
Abstract
We created a website for patients and families that allowed them to review clinic test results, review educational materials related to these results and post questions to their diabetes educator. Fingerstick haemoglobin A1c (HbA1c) testing and periodic use of a continuous glucose monitoring system (CGMS) were offered to all patients. The HbA1c and CGMS results were posted to the website after each clinic visit. A total of 52 patients with type 1 diabetes were enrolled in the study. There were 16 patients with HbA1c values within ADA guidelines and 16 with HbA1c values above guidelines; 20 patients were excluded for various reasons. Users of the website were defined as families who logged in four or more times over the six-month study period. For patients whose HbA1c started above ADA guidelines, the mean HbA1c for website users decreased from 10.5% (SD 2.2) at baseline to 9.1% (SD 1.2) after six months. In the non-users, the mean HbA1c increased from 9.5% (SD 1.5) at baseline to 10.4% (SD 2.5). However, these changes were not significant. A between groups comparison (users versus non-users) showed a significant improvement in HbA1c for website users (P = 0.03). This change in HbA1c was clinically relevant. Further studies with more patients are needed to see if these improvements can be sustained over a longer period.
Introduction
Type 1 diabetes mellitus is a chronic disease that requires lifelong medical management. Education is given to patients and their families at the time of diagnosis, but this is often only basic management (sometimes referred to as ‘survival skills’) and may not be fully understood. 1 Patients and their families need continuing education as they encounter specific problems in managing their diabetes. It has been suggested that difficulties in accessing appropriately trained medical staff can be a significant barrier to improving patient and family understanding of diabetes management. 2 In addition, studies suggest that educational interventions need to continue. 3–7
We hypothesized that patients would prefer to use an Internet-based system for continuing education. Therefore we created a website, the Pediatric Diabetes Education Portal (PDEP), designed to augment the teaching delivered at clinic visits and improve access to care.
Pediatric diabetes education website
Patients and their families were encouraged to use the website to review their test results, review educational materials and post questions between clinic visits. Patients were shown how to log in to the website at clinic visits but received no additional training on using the site. An example of a family and provider interacting on the website is shown in Figure 1. Parents were given access to their child's case file on the website, and depending on the age of the child and parent preference, the patient was also granted access. In some cases both parents were given separate access to their child's case so both could be notified by email separately when new comments were added.
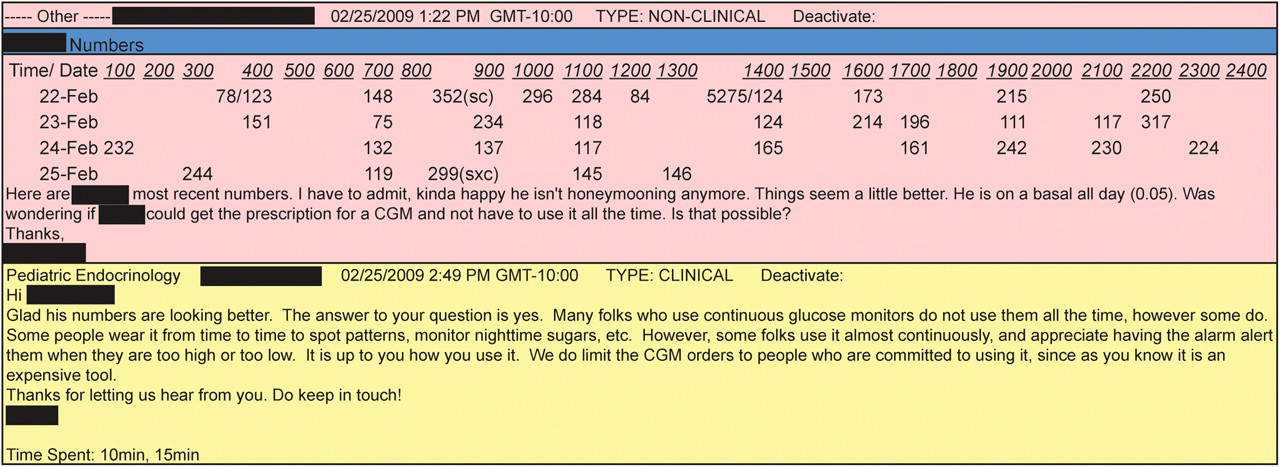
An example of the provider screen showing comments from a patient, including a blood glucose log and comments from the provider
Results of point-of-care HbA1c testing and summary graphs of the CGMS readings were printed for patients at clinic visits and were then posted to the website so they could later be viewed from home. When a new comment or document was added to the information on the website, all case participants were notified by email so that they could log in to view it. An example of the test results posted on the website are shown in Figure 2.

