
Abstract
A 56-year-old man was on the transplant list with end-stage liver disease secondary to hepatitis C when a donor liver became available at a location 545 km away. The procurement team, consisting of a senior and junior fellow, went on the retrieval, while the staff surgeon remained in the hospital with the recipient. At the time of organ procurement, a suspicious lesion was identified in the left lateral lobe. The transplant fellows took intraoperative pictures of the lesion with a smart phone and sent them to the staff surgeon for advice. A teleconsultation, facilitated by images sent from the smart phone, took place over the next 22 min. The decision was made to proceed with the transplant, as it was felt that the lesion could be resected from the liver allograft. Had the fellows not been able to interact with the staff surgeon in real-time during the surgery, there is a high likelihood that the organ would have been rejected by the staff surgeon due to the unexpected finding. The patient's postoperative course was relatively uneventful with no evidence of infection. The patient was discharged from hospital and continues to do well. We expect that the role of smart phones in remote consultation will continue to expand in future.
Introduction
The use of smart phones such as the RIM BlackBerry, the Apple iPhone or the Google Android is becoming increasingly common in medicine. 1,2 Smart phones have a wide range of applications from specific programs such as pharmacopoeias and medical calculators, to real-time telesurgery consultations. 3 Smart phones have also been used to allow specialists to conduct remote consultations for stroke patients. 1,3
