
Abstract
We compared the effectiveness of home telerehabilitation with conventional rehabilitation following knee replacement surgery (total knee arthroplasty, TKA). Forty-eight patients (mean age 66 years) who received TKA were recruited prior to discharge from hospital after surgery and were randomly assigned to telerehabilitation or usual care. Telerehabilitation sessions (16 per participant over two months) were conducted by trained physiotherapists using videoconferencing to the patient's home via an Internet connection (512 kbit/s upload speed). Disability and function were measured using standardized outcome measures in face-to-face evaluations at three times (prior to and at the end of treatment, and four months after the end of treatment). Clinical outcomes improved significantly for all subjects in both groups between endpoints. Some variables showed larger improvements in the usual care group two months post-discharge from therapy than in the telerehabilitation group. Home telerehabilitation is at least as effective as usual care, and has the potential to increase access to therapy in areas with high speed Internet services.
Introduction
Physical rehabilitation is an important factor in the recovery of patients following total knee arthroplasty (TKA). Rehabilitation generally begins in the hospital, 1,2 and continues after discharge, both at home and in outpatient clinics. 3 Demand for home care and outpatient clinics is increasing and is difficult to meet, especially in rural areas. Telerehabilitation is an alternative to conventional face-to-face therapy and home telerehabilitation may facilitate the delivery of rehabilitation services to people who cannot access them. 4 Clinical care that can be provided via home telerehabilitation encompasses active treatment and follow-up, 5 rather than diagnosis and evaluation by teleconsultation.
Published studies on telerehabilitation have been limited to patient assessments using videoconferencing between two clinics. 6–9 In TKA, a pilot study documented the efficacy of telerehabilitation in terms of both physical and functional objective outcome measures on 21 patients. 10 The physical and functional improvements in the telerehabilitation group were similar to those in the control group. There was a non-significant trend for greater improvements in the telerehabilitation group for most outcome measurements. The study provided evidence for the efficacy of low-bandwidth telerehabilitation consultations. The experience of clinical physiotherapists and participants who received treatment via telerehabilitation was also examined. 11 High levels of satisfaction were reported by participants. The service was found to be effective, safe and easy to use, and it integrated well into current clinical practice. The study demonstrated the potential for delivering physiotherapy services via low-bandwidth Internet connections. In the same way, other pilot studies have demonstrated similar trends for TKA telerehabilitation. 12,13
While home telerehabilitation for post-knee arthroplasty seems to be practicable for patients discharged from hospital, 12,13 there is no evidence that it is effective. The purpose of the present study was to investigate the clinical efficacy of telerehabilitation at home for patients following discharge from hospital after TKA.
Methods
Patients who had TKA were recruited prior to discharge from two acute care hospitals, the University Hospital of Sherbrooke (UHS) and the University Hospital of Quebec (UHQ). These hospitals provide orthopaedic services for a metropolitan (Quebec City and region) and an urban (Sherbrooke and region) area of Quebec. The study was approved by the appropriate ethics committee.
Recruitment and randomization
The design was a randomized controlled trial. Potential participants were first approached by their hospital physiotherapist in the post-operative unit to determine their interest in the research project. With the candidate's permission, the availability of high speed Internet access at their home was checked. If high speed broadband access was potentially available, the candidate's informed consent to participate in the study was obtained. The participants were then randomly assigned to the telerehabilitation group (experimental group) or home care/outpatient clinic group (control group). Randomization was done by a random number generator with sealed envelopes.
For the experimental group, high speed Internet access was made available to each home within five days of the subject's discharge from the hospital. A research assistant went to the patient's home to install the telerehabilitation equipment and test the quality of the Internet connection. It took about one hour to complete this procedure. The telerehabilitation equipment was collected by the research team at the end of the planned telerehabilitation period (two months). Control group participants were referred by the institution to the usual home care services.
Telerehabilitation equipment
The telerehabilitation equipment was based on that used in previous studies. 12,13 It consisted of videoconferencing CODECs (550 MXP, Tandberg) with remote-controlled cameras, 50 cm LCD screens and associated software for user-friendly control. 14 The equipment was developed to ensure that interactions between clinicians and patients during the telerehabilitation sessions were not impeded by technology, see Figure 1. A mouse-based interface allowed intuitive control of the camera functions at both sites.

Screenshot (from the clinician's unit) of typical rehabilitation exercises
Outcome measures
The outcome measures chosen to assess changes following TKA post-surgery rehabilitation were:
Disabilities: range of motion was measured by goniometry, balance was measured by the Berg balance scale
15–17
and lower body strength was measured by the 30-s chair-stand test;
18
Function: knee function was measured by WOMAC,
19
locomotor performance in walking was measured with the Timed Up and Go test
20
and the Tinetti test,
21
and functional autonomy was measured with the Functional Autonomy Measurement System (SMAF).
