
Abstract
We conducted a systematic review of the applications and technical features of digital interactive television (DITV) in the health and social care fields. The Web of Knowledge and IEEE Xplore databases were searched for articles published between January 2000 and March 2010 which related to DITV systems facilitating the communication of information to/from an individual's home with either a health or social care application. Out of 1679 articles retrieved, 42 met the inclusion criteria and were selected for review. An additional 20 articles were obtained from online grey literature sources. Twenty-five DITV systems operating in health and social care were identified, including seven commercial systems. The most common applications were related to health care, such as vital signs monitoring (68% of systems) and health information or advice (56% of systems). The most common technical features of DITV systems were two-way communication (88%), medical peripherals (68%), on-screen messaging (48%) and video communication (36%). Digital interactive television has the potential to deliver health and social care to people in their own homes. However, the requirement for a high-bandwidth communications infrastructure, the usability of the systems, their level of personalisation and the lack of evidence regarding clinical and cost-effectiveness will all need to be addressed if this approach is to flourish.
Introduction
An ageing population and rising quality of life expectations are likely to place greater demands on health and care services to support older and vulnerable people to live in their own homes. The European Commission has advocated the proper use of Information and Communication Technologies (ICT) as one way of achieving this. 1 Digital interactive television (DITV) is a potentially useful technology for health care. In the UK, there are 60 million television sets and 90% of households have digital television. 2 By 2012, the television signals in all EU countries will have switched from analogue to digital. 3 This is facilitating the development of DITV services, such as Internet Protocol television (IPTV). Consequently, there is likely to be a movement from conventional public broadcasting towards individual, on-demand access to interactive services.
Advances in television-based services and changes in care provision offer the potential to provide new ways to access health and care services. They may also offer new opportunities for social interaction for vulnerable members of society who are isolated and/or hard to reach. Older people, in particular, may benefit from new television-based services as they are the heaviest consumers of television programmes, averaging 5¼ hours viewing per day. 4
We have reviewed existing and developing DITV systems to identify their health and social applications, and technical features.
Methods
A systematic literature review was conducted. Two online bibliographic database search engines, Web of Knowledge (WoK) and IEEE Xplore, were searched using the same strategy (Table 1). Keywords for digital interactive television were combined with keywords relating to health or social terms. The search was limited to the period January 2000 to March 2010.
Search terms
Articles that described a DITV system which facilitated the communication of information to or from an individual's home with either a health or social care application were included. For the present review, health care was defined as ‘services provided to individuals for or in connection with the prevention, diagnosis or treatment of illness, and the promotion and protection of public health’. 5 A social care application was defined as any service that supports people to maintain their independence, enables them to play a fuller part in society, protects them in vulnerable situations and helps them to manage complex relationships. 6 Social care was interpreted in its widest sense to include traditional social care services (e.g. practical support to help vulnerable people maintain their independence) but also services to promote and support social interaction and engagement. Articles were excluded for any of the following reasons: non-English language; general reviews; technical articles without a described health or social application; articles about the usability of a system DITV component (e.g. remote controls); systems using television only as a display for a different system (e.g. a videoconferencing system); and articles about television programmes, e-commerce, mobile TV, electronic programme guides or pedagogy applications. Duplicate articles were also excluded.
One reviewer screened the titles and abstracts of articles retrieved from the database search. Relevant articles were selected according to the exclusion criteria. Following this, two reviewers agreed which of the selected articles should be included and disagreements were resolved by consensus. The full texts were obtained for further review and data extraction.
Online grey literature sources, such as Google Scholar and the websites of academic departments and commercial organisations, were also searched. Articles of interest were selected using the same inclusion/exclusion criteria. A data extraction sheet was created with the following areas: (1) the general characteristics of the identified DITV systems (name and country of origin); (2) the applications; and (3) the technical features. The application was defined as the end-use of a DITV system. A technical feature was defined as the specific hardware or software component of a DITV system which supports the application.
