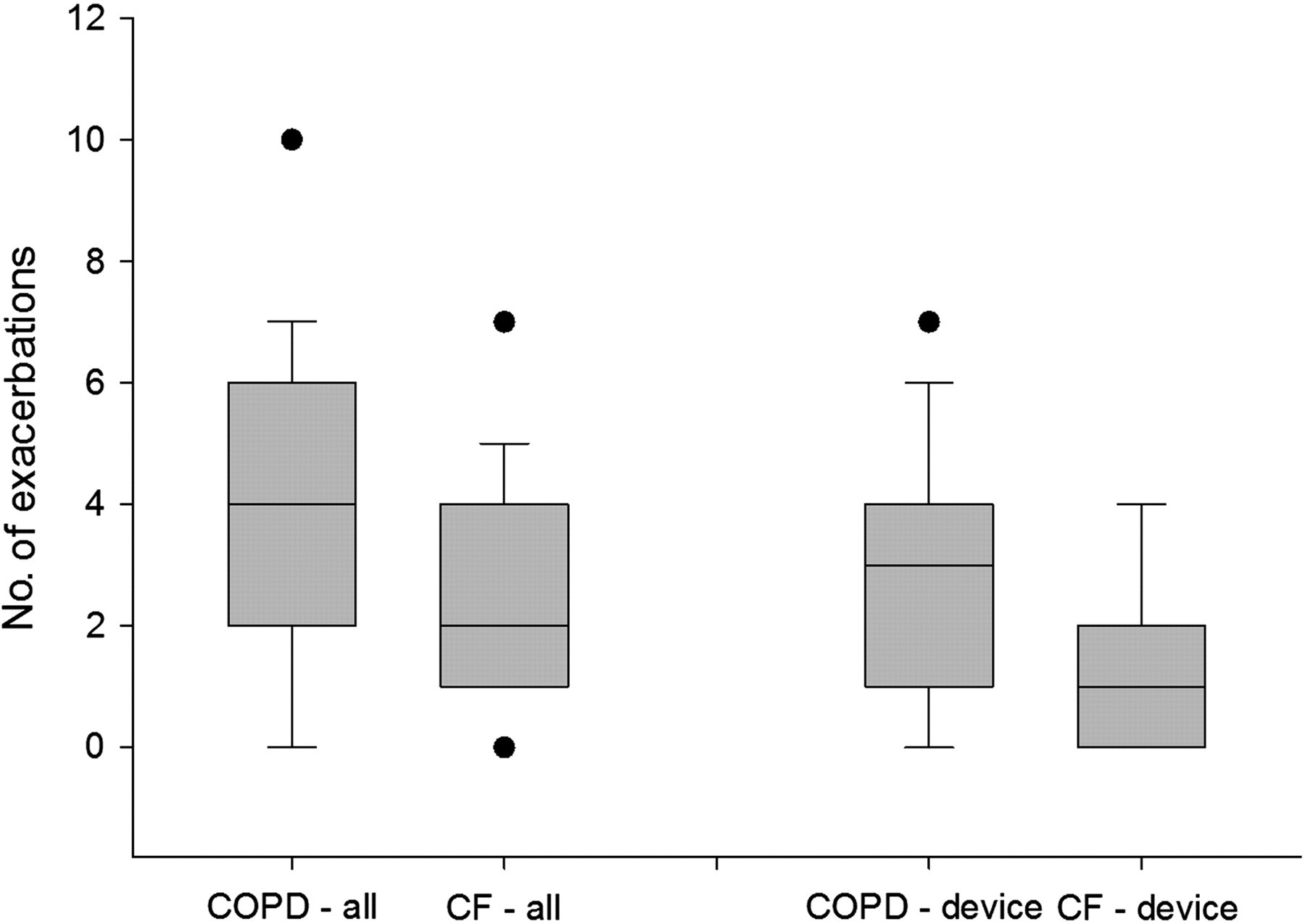
The number of all exacerbations (left) and device-detected exacerbations (right) in patients with COPD and CF. The boundary of the box closest to zero indicates the 25th percentile, a line within the box marks the median, and the boundary of the box farthest from zero indicates the 75th percentile. Whiskers (error bars) above and below the box indicate the 90th and 10th percentiles
The number of hospitalisations in COPD in the six months of the study was significantly reduced compared to the same six months in the previous year. There were six hospitalisations (0.33 per patient) due to acute exacerbation of COPD compared to 14 (0.78 per patient) in the same six months in the previous year, P = 0.027. For CF patients there was no difference in the number of exacerbations requiring intravenous antibiotics in the study year (26 episodes) compared to the previous year (22 episodes).
