
Abstract
The evidence base for lifestyle monitoring is relatively weak, even though there are significant numbers of commercial installations around the world. We conducted a literature review to summarize the current position with regard to lifestyle monitoring based on sensors in the home. In total, 74 papers met the inclusion criteria. Only four papers reported trials involving 20 or more subjects, with a further 21 papers reporting trials involving one or more subjects. Most papers (n = 49) were concerned with technology development. Motion detection was the most common of the technologies employed, followed by door and electrical appliance usage. The predominant monitoring strategy was that of detecting changes in activity. However, little attention has been given to determining when or how changes in the profile of activity should be used to raise a call for assistance from a health or care professional. Lifestyle monitoring remains a relatively immature research area in which there is little detailed understanding of how to provide comprehensive and effective systems.
Introduction
In lifestyle monitoring, sensors are installed in the home to monitor behaviour in order to gain an understanding of ‘normal’ activity so that any unusual changes over time can be recognised and responded to. For example, a sudden change in mobility around the home may indicate that the subject has fallen, while a gradual decline in the time spent in the kitchen may suggest illness or malnutrition. In addition, some applications of lifestyle monitoring have been used as assessment tools, i.e. installed for a short period of time to provide data to assist the care assessment process. 1
The underlying assumptions of lifestyle monitoring, namely that it is possible to determine an individual's health or care status by the remote monitoring of behavioural characteristics, were the focus of the study undertaken by Celler et al. 2 in 1995. They concluded that an individual's health status could be determined by monitoring relatively simple variables relating to the interaction between the individual and their local environment. They reported that some 50% of people had undiagnosed medical problems that could be detected by home monitoring. Subsequently the Anchor Trust and British Telecom developed a system to detect changes in a user's lifestyle. 3,4 The final conclusions of these studies were that the system was generally acceptable, that it enhanced feelings of safety and security, that it increased care choices, and that it supported and enhanced the carer's role.
Despite the growing interest in all aspects of telecare, the evidence base remains relatively weak, especially for lifestyle monitoring, even though there are significant numbers of commercial installations around the world. We therefore conducted a literature review to summarize the current position with regard to lifestyle monitoring based on sensors in the home.
Methods
The review considered articles dealing with lifestyle monitoring available on the electronic databases OvidSP (and including Medline, CINAHL, PsychInfo and British Nursing Index) and INSPEC using the search structures and terms described in Table 1. All articles, including conference proceedings, published in the English language between January 1990 (5 years before the Celler et al. study which was one of the first of its type) and December 2009 were included.
Search terms and search structure
The focus of the review was on home-based lifestyle monitoring systems using the following exclusion criteria:
Articles evaluating user views only; Articles about Smart homes centred around the control of the environment only; Behavioural monitoring using mobile devices such as GPS or mobile phones; General reviews of assistive technology; Horizon scanning or ‘blue sky thinking’ articles; Non journal or conference proceedings; Articles not written in English; Stand alone technologies related to vital signs monitoring with no links to the identification of behavioural change; Technological concepts with no evidence of development; Technology centred around the use of video cameras only; Technology centred around the use of wearable sensors only; Theses.
No exclusion criteria were set on the quality of papers.
Two reviewers independently applied these criteria to the papers identified. In the case of any disagreement, a third, independent reviewer made the final decision on which papers were included. The exclusion criteria were then applied again on the full papers and, where appropriate, data extracted. A number of papers described distributed sensors for behavioural monitoring in association with vital signs monitoring, video cameras and body-worn sensors and these were retained in the review.
Results
The database search identified a total of 1994 articles. Of these, 1420 were associated with OvidSP and its subsidiary databases and 574 with INSPEC. On review, it was established that there were a total of 159 duplicates between the databases, giving a total of 1835 unique articles.
The initial screening of these 1835 articles resulted in a total of 133 potentially relevant articles, with the two reviewers agreeing on 79 of them (59%). The remaining 54 articles identified by only one of the reviewers were then independently evaluated by a third reviewer and it was decided that 28 of these articles should be included. This resulted in a total of 107 articles for detailed review of the full texts. Of these, a further 15 were rejected on the basis of the full text while 18 proved to be unobtainable even when the authors were contacted by mail and email, leaving a total of 74 articles to be subjected to full review. The distribution of these 74 articles by year is shown in Figure 1.