In many Canadian transplantation programmes, trained fellows are sent to perform the organ procurement while the staff surgeon remains at the recipient site. At the time of procurement, decisions must be made about the quality of the donor liver, even though there will have been an extensive work-up by the organ procurement organization. If the allograft is found to be of poor quality then the team will communicate this to the staff surgeon who must decide whether or not to reject the organ without observing the organ characteristics personally. The present report concerns a case in which smart phones were used in real-time to gain a staff opinion in the evaluation of a donor liver during organ procurement at a remote site.
Case report
A 56-year-old man was on the transplant list with end-stage liver disease secondary to hepatitis C. He had been admitted to hospital with the decompensated features of liver failure and continued to deteriorate following admission with hepatorenal syndrome and severe hepatic encephalopathy and a Model of End Stage Liver Disease (MELD) score of 34. 4 A donor liver then became available at a location 545 km away. The donor was a middle-aged male who had sustained brain death from head trauma with no previous medical or surgical history. The patient was afebrile, had a normal white blood cell count and was on low dose pressors. The procurement team, consisting of a senior and junior fellow went on the retrieval, while the staff surgeon remained in the hospital with the recipient.
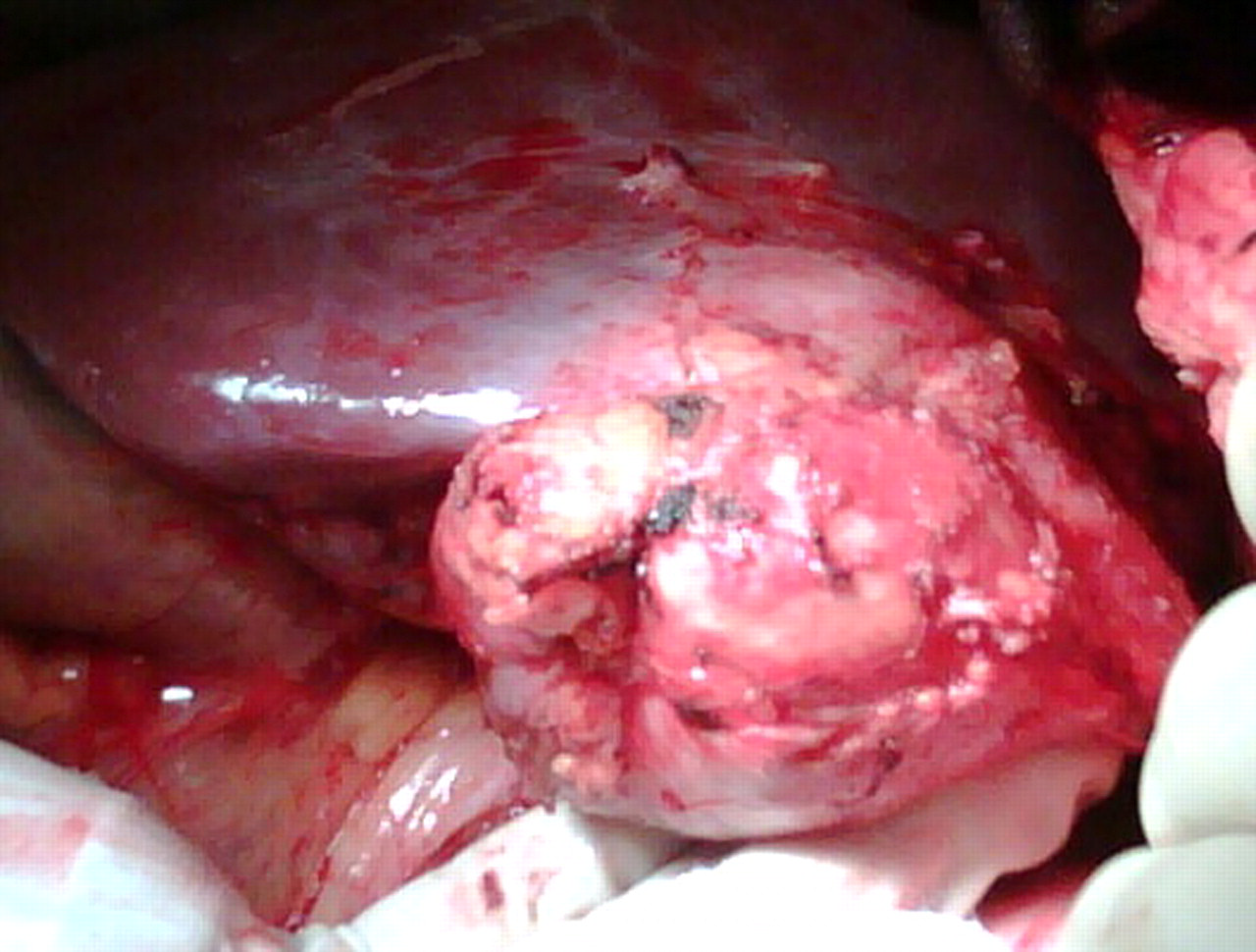
At the time of procurement, a lesion was identified in the left lateral lobe. The following discussion ensued over a 22 min period, via smart phones (BlackBerry Bold with 3.2 megapixel camera):
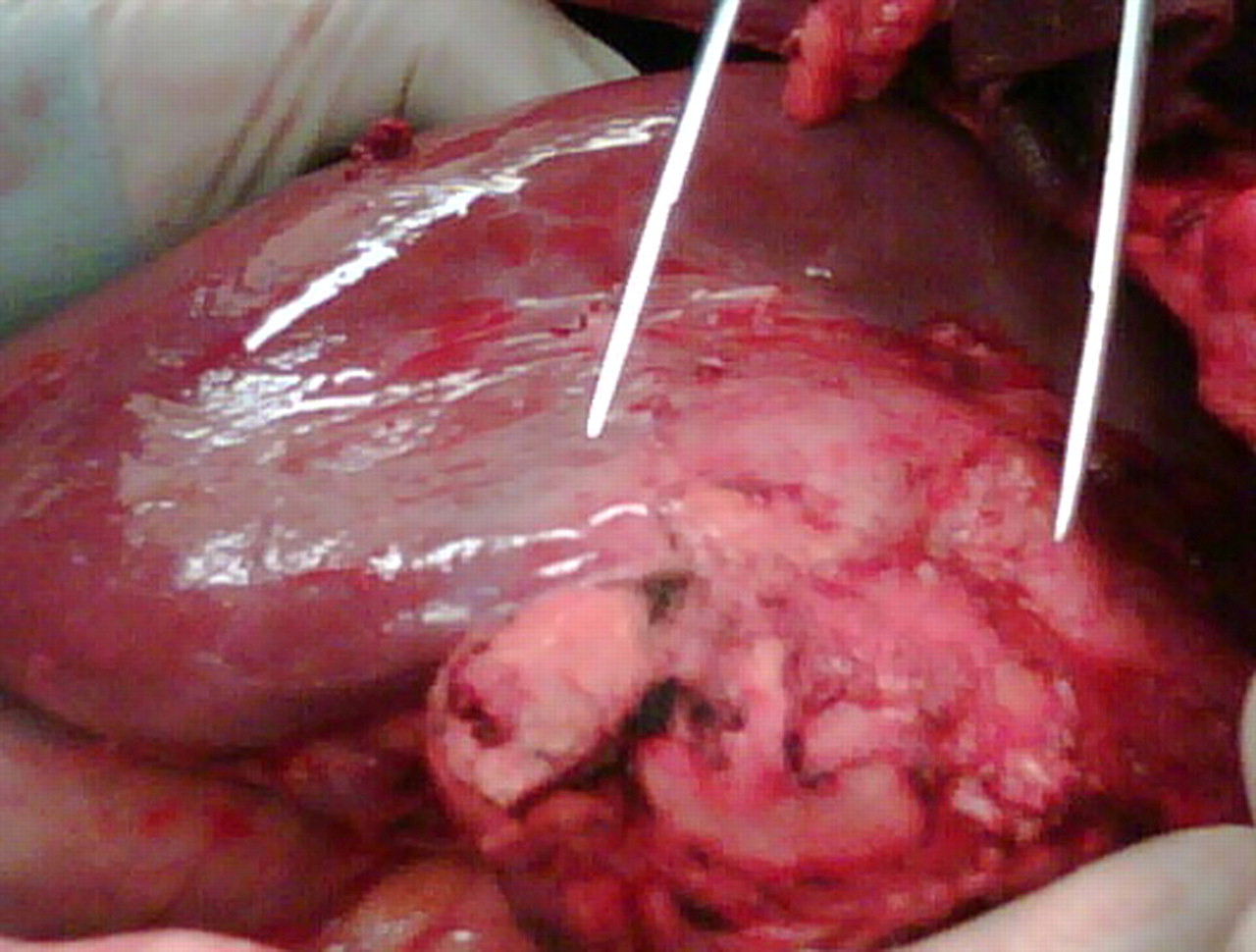
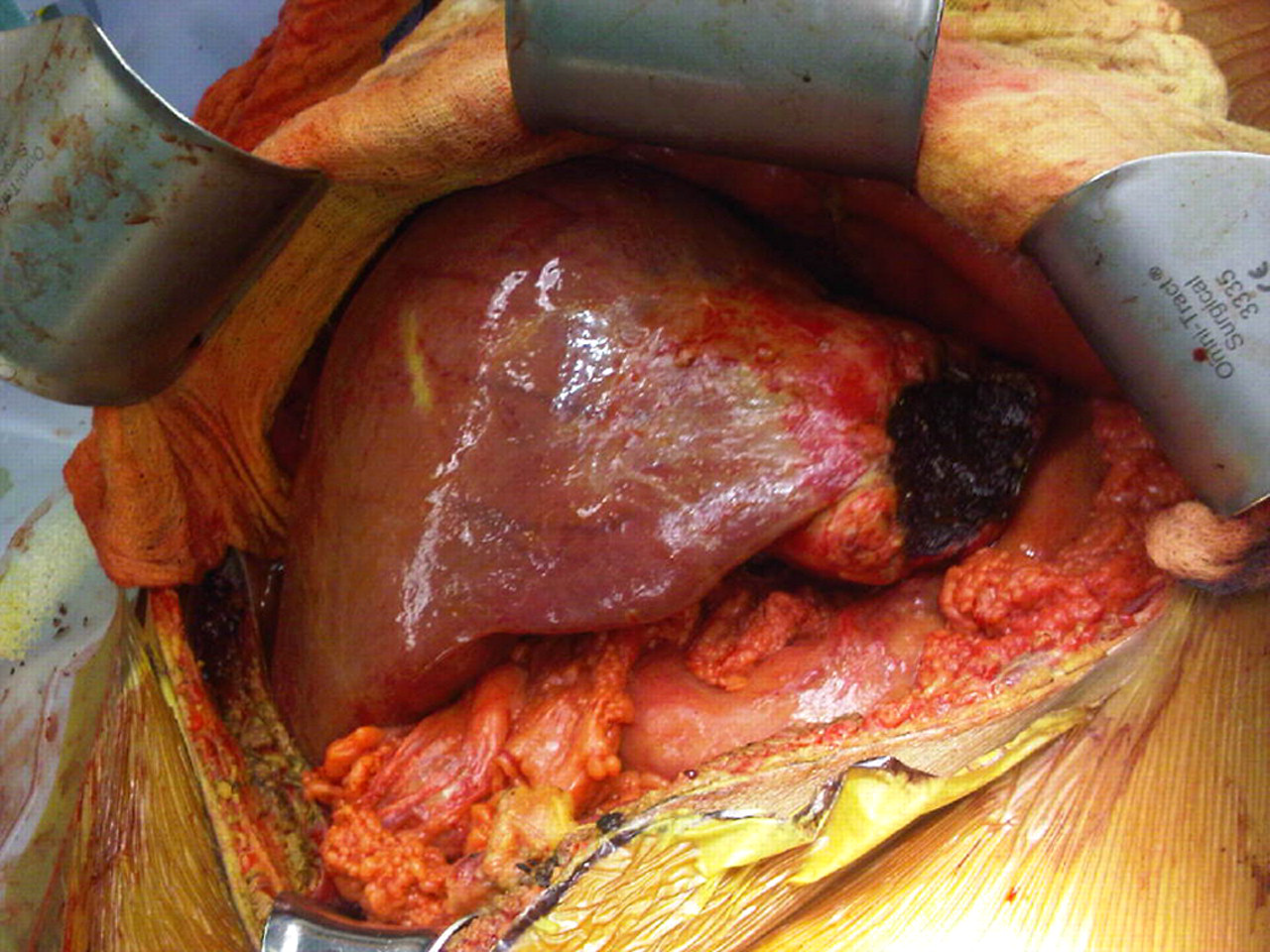