22
These variables were measured at the beginning (T1) and at the end (T2) of the experimental intervention, and four months afterwards (T3).
Quality of life was measured using the SF-36, 23 at the beginning (T1) and at the end (T3) of the study.
Physiotherapy
The physiotherapy for all participants was designed for functional rehabilitation. It was based on reducing disabilities and improving function in daily activities through progressive exercises. The mean duration of each therapy session was about one hour (including treatment assessment and recommendations between treatments). The teletreatments were delivered at a rate of two sessions per week for eight weeks (i.e. a total of 16 sessions). The home visit/outpatient clinic treatments were delivered as usual over a period of about two months.
For the experimental group, someone was expected to be at the participant's home during teletreatment to ensure the patient's safety during transfers and locomotion, and in case of emergency. This person was a family member or friend who had received prior training in the use of the technology that had been installed, but not on the therapy.
Data collection procedures
For both groups, an appointment was made with each subject by the independent clinical evaluator to take the clinical measurements in the first week after returning home from hospital (T1). All other assessments were done at the research centre: in the week following the end of the therapy (T2) and two months after the end of therapy (T3). Assessments were conducted by a trained research assistant at each hospital.
Statistical analysis
To examine the effect of the physiotherapy itself (administered to both groups), the intra-group difference was tested using a Wilcoxon test for two related samples. To examine the effect of telemedicine, the inter-group difference was tested with a Mann-Whitney test for two independent samples. The group-time interaction was examined using a Mann-Whitney test for two independent samples.
Results
Following randomization, there were 24 patients in each group. In the experimental group, three participants were lost during follow-up: one left immediately after the randomization and two were excluded by medical decision (vagal shock and unknown reason). In the control group, three decided to leave the study immediately after the randomization (they had expressed a preference for being in the experimental group) and one had surgery for an aneurysm in the leg. Analyses were conducted on 41 participants. There were no differences at baseline between the two groups on variables potentially related to the outcome: age, weight, height, schooling and number of hospitalized days after their surgery (Table 1).
Patient characteristics at baseline
*Mann-Whitney test for two independent samples
Effect of physiotherapy
In each group, clinical efficacy at the end of treatment was compared to the pre-treatment assessment (T2-T1). As expected, there were significant improvements in all clinical variables, see for example Figures 2 and 3.
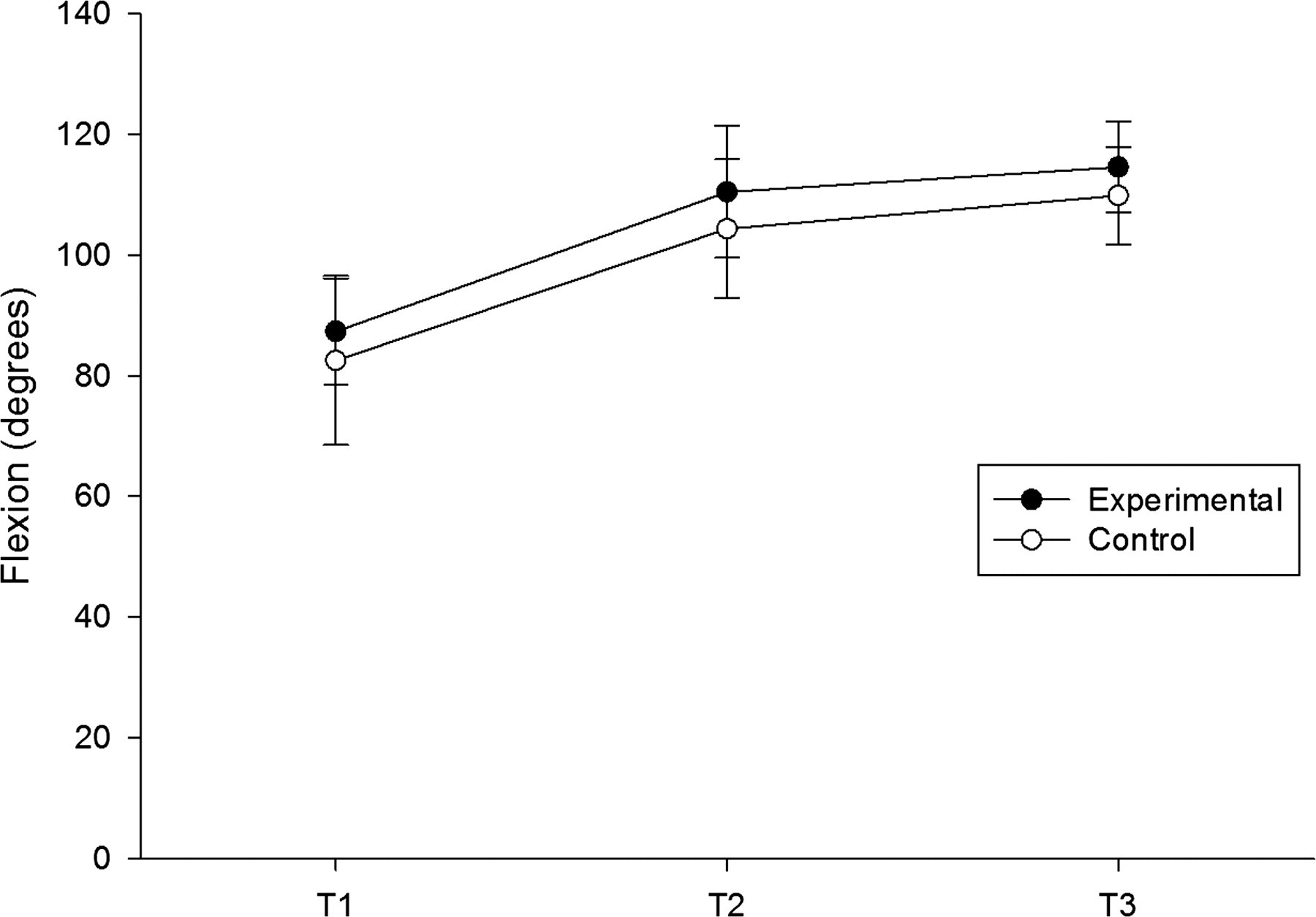
Joint range of motion – flexion

Joint range of motion – extension