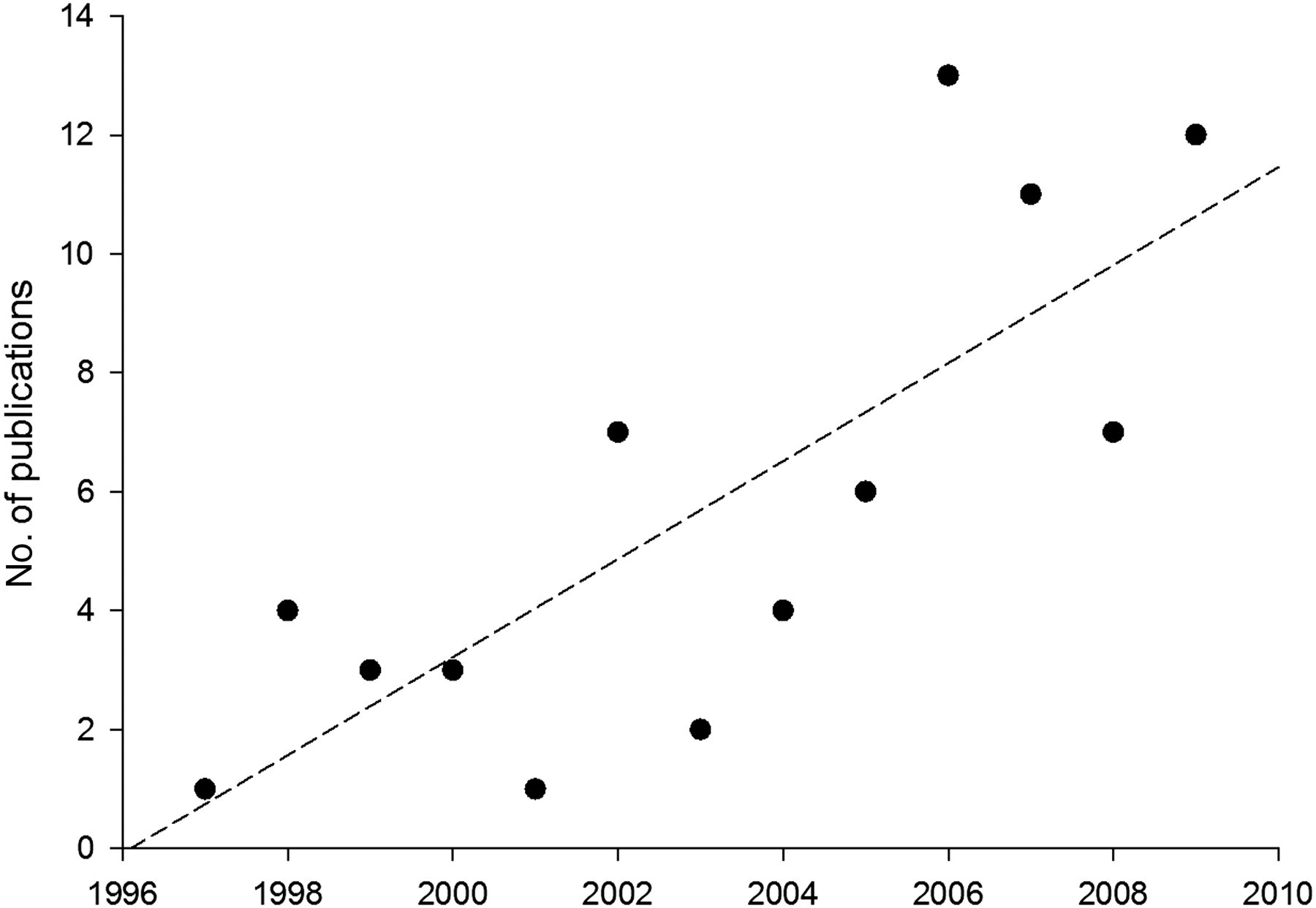
Number of publications identified for review and their year of publication. The broken line is the least-squares regression
Of the 74 full articles reviewed, only four 5–8 were concerned with trials involving more than 20 subjects (Table 2), whilst a further 21 papers reported trials with fewer than 20 subjects. The distribution of reported trials is shown in Figure 2. The remaining 49 papers described only technology development without reporting on any formal user trials.