Results
In total, 1894 articles were identified from the academic databases. There were 721 and 1173 articles from the WoK and IEEE Xplore databases, respectively. Of these, 215 were duplicates, leaving 1679 unique articles. The review stages are summarized in Figure 1. The full texts of 57 articles were retrieved and reviewed. Of these, 15 were excluded for the following reasons: technical paper with no defined application (n = 6); standalone technology with no communication to/from the user's home (i.e. television used as a display only) (n = 4); e-commerce only (n = 3); usability study of the interface only (n = 2). Information was extracted from the remaining 42 academic articles and a further 20 articles were identified from grey literature sources.
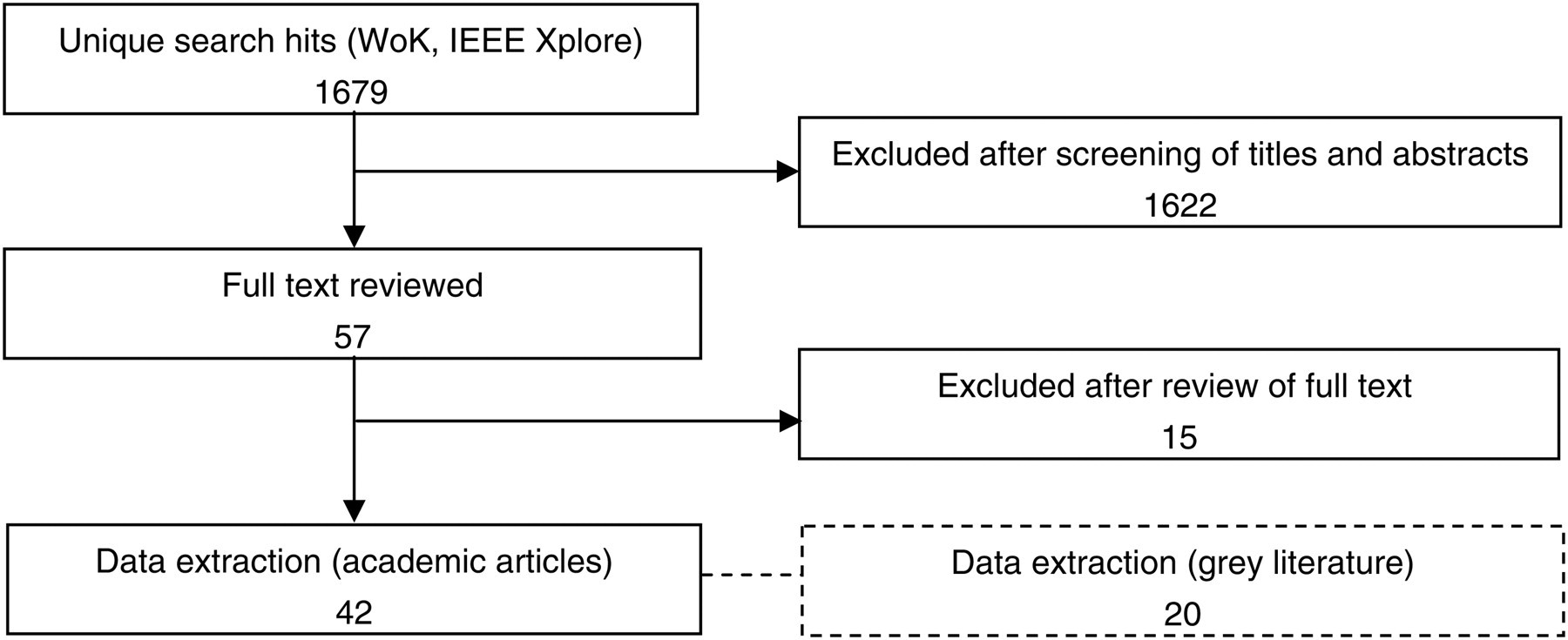
Literature search results
DITV systems
A total of 25 DITV systems were identified. Details of 19 of these systems had been first published in the previous three years. The country of origin and the applications of these systems are summarized in Table 2. The technical features of each system are summarized in Table 4. Definitions of terms used in these tables are provided in Tables 3 and 5, respectively.
