
Abstract
We studied 138 patients admitted for heart failure (HF). Patients were allocated one of three treatment strategies. Group 1 (G1, n = 50) were given usual care for HF, Group 2 (G2, n = 56) received a multi-disciplinary team approach, while Group 3 (G3, n = 32) had home telephone self-monitoring. Telemonitoring was based on the answers to three simple queries about bodyweight change, dyspnoea and general health. The system stratified the HF severity of each patient once a week, and recommended a prompt medical appointment or simple follow-up. Over a 12-month follow-up period, there were 43 adverse events (cardiovascular deaths and rehospitalizations for HF: G1 = 22, G2 = 14, G3 = 7). There was no difference between G2 and G3 (P = 0.78) but there was significant disadvantage with usual care (P = 0.02 vs. G2 and P = 0.04 vs. G3). Time to re-admission for HF increased in G2 and G3 compared to G1 (188 and 198 days vs. 95 days, P = 0.03 and P = 0.02 respectively). Automated home telephone self-monitoring reduced rehospitalization in patients with advanced HF.
Introduction
Heart failure (HF) is increasing due to the ageing population, the prevalence of hypertension and improved management of myocardial infarction. 1,2,3 After the first hospital admission for HF, 25% of patients are re-admitted within 12 weeks. 1 Hospitalization represents the main cost in HF and is associated with poor prognosis. 3 Patient education enables early detection of worsening chronic heart failure and repeated nurse-led home-based interventions reduce hospitalization rates. 4,5,6,7 Telephone-based monitoring also improves the quality of life. 8
Monitoring HF patients is part of health care and essential to good practice. 2 Several telemonitoring methods have been developed to detect symptoms or to monitor physiological variables via home devices in order to provide early warning of impending decompensation. 9,10,11,12 Many studies have demonstrated a reduction in all-cause hospitalization and mortality, while others have shown an increase in time to re-admission or improvements in quality of life. 4,7,8,10,13–15 Some telemonitoring programmes have found limitations such as the need for specific training, the lack of a patient-friendly interface, the time required to interact with the system and cost. 9,10,15,16
The aim of the present study was to assess the effect on cardiovascular death or re-hospitalization for heart failure of three different clinical management strategies: standard HF care, management in a HF clinic and home telephone self-monitoring.
Methods
We included all HF patients with left ventricular systolic dysfunction (LVEF <45%), recently discharged from hospital or diagnosed with acute or worsening HF up to three months before the study, between January 2007 and January 2008. We screened all patients during this period and all who were offered telemonitoring accepted it. All patients had diagnosed HF according to European guidelines. We excluded patients younger than 18 years old, patients with extracardiac co-morbidities or an estimated life expectancy of less than six months, and patients scheduled for cardiac transplant, left ventricular assist device, valvular surgery, percutaneous coronary intervention or cardiac resynchronization therapy. The study was approved by the appropriate ethics committee.
Study design
Consecutive patients were enrolled. They were allocated to three different groups for HF monitoring in a non-randomized fashion, see Figure 1. Those willing to be referred to their own cardiologist were in Group 1 and were given standard HF care management. Patients with no medical practitioner and who did not possess a scale and/or telephone at home were allocated to Group 2. These patients received a multi-disciplinary team approach during visits to the heart failure clinic. The remaining patients, who had no medical practitioner but had a telephone and scale at home, comprised Group 3. These patients were followed using our telemonitoring system (Telecard) in a home telephone self-monitoring approach.