Example of HbA1c and CGMS data posted to the website after a clinic visit. The differently coloured lines on the CGMS graph represent different days. The CGMS recorder measured glucose readings every 5 min and used the patient's glucometer readings to calibrate these points
Postings from the diabetes care team invited patients to review information related to their test results and to review educational materials. Providers were able to switch between cases on the website, use a built-in billing system, and forward the case to other physicians for review if necessary. Patients and their families saw a simplified view of the website without these additional features.
Hypothesis
Numerous studies have shown that increased frequency of HbA1c and lipid testing do not necessarily lead to significant improvements in HbA1c, lipid profiles 8 or quality of life 9 for patients with diabetes. Furthermore, a recent meta-analysis of home telehealth did not support a definitive link between telehealth and diabetes outcomes. 10 The PDEP website was accessible from home and allowed: (1) review of educational materials related to patient test results, (2) posting of questions about blood glucose logs and (3) communications between the patient and family and their diabetes care provider. We hypothesized that use of the website would improve outcomes for children with type 1 diabetes.
Methods
All children with type 1 diabetes and their families seen at our clinic over one year were offered access to the PDEP. Patients and their families were enrolled and confirmed to have Internet access at home and/or work from which to access the website. The PDEP website allowed families to log in from home to view educational materials related to their test results, post questions and read comments from their physician and diabetes educator. HbA1c was measured at enrolment and then every three months. Use of a continuous glucose monitoring system (CGMS) was offered at least once to every patient in the study (Medtronic iPro, Medtronic, Minneapolis, USA). The sensor and recorder were worn for 3–5 days and the data were downloaded at clinic visits, when summary graphs were printed for the patient and family.
After six months of use of the PDEP, questionnaires were given to patients and families to assess their satisfaction with the website, point-of-care fingerstick HbA1c testing and CGMS use. The responses were made on a 5-point Likert scale. All questionnaires were completed by all family members together and either returned by mail or at subsequent clinic visits.
Patients and/or parents were classified as users or non-users of the website. Users were defined as patients and/or parents who (1) logged in to the website four or more times or (2) logged in two or more times if they also posted comments.
To examine improvement in HbA1c, patients were divided into those whose baseline value was above the ADA age-recommended guideline at enrolment and those whose value was already within the guideline. The change in HbA1c from baseline was compared between the user and non-user groups after six months with an unpaired t-test.
To determine if use of the website encouraged patients to use other means of accessing care, the number of clinic visits and telephone calls amongst users and non-users related to diabetes management was compared for six months before and six months after enrolment. This analysis excluded telephone calls or clinic visits for prescription refills or for administrative reasons (e.g. school forms).
The study protocol was approved by the appropriate ethics committee. Written informed consent was obtained from all study participants.