Country of origin and applications of the DITV systems. Values in parentheses are the total number of applications/technical features which are currently under development
Com Commercial product
Dev Product in development
Cpt Concept (both ‘concept’ systems derive from academic, peer-reviewed papers which describe DITV architecture and describe potential health and/or social care applications)
# Not available in all areas or countries
* Not available on current TV system; some features available on the web-based version; not included in the total count
( ) Under development in commercial product
– Data unknown
Definitions of applications in Table 2
Technical features of the DITV systems. Values in parentheses are the total number of applications/technical features which are currently under development
# Not available in all areas or countries
* Not available on current TV system; some features available on the web-based version; not included in total count
( ) Under development
BB Broadband
DTT Digital terrestrial television
ISDN Integrated Services Digital Network
PSTN Public switched telephone network
RC Remote control
TS Touch screen
KB Keyboard
PDA Personal digital assistant
– Data unknown
Definitions of technical features in Table 4
Nearly all (n = 23) systems were located in the European Union and most had been developed in the UK (n = 8). Seven systems were commercially available, either through commercial organisations or public authorities, and 16 systems were in development. Two other systems were described as concepts only, where development has not yet begun but the proposed applications and technologies had been described in detail (Table 2).
Sixteen of the 25 DITV systems were identified from academic journals. The other nine were identified from the grey literature. A subsequent search of the Web of Knowledge using the brand names of the systems identified from the grey literature failed to retrieve any relevant academic articles.
An additional 13 systems were classified as ‘social television’ 7–17 but these were excluded from the study. Social television systems are designed to enhance television programme viewing, rather than providing or supporting care. For example, they provide a shared and enhanced experience of broadcast television programmes between remote viewers. This includes facilities such as what channel and programme other people are watching, text, voice and/or video communication to stimulate discussion about the TV programme. 10 A review of social television systems can be found in Harboe et al. 10
Applications
In the following results, frequencies and percentages stated include DITV systems in development or at the concept stage, as well as the commercial systems. Five of the 25 systems (20%) had a single identified application. Four or more applications were identified with seven of the systems (28%). The Viedome system had the greatest number of applications (6).
In general, health applications were more common than social care applications, with vital signs monitoring being the most common (68% of systems). Health-care information and education was provided in 56% of systems, and the facilitation of some form of direct consultation with health and care professionals (via voice, text and/or video) was identified in 44% of the systems.
Seven DITV systems (28%) facilitated social interaction in some form, mainly through video communication with other users. For example, the CaringTV system enables users to participate in welfare-promoting interactive video programmes, including exercise sessions, panel discussions with experts and free dialogue between users. Other examples of social interaction possible with DITV systems include experience sharing with other users and remote game-playing, as in the Viedome system.
While approximately half the systems provided access to ‘infotainment’ applications (such as news, home safety information, video-on-demand, photo albums), less than one-third provided information on local services and events.
Technical features
A wide range of technical features was identified (Table 4). Most of the DITV systems (18 out of 25) were designed for use with a broadband Internet connection. The most common technical feature, present in 88% of systems, was the transmission of information to and from the user. Many systems also incorporated medical peripheral devices for vital signs monitoring (n = 17), on-screen messaging (n = 12) and video communication (n = 9). The least common applications were games (n = 4), one-way communications (n = 4), environmental control (n = 4) and web browsing (n = 3). The Viedome system had the greatest number of technical features.
Only one system provided individually tailored services. The Stream system incorporates a ‘personalisation engine’ which develops a profile of users based on their needs and previous use of the system to provide relevant information. Most systems (n = 16) provide access to personal data and/or targeted information.
The input device for most systems (22 out of 25) was a remote control. Simplified remote controls which have a small number of buttons were used with the Betavista and VPTV400 systems. Other input devices included a portable touch screen console (Viedome, CaringTV) and wireless keyboards (Stream, SMART, T-Care).