Some variables continued to improve after T2. For example, joint range of motion continued to improve in both groups for flexion, but only in the control group for extension (a difference of 1.1°). The same pattern of differential improvements in the control group was observed for the Berg test (a difference of 1.6 points), the 30-s chair-stand test (a difference of 0.9 repetitions), the SMAF (a difference of 1.2 points) and the total score of the WOMAC (a difference of 8.1 points). With the exception of the total score of the WOMAC, these differences were not clinically significant. However, participants from the control group showed more improvement than the experimental group in functional activities (e.g. climbing stairs, walking) between T2 and T3 (WOMAC difficulty section, P = 0.047).
A comparison between T1 and T3 showed that participants from the control group had better physical functioning (P = 0.019) and less bodily pain (P = 0.013) two months after the end of treatment compared to before treatment.
Effect of telemedicine
There was no intergroup difference between the telerehabilitation and conventional rehabilitation at T1 and T2, meaning that the participants improved equally in both groups. Moreover, the group × time interaction showed no difference between T2 and T1 for both groups. Thus there was no differential effect between the experimental and control groups between T2 and T1.
Discussion
The results of the trial suggest that home telerehabilitation is as effective as usual care in reducing disability (range of motion, balance and muscle strength) and improving function (knee function, walking and autonomy) after two months of treatment. These results are similar to those of a previous pilot study on TKA telerehabilitation. 10
However, our results show that the improvement two months after the end of treatment in some variables was larger in the control group than in the experimental group. This tendency was also noted for the general health status. Interpretation of this differential improvement in the control group is difficult to explain. One factor could be the follow-up instructions given by physiotherapists when they discharged the participants at the end of therapy: were the instructions similar for both groups? Further research is required. However, our study confirmed that home telerehabilitation is an effective way of providing physical rehabilitation following TKA and suggests that it is as effective as usual care, at least in the short term.
The internal validity of the study could have been affected by certain biases. First, there is the question of selection. A comparison of surgery lists for patients for knee arthroplasty and participants referred to the study showed that less than half of the patients were referred to the research team by physiotherapists. Therefore, we cannot exclude a selection bias.
The variables potentially related to the study outcomes were controlled by the randomization: age, height/weight and length of stay in hospital after the surgery. This avoided confounding factors. Overall, the standardization efforts and the choice of instruments ensured good internal validity.
The present study suggests that telerehabilitation is a practical alternative to home visits by a physiotherapist for delivering rehabilitation services. This new delivery method appears acceptable to patients, although both must modify their expectations. In our study there was sufficient bandwidth available to make home telerehabilitation feasible. The next step will be to conduct controlled trials to measure the cost-effectiveness of the two treatment alternatives.
Footnotes
Acknowledgements
We thank all patients for their contribution in this project. The research was supported in part by a grant from the Fonds de la Recherche en Santé du Québec.