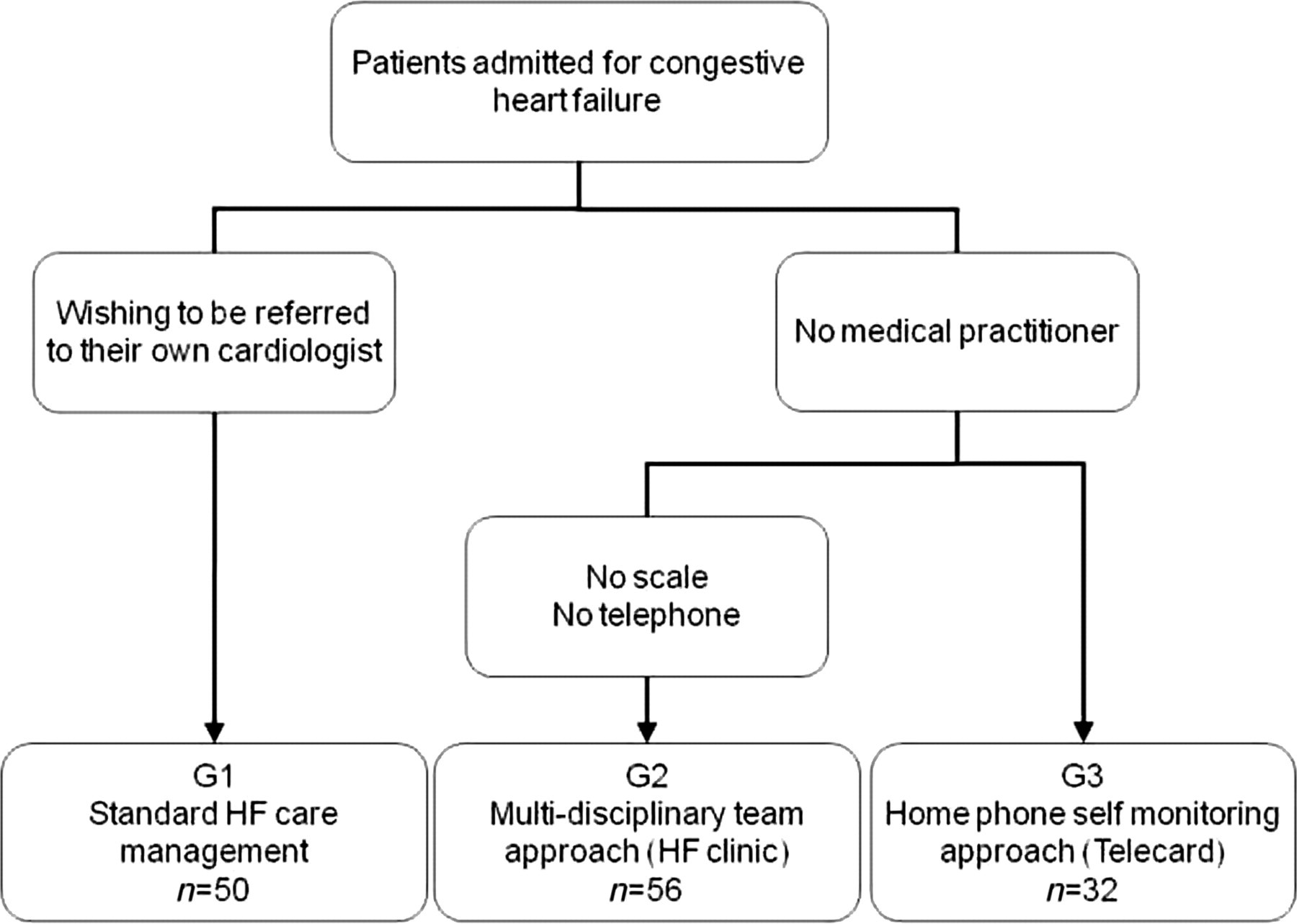
Treatment allocation; G1 = usual care management, G2 = HF clinic management, G3 = telemonitoring
Patients in G1 received standard care management from their general practitioner and cardiologist, without any intervention from the HF multi-disciplinary team. Patients had a specific treatment started at discharge from hospital without any further visit to HF clinic. No recommendations were made to practitioners, but they were invited to follow the European guidelines for the treatment of chronic heart failure. Patients in G2 were managed in a HF clinic by a multidisciplinary team of nurses, dieticians and doctors. During a 45-min consultation, patients were educated to understand their treatment plan, to adapt their preferred foods to low-sodium versions, to be familiar with effects and side-effects of major medicines, to monitor and attend their symptoms, to practice at least 30 min of aerobic activity per day on most days of the week, and to build up their activity level. We took advantage of the ‘I-care tool’ during ambulatory visits. 17 This consultation was repeated five or six times per year during face-to-face visits. If needed, patients were able to telephone the clinic and take advice from a care giver, usually a nurse. Patients in G3 were assigned to telemonitoring, and had only three planned visits to the clinic during a year.
Automated self-monitoring
Patients were asked to call an automated system once a week, to listen to the voice questions and to answer using the telephone keypad.