Discussion
The present study demonstrates differences in the degree of utilisation of telemonitoring by patients. Contrary to our expectations, COPD patients were more likely to remain in the study and recorded more days than CF patients. The difference in the staff involved in the two studies was not likely to have played a significant role in the differences in utilisation and other outcome measures.
The technical difficulties were mainly of two types: the device was slow to send the recorded data or the device could not re-initialise after running out of power. The technical team provided telephone instructions on how to deal with these problems. Both problems were encountered throughout the two studies and we do not believe that technical difficulties account for the higher withdrawal from the study in CF patients compared to COPD patients. CF patients, however, were more likely to stop recording because of this. They were less likely to respond to the reminders of the research team and to seek help from the technical team and, therefore, more likely to drop out of the study.
Formal qualitative interviews with patients would have been valuable, but were not conducted. Nevertheless, our impression is that no single factor explains the results of the study. The difference in adherence may not be a reflection on telemonitoring itself. Rather, it may be that young CF patients are less likely to adhere to any type of daily discipline. Daily monitoring may be more acceptable to older COPD patients with a less busy lifestyle. For CF patients, lack of adherence to daily treatment such as intake of pancreatic enzymes, daily physiotherapy, nebulised agents and insulin are well documented. 13–15
There was no difference in the total number of exacerbations diagnosed in the two groups, whereas the number of device-detected exacerbations was greater in COPD than in CF patients. There are three possible reasons for this. First, the definition of exacerbation was more stringent in CF than in COPD patients. Second, COPD patients had lower FEV1 than CF patients, which is a known risk factor for acute exacerbations. 16–17 Third, the greater number of days recorded by COPD patients compared to CF patients allowed the device to detect more exacerbations according to our pre-defined criteria.
Due to the large number of CF patients who were withdrawn from the study, we compared basic characteristics of patients who remained in the study with those who dropped out. 9 The two groups were matched with respect to age, gender, disease severity and the prevalence of CF-related complications.
Provision of IV antibiotics as a marker for CF exacerbation severity was compared in the study year compared to a parallel period in the previous year. This was done instead of comparing hospitalisations for CF exacerbations. Factors affecting site of management of CF exacerbations (hospital or home) have been comprehensively reviewed. 18 In short, the reasons for choosing site of treatment are built into the way that CF exacerbations are managed in the UK. Most exacerbations (even severe ones) are not treated in hospital. Hospitalisation for CF patients during exacerbation often occurred due to lack of social support at home, inability to comply with self-administration of antibiotics and patients' own choice.
For COPD, care is less cohesive and is spread across primary care (family practices) and secondary care (hospitals). Most COPD mild to moderate exacerbations are treated in primary care. Only patients with severe exacerbations and particularly those needing intravenous administration of antibiotics are treated in hospital.
There were no control groups in the two studies because they were feasibility studies. Instead, we used outcome measures in the same six-month period in the year prior to the study as comparators. So the observations outlined in the present study may suffer from the drawbacks of cohort research. This is not unique to trials of telemonitoring in pulmonary medicine. In a comprehensive review of telemonitoring, Paré et al. reported that, unlike studies in diabetes, most published studies in pulmonary disease were not randomised and did not include control groups. Nevertheless, the effect of this intervention appears to be more prominent in pulmonary disease than in diabetes. 19 Consequently, newer prospective studies in COPD have randomised patients' entry and include a control arm. 20 Most reported studies in respiratory medicine suggest that patients are in favour of the technology. 21
We propose that telemonitoring should be used as an additional tool to inform the work of teams rather than a de novo method. The way the technique is applied needs to take into account the structure of the health system for every respiratory disease. Telemonitoring is likely to be most helpful for selected adherent patients at times of clinical deterioration and frequent exacerbations. Identifying the trigger points for intervention for different patients could prevent the need for aggressive treatment, including hospitalisations, and could ultimately improve patient outcomes.
Footnotes
Acknowledgements
We thank Professor Lionel Tarrasenco, Keith Ralph, Mark Larson, Neil Townsend and the technical teams in E-san and t+ Medical for their help. We are grateful to Mrs Rosemary Greenwood for assistance with the statistical analysis. The work was supported by grants from O2 Telecommunication UK and David Telling Charitable Trustees, Bristol.