The transplant fellows took intraoperative pictures of the lesion with a smart phone and sent them to the staff surgeon for advice (Figure 1). The staff surgeon responded by asking for measurements of the lesion as well as a more detailed description of the lesion's texture, consistency and any other additional abdominal findings. The fellows measured the lesion size as 6 cm and sent a response to the staff surgeon (Figure 2). The fellows suggested malignancy as a possible aetiology. Based on the photographs and the description given by the fellows, the staff surgeon felt that the likelihood of the lesion being a cancer was low and asked the fellows to incise the lesion. The fellows incised the lesion and sent a photograph back to the staff surgeon. They explained that the lesion contained a thick purulent material. The fellows sent a picture to the staff surgeon identifying calcification of the capsule of the lesion, which suggested a chronic process (Figure 3). The material from the lesion was sent for Gram staining and for acid-fast bacilli staining, both of which returned as negative at the donor site. A frozen section was also sent and was negative for malignancy. The urgent need for a liver allograft for the recipient due to the recipient's deteriorating medical condition was considered. Another set of pictures were sent to the staff surgeon showing the anatomy of the liver and showing that the lesion was resectable. At this point the decision was made to proceed with the transplant, as it was felt that the lesion could be resected from the liver allograft. This information was communicated to the family of the recipient and they supported the use of the liver graft. Lesion in left lateral segment of donor liver Measurement of lesion size Lesion after incision, showing calcification of the capsule of the lesion suggesting a chronic process