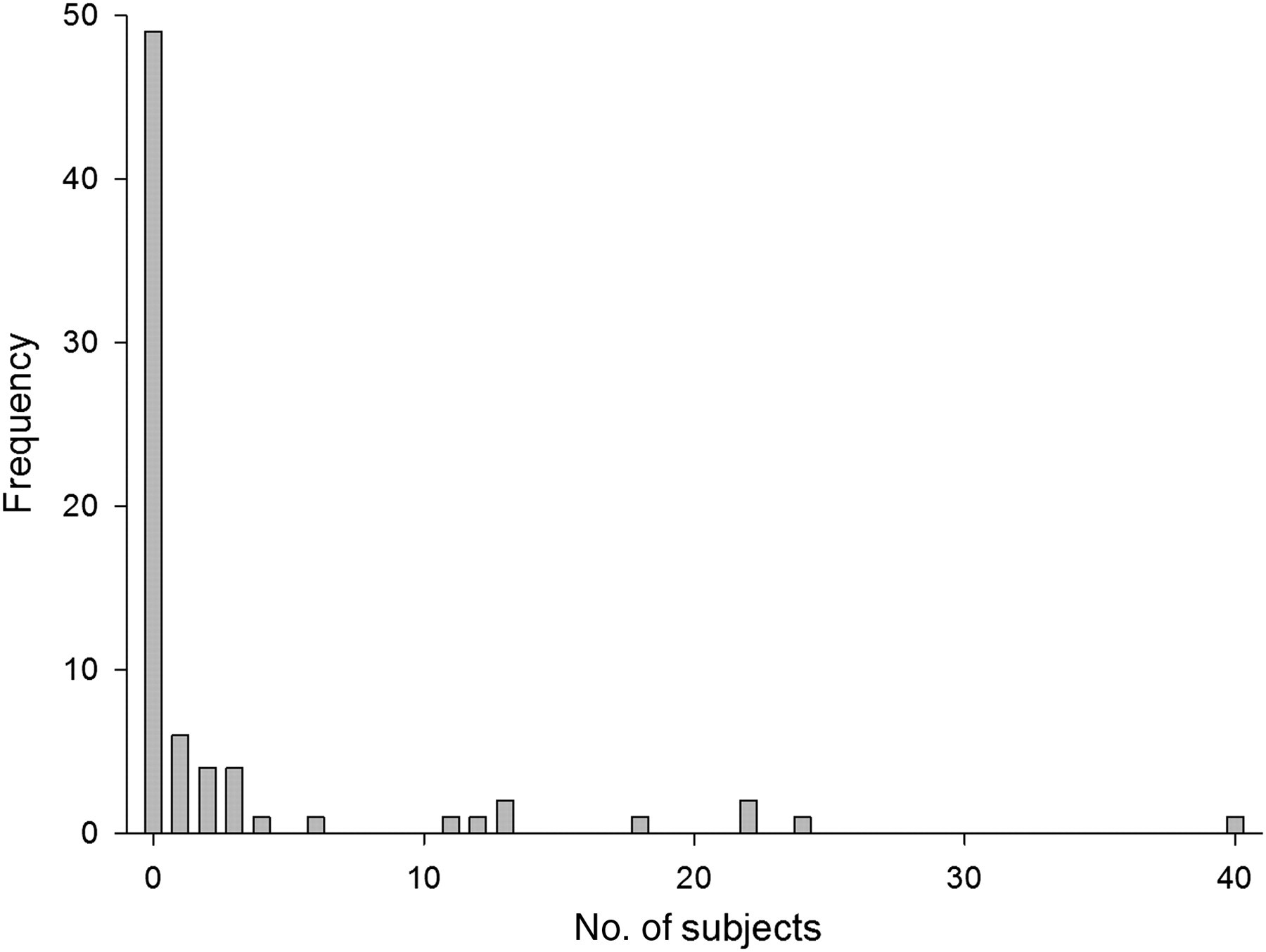
Numbers of subjects
Articles reporting trials involving more than 20 participants and sorted according to sample size
Motion detection was the most common of the technologies employed, see Table 3. For studies which included other monitoring approaches in addition to behavioural monitoring, the sensor types are summarized in Table 4. The number of studies employing associated monitoring strategies is shown in Table 5, while Table 6 shows additional information associated with the deployment of the monitoring approaches of Table 4.