Discussion
The present review identified several DITV systems that deliver health and social care, along with information services, to people in their own homes. A large number of applications and technical features were evident. Nearly three-quarters of the systems had three or fewer applications, with two-thirds of them mainly focused on health. However, the majority of the systems identified were still under development and their scope may be expanded in the future. This suggests that initially they have been designed to provide particular health-related DITV services (e.g. vital signs monitoring for a specific health condition) rather than cater for the wider and more general health and social needs of client groups. Four of the seven commercial systems provided both health and social care-related applications.
Applications
In general, health-care aspects were better developed than social care ones, and there was an emphasis on vital signs monitoring. In general, systems tended to have a few inter-related applications. Several DITV systems not only collected vital (or physiological) measurements from patients but also provided feedback and allowed varying levels of interaction with health-care professionals. Where vital signs monitoring was present, 82% of systems also provided either health-care education/information or consultation with a health or care professional, or both.
The ability to integrate multiple interactive multimedia applications on DITV has the potential to enhance the remote care received by the user. These types of health applications could be used to help self care, which is the care taken by individuals themselves of their own health and well being. 62 Enabling self care and helping people to understand their own health-care needs are becoming increasingly important as the demands on health-care services escalate. Many countries now promote self care through health-care policy 63 and DITV may be a useful method of supporting this.
The social care applications were less common and were typically designed to facilitate social interaction, mainly by videoconferencing. DITV may be used to help maintain a person's contact with family or friends or provide access to peer-support networks. Another possible area for development is greater access to information on local services and events. These types of Internet-based applications may facilitate and promote a sense of belonging and civic engagement, allowing the individual to play a fuller part in society. 64
Technical features
The number of technical features available in the DITV systems depended on their applications. For example, health-oriented DITV systems tended to have technologies such as medical peripherals (the other systems with a vital signs monitoring application required the user to manually input data such as weight and blood pressure). All nine systems with video communication were used for health-care consultations, as well as contact with family in some instances.
Multi-use systems with several applications incorporated more technology, with just under half of the systems identified in the review having more than three technical features. Systems incorporating more technology may be more expensive and may also add to the demand placed on the user to learn how to use the different functions.
Most systems incorporated two-way communications with the user. The most common technical features incorporated the remote communication of information (e.g. on-screen messages, email, videoconferencing). Where systems contained fewer technical features (3 or less), there was no apparent trend in the type of features included, except for the widespread use of technology requiring two-way communications.
The input control for most DITV systems was a standard remote control unit. However, many older people have difficulty in using these devices. Some people find the buttons too small or too close together with unclear labels and lacking in sufficient tactile feedback to indicate that a selection has been made. 65 These problems can be greater for people with physical, sensory or cognitive impairments, 66 which may lead to technology abandonment. The user interfaces of some systems identified in the review were better designed for use by older people. For example, the VPTV had a simple five-button remote handset with a built-in microphone and speaker for video communication. Other input devices that could be used for DITV include infra-red point and click, gesture recognition (e.g. Wii remote) and interactive voice response. Careful attention should be given to users with sight impairment, with the provision of audio and/or haptic feedback as part of the input control. Recent research has shown the potential of this concept for blind people using the Wii console. 67
The input control is only one part of the interaction of the user with a complete DITV system. Other aspects of the interaction are the type and size of display relative to viewing distance; content layout and navigation; data input method; text size and contrast; terminology; sound; and aesthetics. There was insufficient evidence from the articles in the review to extract data about these other factors. Carmichael 65 and, more recently, Collazos et al. 68 have produced design guidelines for DITV. Also, Rice and Alm 69 have investigated user-centred methods in the conceptual design of new DTV applications. More research is required, particularly in relation to older users for whom many of the systems are intended.
Personalisation
The systems identified in the study offered different levels of personalisation. Most provided either targeted information to users based on their demographic or health condition or enabled access to the individual's personal information, such as vital signs or feedback from clinicians. Personalisation has been defined as ‘the way in which services are tailored to the needs and preferences of citizens’ 61 and it is becoming more significant for the delivery of public services, particularly in the UK. Like the Stream system, other DITV systems could incorporate personalised information on local services and events based on the user's needs and preferences via some form of user profiling. This will increase the likelihood that the content is relevant to the individual, encourage long-term use and may reduce abandonment.