Guide Vocal-Web (Guide Vocal-Web, France Telecom, Orange Business Service, France) is software for specifying interactive voice dialogues between human and telephone. Briefly, using a computer linked to an Orange business website service, we edited three heart failure-related questions displayed in a tree manner with nodes. Questions were about change of weight, dyspnoea and general health condition (Figure 2). The text was then converted into a synthetic voice message.

Risk of worsening HF, estimated by the Telecard algorithm with 3 heart-failure-related questions: 0 points: recall within 7 days, 1 point: recall within 72 hours, 2 points: visit General Practitioner, 3 points or more: automatic call to HF clinic
Patients were able to listen to audio advice, inviting them to repeat their call after a week (stable patient), after three days (minor worsening HF), to proceed to a medical visit (suspected worsening HF), or they were directly connected to HF clinic care giver (high risk of hospitalization according to the algorithm).
Data collection and primary endpoint
At baseline, we collected demographic data and clinical data. In addition, a physical examination was performed by a cardiologist assisted by a specialist nurse. Patients were followed up for cardiovascular (CV) death, unplanned HF-related re-admission and time to re-hospitalization. We also collected the number of in-person visits to the HF clinic, and the number of calls transmitted to the HF clinic due to suspected worsening heart failure. The primary endpoint was CV deaths and hospitalization for HF, i.e. whichever event occurred first.
Statistical analysis
All data were analysed with a standard package (StatView). A proportional hazards Cox model was used for normally-distributed continuous variables. Kaplan Meier (log rank test) curves were constructed using time-dependent, all-cause survival and event-free survival data. It was followed by analysis with the Wilcoxon test of any differences in the number and timing of the events between the groups.
Assuming an endpoint frequency of 50% in the control group at one year for the composite outcome of CV death or re-admission for heart failure in the community, 18 we calculated that 26 patients would be required in each group for the study to have 80% power to detect an endpoint frequency of 16% in the telemonitoring group with a two-sided alpha level of 5%, using a log rank test. 9 Endpoints were assessed by telephone call and in hospital visit (emergency room, HF clinic visit or hospitalization for HF).
Results
Characteristics at baseline
We studied a total of 138 patients who were allocated to Group 1 (n = 50), Group 2 (n = 56) and Group 3 (n = 32), see Table 1. Overall, the mean age was 68 years (SD 11) and 78% were male. Ischaemic heart disease was the primary cause of heart failure followed by dilated cardiomyopathy. NYHA functional class II, III and IV were 54%, 42% and 4%, respectively. Mean left ventricular EF was 31% (SD 9), and the mean six-min walking test distance was 373 m (SD 125). Most of the patients received beta-blockers, ACE/AT2 inhibitors and diuretics. Cardiac resynchronization therapy was delivered in 27% of patients.
Clinical characteristics of patients at inclusion. Values are mean (SD)
ACE, angiotensin-converting enzyme; AT2, angiotensin-receptor type 2; NYHA, New York Heart Association
All groups were similar in their clinical characteristics at inclusion. Multivariate Cox model analysis showed no difference in dilated cardiomyopathy frequency (P = 0.06), NYHA functional class (II, P = 0.457; III, P = 0.64) and ACE/AT2 inhibitors medication (P = 0.07).
Telemonitoring data
The mean duration of the telephone calls was 48 s (SD 8). The overall number of telephone calls was 455/year, corresponding to 19 calls/year per patient. Out of the 455 calls, 27 were referred to the heart failure clinic because of a high probability of worsening heart failure according to the Telecard algorithm. The attrition rate was 0%, but the number of skipped or delayed telephone calls increased at follow-up, attaining 8% 12 months after inclusion.
Endpoint
During the 12-month follow up period, there were 11 deaths and 32 re-occurrences of HF necessitating hospitalization. Among the 27 calls that were referred to the HF clinic, 20 calls ended up with specific therapy adjustment preventing hospitalization, while seven calls necessitated hospitalization. Time to first event was significantly longer in the telemonitoring group as well as in the HF clinic group, compared to standard care (see Table 2). The time to first event was delayed by 10 days in the telemonitoring group compared to HF clinic management, but the difference was not significant.