Results
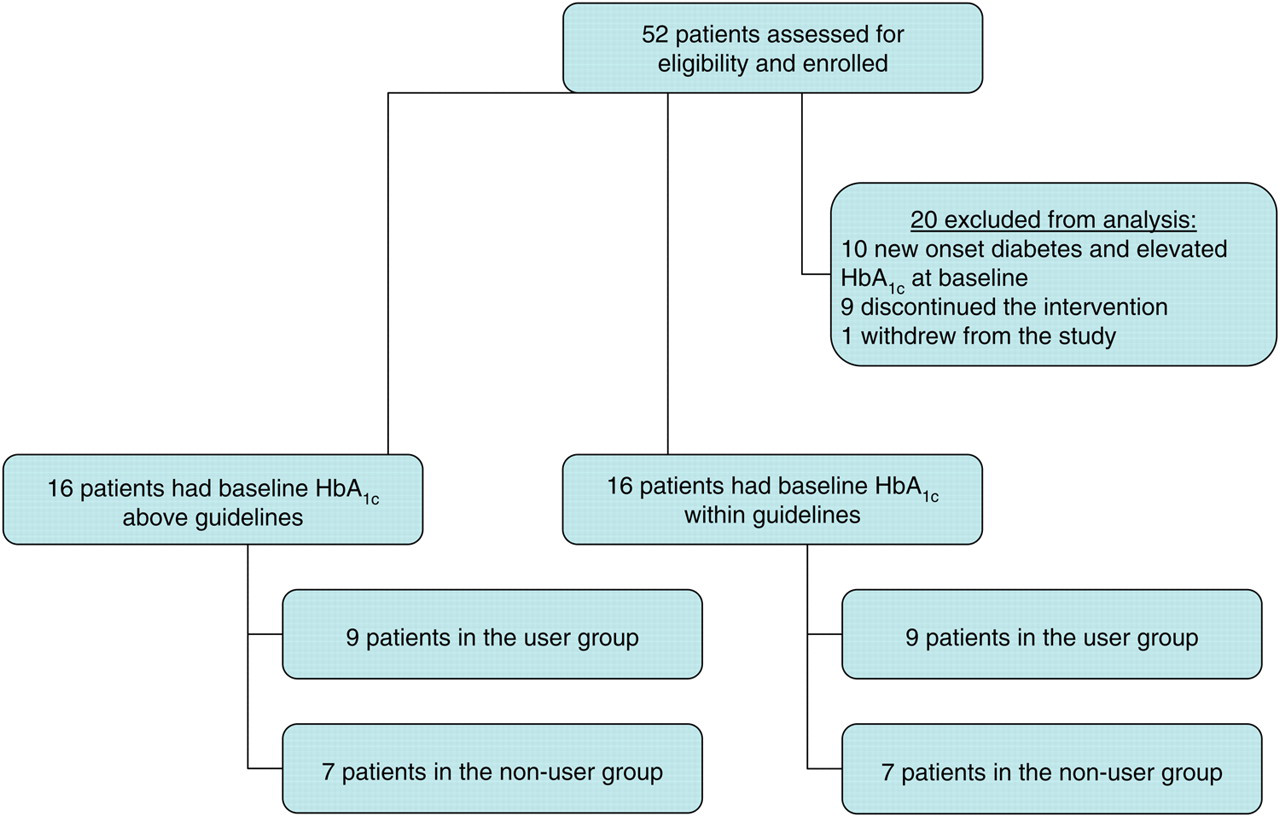
A total of 52 patients were enrolled over one year. Twenty patients were excluded for various reasons (see Figure 3), 16 patients had HbA1c values within ADA guidelines and 16 had HbA1c values above guidelines. The mean age of the patients who were users of the website was 11.5 years (SD 4.0), and the mean age of the non-users was 10.9 years (SD 4.2). Twenty-five of the 52 patients were female.
Study participants
Of the 16 patients whose baseline HbA1c was above the guideline value, nine met the definition of being a user of the website. Of these, seven had an HbA1c measured after six months. The mean HbA1c decreased from a baseline of 10.5% (SD 2.2) to 9.1% (SD 1.2). This change from baseline was not significant (P = 0.06).
There were seven non-users, of whom only four had a follow-up HbA1c measured at six months. The mean HbA1c increased from baseline 9.5% (SD 1.5) to 10.4% (SD 2.5). This change was not significant (P = 0.13).
A between groups comparison (users versus non-users) showed a significant improvement in change in HbA1c for the user group (P = 0.03). These results are summarized in Table 1.
Mean values of HbA1c for patients whose value was above ADA age-recommended guidelines at baseline. Comparison between groups, P = 0.03
There was no correlation between CGMS use and the change in HbA1c for the five patients who tried it in the user group. Only two of the non-users tried CGMS, and neither had a six-month follow-up HbA1c for comparison.
Both users and non-users showed an increase in provider contacts by clinic appointments and telephone over the six-month period (2.3–7.0 encounters per patient). However, there was no significant difference in the number of contacts between the user and non-user groups (P = 0.42).
Of the 16 patients whose baseline HbA1c was within guidelines at baseline, all remained so for the duration of the study. Both users and non-users showed a slight increase in mean HbA1c, but there was no difference between the groups (P = 0.45). These results are summarized in Table 2.
Mean values of HbA1c for patients whose value was within ADA age-recommended guidelines at baseline. Comparison between groups, P = 0.45
Questionnaire
Seventeen of the 52 patients/families returned satisfaction questionnaires (33% response rate). Website users reported greater satisfaction with the interventions in the study and felt that use of the system led to an improvement in their diabetes care. While some patients and families were very satisfied with the website, many identified a need to make logging in easier and to make the site simpler to use. The results are summarized in Table 3.