The extent that DITV systems ought to be personalised to the needs of an individual user is not yet clear. The type of health information provided by DITV systems ranged from publicly available information (e.g. access to NHS Choices 70 in the Stream system), to tailored content relating to the individual patient's health condition (e.g. access to topics relating to heart failure in the IGEA-SAT system). It could be argued that general health information, such as advice about different health conditions and health issues provided by NHS Choices, would be more suitable for a system aimed at a wider user group. In contrast, targeted and personalised information based on an individual's health records and vital signs measurements, for instance, may be more appropriate for the self management of a patient's specific health condition.
Market maturity and associated barriers to deployment
The present review identified 25 DITV systems, but only 28% of them were available commercially. Thus the field is still in its infancy. Market maturity is likely to be enhanced by the development of appropriate applications and technologies. Widespread deployment will also be assisted by the EU's i2010 policy framework 71 promoting health and social care delivery through technology, the almost ubiquitous ownership of TVs, the impending European-wide switchover from analogue to digital television, and the rapid technical advances being made in interactive television.
However, the present review also identified certain barriers that need to be overcome to enable DITV to reach its potential to deliver health and social care effectively on a large scale. First, the wider use of DITV systems may be inhibited by the lack of scientific evidence regarding their clinical and cost-effectiveness. Half of the DITV systems (12 out of 25) did not report any user evaluation results and determining the scale of evaluations from the other articles was difficult. In addition, the level of user involvement in the design process was often unclear and we could not identify any articles which published the user requirements for a particular system. Evaluation outcomes were typically focused on system usage and user satisfaction. Health outcomes were evaluated for only three systems (Motiva, NHS Direct, IGEA-SAT).
This lack of information may have a number of causes: the funding for technology development may not have included evaluation; products may have been evaluated but the results not published due to commercial sensitivities; the exclusion of non-English articles in the search strategy; the source of information; and the latency of publication as a result of the relative immaturity of the technology. For example, one-third of the DITV systems were identified from the grey literature, such as commercial websites, rather than the academic literature. In addition, the majority of systems have emerged in the last three years and few have reached full development, so there may not have been sufficient time for a whole system evaluation. Some systems (e.g. NHS Direct Digital, Stream) have also been cancelled or scaled down in their scope. The fate of these large scale projects may indicate the difficulties of market penetration. This suggests a need for further research on user requirements and the health and social effects of DITV systems.
Second, many of the DITV systems were designed for broadband connections. Systems with multiple applications requiring two-way communication, such as videoconferencing, need high bandwidth for reliable data transfer. The infrastructure and costs associated with such data transmission speeds could, therefore, be a limiting factor in certain areas and countries. Several European countries, such as the Netherlands, have a well-established high-bandwidth communication infrastructure, whereas it is more fragmented in the UK. It is therefore interesting to note that the greatest number of developments identified were from the UK, with most systems being designed for use with broadband.
Third, DITV will only be successful in the long term if users are confident in operating the equipment. The high number of systems which use a standard remote control unit with many buttons may be cause for concern. Both the input control and user interface for the DITV systems should be suitable for the intended users, particularly if targeted at older people.
Conclusion
The present review identified 25 DITV systems which incorporate a wide range of applications and technical features. There was a trend towards health-oriented applications and the use of DITV for social care was less developed. The changing population demographics, the familiarity of television and the recent proliferation of interactive television technologies suggest that DITV has potential for delivering health and social care to people in their own homes. However, the requirement for a high-bandwidth communications infrastructure, the usability of the systems, their level of personalisation and the lack of evidence regarding clinical and cost-effectiveness will all need to be addressed if this approach is to flourish.
Footnotes
Acknowledgements
We thank the Technology Strategy Board for funding the study and the project partners for their contribution: Tunstall Group Plc, DigiTv, Fold Housing Group and Housing21 Ltd.