Primary outcome measure and its components at 12-month follow-up
For primary endpoint, cardiovascular deaths and hospitalizations data are given as absolute values (expressed as a percentage of the number of patient in each group), for time to primary endpoint, data are given as mean (SD).
*P < 0.05 vs. usual care
† P < 0.05 vs. telemonitoring
There was a significant reduction in the primary endpoint in the telemonitoring group compared to standard care, but there was no difference between the HF clinic group and telemonitoring (Table 2). The risk reductions for the primary endpoint (CV death and hospitalization for HF) were 28% and 32% in the Telecard and HF clinic groups respectively, compared to the standard care group. However outcomes in isolation showed only a difference in hospitalization rate, but not for cardiovascular deaths.
Actuarial plots of time to event (i.e. the percentage of patients free of an event) showed no difference between telemonitoring and HF clinic management (P = 0.78). There was a significant benefit on composite endpoint for re-hospitalization or CV death when both were compared to standard management (P = 0.02 vs. HF clinic and P = 0.04 vs. telemonitoring, Figure 3).
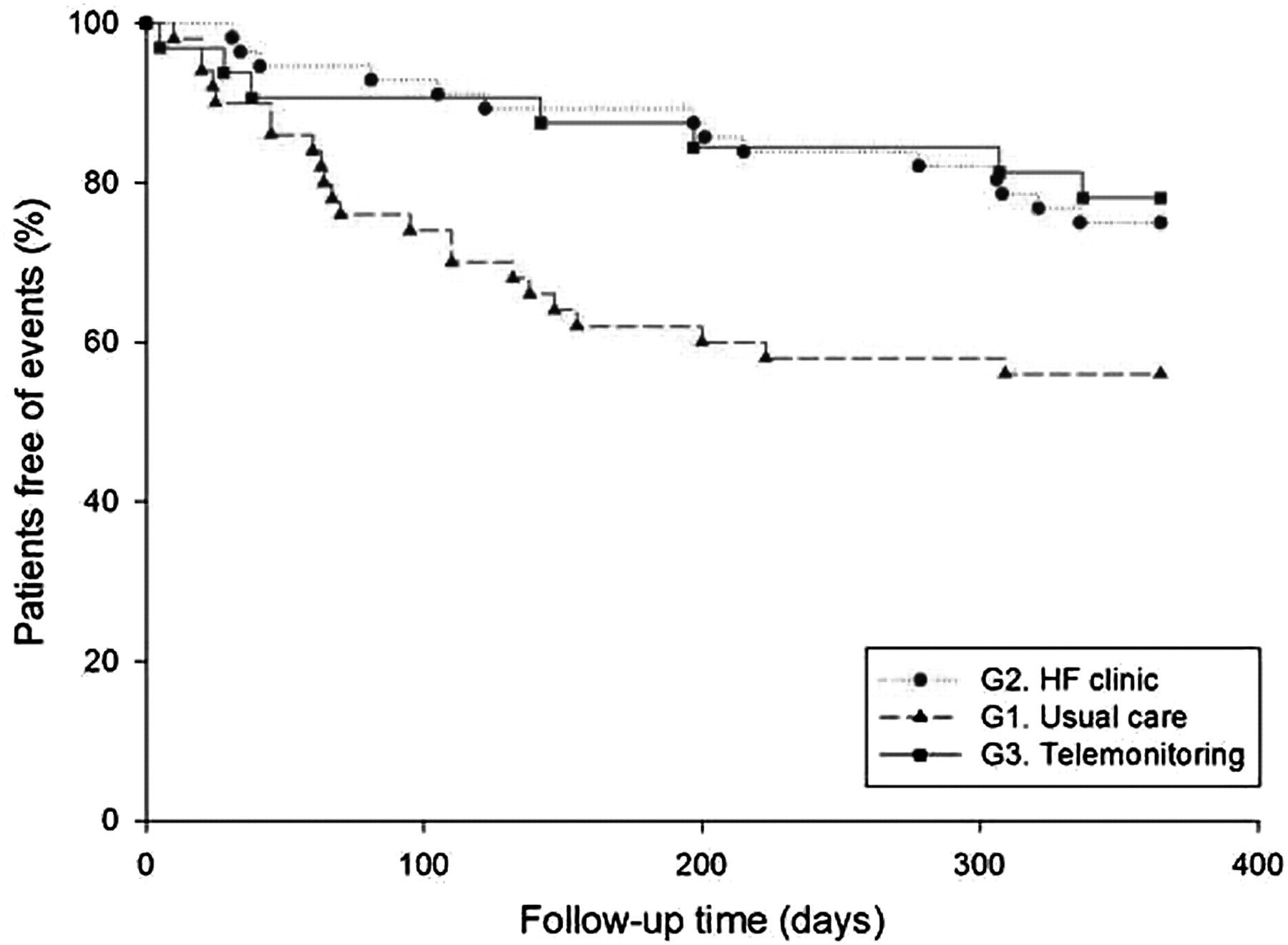
Percentages of patients free of an event (cardiovascular death or hospitalization for HF). Risk reductions for primary endpoint (cardiovascular death and hospitalization for HF) were 28% and 32% in the telemonitoring and HF clinic groups respectively compared to the standard care group. Telemonitoring vs. HF clinic management, P = 0.78; Telemonitoring vs. standard care, P = 0.04; HF clinic management vs. standard care, P = 0.02
Discussion
The present study suggests that automated home-based telephone self-monitoring may be an effective method of reducing the risk of CV death or re-admission for heart failure in high-risk patients. It appears to be similar to active HF clinic management. Most of the benefit from telemonitoring was in fewer HF re-admissions and not in mortality reduction.
Telemonitoring in heart failure
Telemonitoring, as a tool to detect moderate HF decompensation early, can notify the medical team before patients become refractory to ambulatory management. Table 3 summarizes several telemonitoring studies. Despite advantages in HF outcomes, improved feasibility, user-friendly technology and acceptable training information for patients and their families, telemonitoring in HF raises several questions. 11
Telemonitoring in heart failure
ACE, angiotensin-converting enzyme; AT2, angiotensin-receptor type 2