Number of studies employing specific sensor types
Other forms of monitoring used in association with a behavioural monitoring approach as the primary element
Variables evaluated during behavioural monitoring
*Distinction is made here between monitoring systems which use a formal means such as the official Barthel index to record ADL and monitoring systems which express general levels of activity by other means, for example the proportion of active time in a day or transitions between rooms
Variables evaluated in association with behavioural monitoring
The information analysis and artificial intelligence methods employed are summarized in Table 7. There is increasing investigation into such techniques. However, on the basis of the papers reviewed, the techniques are not yet robust enough for operational use and performance data is still lacking.
Information analysis and artificial intelligence methods
Discussion
The majority of articles provided only an overview of the methods that were applied along with, where appropriate, brief details of the evaluations being undertaken. It is therefore difficult to obtain a complete understanding of what systems and methods have been deployed and in what context. There is a need for all involved in the reporting of research and development findings in this area to provide more information about what they are seeking to achieve and the associated methodologies.
Figure 1 suggests that there has been a steady increase in publications on lifestyle monitoring in the home since 1997. The first paper included in the review was from 1997, confirming that Celler et al.'s study in 1995 was one of the earliest of this type. Only 25 papers reported trials involving one or more individuals, while 49 papers reported on technical development in the absence of trials. This provides only weak formal evidence to support the use of lifestyle monitoring, despite numerous commercial installations around the world. Where evaluation with users has taken place, studies have not yet addressed the clinical and cost effectiveness of the intervention when compared to conventional care delivery. Large scale and longitudinal studies would be helpful, such as that being undertaken by Kaye who has recruited 200 older people, installed lifestyle monitoring systems in their homes, and is gathering data over a 30 month period. 9
Many commercial lifestyle monitoring products are now offered for short-term health and care assessments, 10,11 where equipment is installed for a period of a few weeks and then removed. Since there may be more immediate commercial potential in short-term care assessment, researchers may find it valuable, in order to maximise the impact of their work, to focus their efforts on short-term assessments as well as long-term monitoring.
A wide range of sensor technologies have been used in association with an equally wide range of monitoring strategies (Tables 3–7). For most approaches, the most common sensor technology was the PIR for motion detection, followed by door contacts and electrical supply monitoring. These somewhat crude sensors for data capture may be appropriate for monitoring gross changes in room occupancy and so forth, but for finer analysis the resolution is probably too low. Thus when attempting to link user activity data to formal health and care assessment, researchers may need to acquire data of finer granularity to ensure that accurate assessments can be made.
It is clear from Table 5 that the predominant monitoring strategy is that of detecting changes in activity. Very little attention has been given to determining when or how changes in the profile of activity should be used to signal an important change in health or care status that merits the raising of an alert. Thus, the emphasis has been on detecting changes in the profile of activity, but not on linking this to procedures to determine health and care needs, or of triggering a re-assessment of such needs. Indeed, in many instances there appeared to be a deliberate decision that the focus should be on highlighting changes to activity profiles, and that professionals should then analyse the data and determine when and how to intervene. While this reduces the technical complexity, it may represent a barrier to uptake. Specifically, it is unlikely to be cost effective if clinicians have to spend substantial time in monitoring behaviour that subsequently does not necessitate a health or social care intervention.
Many of the articles reviewed employed information analysis, artificial intelligence and machine intelligence techniques to identify changes in patterns of behaviour. However, these were generally employed in the context of an established profile of behaviour with limited attention given to the introduction of other, long-term factors which may influence behaviour, such as seasonal variations in behaviour. It should also be noted that much of what has been reported was associated with the evaluation of the method rather than its use in an operational environment.
The present review therefore raises a number of questions:
What is the primary purpose and role of lifestyle monitoring (assessment, long-term monitoring or both)? Can levels of activity be effectively monitored using current sensors? Is the link between health status and activity sufficiently well understood? What features of a particular person's life and activity should be monitored? Do the data analysis techniques being utilised result in clinically important information? What is the correct service response to monitoring, and what are the organizational and operational issues associated with this?
In summary, the original aim of the literature review was to establish the current position with regard to lifestyle monitoring research and hence to inform requirements for future development of such systems. Whilst the review provided a better understanding of activity worldwide with respect to lifestyle monitoring, the lack of detail about methods and outcomes restricts the conclusions that can be drawn. Although there are some promising case study results, the review suggests that lifestyle monitoring remains a relatively immature research area in which there is little detailed understanding of how to provide comprehensive and effective systems.
Footnotes
Acknowledgements
The study was independent research commissioned by the National Institute for Health Research. The views expressed in this publication are those of the authors.