Questionnaire results. The quality of the study interventions was scored using a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree). Values shown are the median scores
Discussion
The present study suggests ways of improving care for paediatric patients with type 1 diabetes. Previous studies have found that frequent self monitoring of blood glucose (SMBG) is not always helpful and, in isolation, can lead to depressed mood. 11 We hypothesized that when SMBG is linked to educational advice and changes in clinical management, as we did by posting test results and educational material on the PDEP website, patients and their families would more actively manage their diabetes.
It is our contention that patients with type 1 diabetes stand to benefit the most from telemedical intervention. Unlike patients with type 2 diabetes who are often initially managed with oral medications and who only require periodic adjustment of their treatment plan, all of our patients with type 1 diabetes required multiple daily doses of insulin and frequent dose changes. In addition, these patients must constantly adjust their insulin according to their diet plan. Therefore rapid telehealth review of questions to help patients change insulin doses is appealing. While previous studies in type 1 diabetes have shown significant improvement in patient contacts with their provider, they have not yet shown consistent evidence of improvement in metabolic control as measured by HbA1c and hypoglycaemic and hyperglycaemic episodes. 12 A meta-analysis of studies using Internet-based blood glucose logs for type 1 diabetes has confirmed these findings. 13
Participants in previous diabetes telemedicine intervention studies have reported the need for easier interaction between patients and clinicians, and dietary and nutritional educational material for different groups of patients. 14 This was also found in the Diabetes-STAR trial which failed to show improvements in self-care behaviour in patients with diabetes who used a website to review their records. Interviews with patients showed the need to: (1) address differences in types of users, (2) send out alerts when new information was available, and (3) provide more oversight of the use of dietary data. 15 The PDEP was designed to address all these concerns by automatically notifying patients and providers when new information was posted to the website and by providing links to educational material.
In our study both users and non-users increased contact with their diabetes care provider by telephone communication and clinic appointments, but only users of the website showed improvements in HbA1c. This suggests that it was website use, and not more frequent clinic follow-up, that led to improvement in HbA1c. We speculate that being able to log in and see clinical test results may have allowed website users to obtain more frequent feedback about managing their diabetes, ultimately leading to improved diabetes management.
We also found that CGMS use was not associated with a change in HbA1c, probably because of the small number of patients in the study. In addition, users of the website whose HbA1c started within the recommended range showed no change versus non-users, and on average these patients stayed within the guidelines. This was expected as they had little room for improvement to begin with.
Strengths and weaknesses
A strength of our study was the positive feedback from patients who used the website, which showed that HbA1c can improve with more active diabetes management. Participation on the website may lead to improved patient knowledge and better diabetes control.
Limitations of the study include the small sample size and short follow-up period. It would therefore be premature to conclude that use of websites like the PDEP would help all paediatric diabetic patients. In addition, comments from the questionnaires showed that the website was sometimes difficult for patients to use. The main reasons cited by non-users for not using the system were trouble logging in from home and difficulty with posting comments. Additional training may be necessary for new users of the site to overcome these difficulties.
One frequently requested function was automatic uploading of blood glucose logs, which has been successfully demonstrated in other trials. 12,16 Also, discussion amongst providers showed a preference for standardized formatting of the blood glucose logs, as patients posted their blood glucose readings in different formats that were not always amenable to rapid review.
In the present study, patients with an elevated baseline HbA1c who used the PDEP website showed significant improvement in HbA1c when compared to patients who did not use the site. The decrease in HbA1c which occurred was clinically relevant. Further studies with more patients are needed to see if these improvements can be sustained over a longer period.
Footnotes
Acknowledgements
We thank Dr C Becket Mahnke for his assistance in creating the PDEP website. We also thank Mr Ri Wen Li for assistance in linking laboratory results to the PDEP and Ms Eludrizza Tabisola-Nuesca, Dr Anita Pedersen and Dr David Crudo for providing care for patients on the website. The work was funded by the AMEDD Advanced Medical Technology Initiative through the Telemedicine and Advanced Technology Research Center. The views expressed here are those of the authors and do not reflect the official policy or position of the Department of the Army, Department of Defense, or the US Government.