First, many systems require interaction between the patient and a computer, e.g. the InSight Telehealth system. 15 However, the mean age in this study was 54 years, while HF patients are usually older, especially the population mainly at risk of HF reoccurrence. 1 Riegel et al. failed to demonstrate a benefit in nurse telephone intervention provided during six months in poorly educated people (78% less than a high school education). 16 Elderly or indigent people may feel uncomfortable with the use of a computer, because of a lack of experience or knowledge.
Second, all systems are technically elaborate 9,10 and therefore relatively costly. Third, in many cases training is necessary, time-consuming, and involves relatives before routine use. However not all telemonitoring systems are complex. For example, the electronic scale used in the WHARF trial was easily manageable in a telemonitoring environment and did not require specific training. 10 Fourth, many telemonitoring systems require frequent nurse interventions 4,7,14 and some studies of nurse-based programmes have found negative effects on mortality and re-hospitalization. 19
We therefore designed the Telecard system to avoid problems raised by the previous techniques. 9,15,20,21
Telecard
The Telecard monitoring system was user-friendly. Because it used a conventional telephone, it did not require specific training. Simplicity is crucial for adherence, particularly in elderly, indigent or socially isolated patients. Telecard was also inexpensive. The cost per telephone call/patient was about 0.08 € and registration for the provider was 189 € per month (France Telecom fees).
Although we had no patient rejections, some patients progressively skipped one or multiple telephone calls. Investigators were informed weekly by FranceTelecom. When a patient missed a weekly telephone call, the software sent them a reminder. Missing a telephone call could be interpreted as a technical problem of the system, or simply that patients were unwilling to call the server once a week.
Our findings are consistent with recent systematic reviews and meta-analyses from Clark et al. as well as Inglis et al. which concluded that structured telephone support and telemonitoring are effective in reducing the risk of all-cause mortality and CHF-related hospitalizations. 22,23 We found a 28% reduction in re-hospitalization at one year. Others have reported a 48% reduction in re-admission at six months. 7 The apparent inferiority of our study is explained by a different design with longer follow-up meaning additional endpoints in all groups, different endpoints and less continuous education, whereas patients received 16 hours of a case manager's time in Riegel et al.'s work. 7
Our study was a prospective, non-randomized pilot trial and we acknowledge this as a limitation. Nonetheless, the results are encouraging and the simplicity and affordability of our system could encourage its widespread use, at every stage of heart failure.