On the back table at the donor site a left lateral segmentectomy was completed using a linear cutting vascular stapler. A reduced graft orthotopic liver transplantation was then performed by a piggyback technique (Figure 4).
Reduced graft orthotopic liver transplantation in the recipient performed by a piggyback technique
The patient's postoperative course was relatively uneventful with no evidence of infection in the following five weeks. The patient was discharged from hospital and continues to do well.
The final pathology results on the lesion showed a thick sclerotic wall, densely adherent to the surface of the liver, with dystrophic calcification and collections of macrophages containing yellow pigment. No signs of malignancy were identified.
Discussion
The role of smart phones in medicine continues to grow. The present case illustrates how smart phones can be a valuable tool in performing real-time consultations. Previous authors have shown that direct, wireless cellular intraoperative communication improves communication times, communication accuracy, communication satisfaction, and minimizes intraoperative case interruption when compared to indirect, traditional pager communication. 5 In the present case, had the fellows not been able to interact with the staff surgeon in real-time during the surgery, there is a high likelihood that the organ would have been rejected by the staff surgeon due to the unexpected finding of a lesion at the time of procurement. The staff surgeon was able to adequately assess the situation and provide instructions to the fellows. Currently, our team are using smart phones to communicate during transplant organ procurement. We expect that the role of smart phones in remote consultation will continue to expand in future.