
Abstract
Telemedicine has been used in the Solomon Islands since 2000. We used quantitative and qualitative methods to examine telemedicine use in the Solomon Islands from January 2006 to June 2009. During the study period 66 telemedicine cases were submitted to the store and forward telemedicine system being used there. These included orthopaedic, oncology, cardiothoracic, infectious, congenital, gastroenterology and dermatology cases. Most cases (52%) were submitted by doctors at the National Referral Hospital (NRH) in Honiara. The majority of responses came from the NRH (27%). A final, firm recommendation regarding patient diagnosis and/or care was given for 46% of the cases. Interviews were conducted with 23 stakeholders in the Solomon Islands and in Australia to better understand the current and future use of telemedicine. The interviews identified the fragility of the Solomon Islands infrastructure, including the lack of training, as the largest barrier to the future use of telemedicine. The best use of telemedicine appears to be case sharing within the Solomon Islands, with connections to clinicians in other countries as a secondary benefit when particular expertise is required.
Introduction
The Solomon Islands is a country of 595,000 people who live on 350 islands in the south-west Pacific. 1,2 There is a shortage of health-care workers, and in 2009 there were 89 physicians, 620 nurses and 74 midwives in the Solomon Islands. 3 This represents approximately 0.2 doctors and 1.0 nurses per 1000 population, which is well below the 2.4 health workers per 1000 population needed to sustain basic health services according to the World Health Organization (WHO). 4
The National Referral Hospital (NRH) in Honiara is the largest hospital in the Solomon Islands with 400 beds and specialist services. There are seven provincial hospitals which offer secondary level care. Nursing stations provide the majority of primary health services to the predominantly rural population of the country. Poor rural services and disproportionate allocation of staff and funds to the tertiary care hospital in Honiara leave outer island communities with insufficient access to primary, secondary and tertiary care. Telemedicine may be helpful for improving access to health care in the Solomon Islands.
Telemedicine in the Solomon Islands
An early telemedicine project commenced in the Solomon Islands in March 2000 in the Gizo and Helena Goldie Hospitals, initiated by a visiting British medical student using a PC and digital camera and linked to the Swinfen Charitable Trust (SCT) telemedicine network. 5,6 The SCT network was established in 1998 and was first used in Bangladesh, then expanded to Nepal and the Solomon Islands. 6 The SCT network received telemedicine referrals from the Solomons by email for about five years, but they ceased in 2004. 7
The iPath system, developed by the University of Basel, 8,9 was first used in the Solomon Islands in 2001. It was a web-based system, initially set up for telepathology. 10 It fell out of use but was revived in 2006 by MedTech Outreach Australia in collaboration with the Consul of the Solomon Islands in Sydney, Australia. It connects clinicians to other clinicians within the Solomon Islands, and also connects them with colleagues in Australia, Switzerland and other countries.
We have reviewed the recent use of the iPath system in the Solomon Islands.
Methods
Quantitative and qualitative approaches were employed. A quantitative analysis was performed of the data posted to the iPath system. Qualitative interviews were conducted to understand clinician's and decision-makers’ views of telemedicine.
Because of the relatively small population of the Solomon Islands, care was taken to ensure the ethical and confidential reporting of any telemedicine data. Patient information is stored on the telemedicine system using unique identifiers to preserve confidentiality and the analysis was based on these identifiers. Any quotations were rendered gender neutral and organization names were removed to preserve confidentiality. The present study was approved by the appropriate ethics committee.
Use of the telemedicine system
Descriptive analyses were employed to summarize the use of the telemedicine system for the period 25 January 2006 to 22 June 2009. A standard data collection template was developed prior to data collection. A researcher coded the data from the telemedicine website onto a data collection form. All entries were double checked for accuracy. A quantitative analysis was then conducted for three types of variables, related to: (1) the health provider, i.e. doctor, (2) the patient and (3) the telemedicine system. The health provider-related variables included who used the telemedicine system, where messages originated (clinical specialty and geographical area) and where responses originated. The patient-related variables included age, gender and clinical problem. The telemedicine system-related variables included the number of cases and responses, the timeline, number of second opinions provided and the characteristics of the cases (e.g. text only or with photographs).
Interviews
Qualitative interviews were conducted in the Solomon Islands in September 2009 and in Australia between June and September 2009. Twenty-three people were interviewed from the following groups: doctors from the Solomon Islands, doctors from Australia, staff from the Solomon Islands Ministry of Health, Solomons Telecom, the WHO, AusAID, People's First Network (PFNET) and the Distance Learning Centers, and the Secretariat of the Pacific Community (SPC). Interviews were conducted at three locations in the Solomon Islands (Honiara, Munda and Gizo) and at two locations in Australia (Brisbane and Sydney). These locations were selected as they were the origin of most telemedicine cases.
The interviews lasted for about 45 min and used open-ended questions. Data collection continued until data saturation was reached. Key themes from the interviews were summarized and checked by the responders to ensure that the recorded information was accurate. Solomon Island costs were expressed in US$ using 2009 exchange rates.
Results
Quantitative findings
During the study period 82 cases were submitted to the telemedicine system. However, 16 of these cases were not Solomon Islands related (15 cases were from the Ukraine, 1 from Russia). Thus, the following analysis is based on the 66 cases originating in the Solomon Islands.
There were 17 cases in 2006, 19 in 2007, 22 in 2008 and eight in the first six months of 2009. Most cases were males (62%). A total of 17 doctors referred at least one case during the study period. This represents 20% of all doctors recorded as working in the Solomon Islands. The mean age of the patients was 25 years (range newborn–78 years). In 59 cases (89%) there were photographs or radiographs attached. Detailed case histories were provided for 61 of the cases (92%) but were missing in five.
There was a range of patient problems (Figure 1). The most common conditions were orthopaedic, which represented 27 (41%) of the cases. Of the 27 orthopaedic cases, eight were fractures, six deformities, three dislocations, six inflammatory/arthritic and four were malignant. Several of the cases were paediatric conditions, including pneumonia/malnutrition, fractures (femur, forearm), cancer (e.g. bone cancers) and congenital conditions.
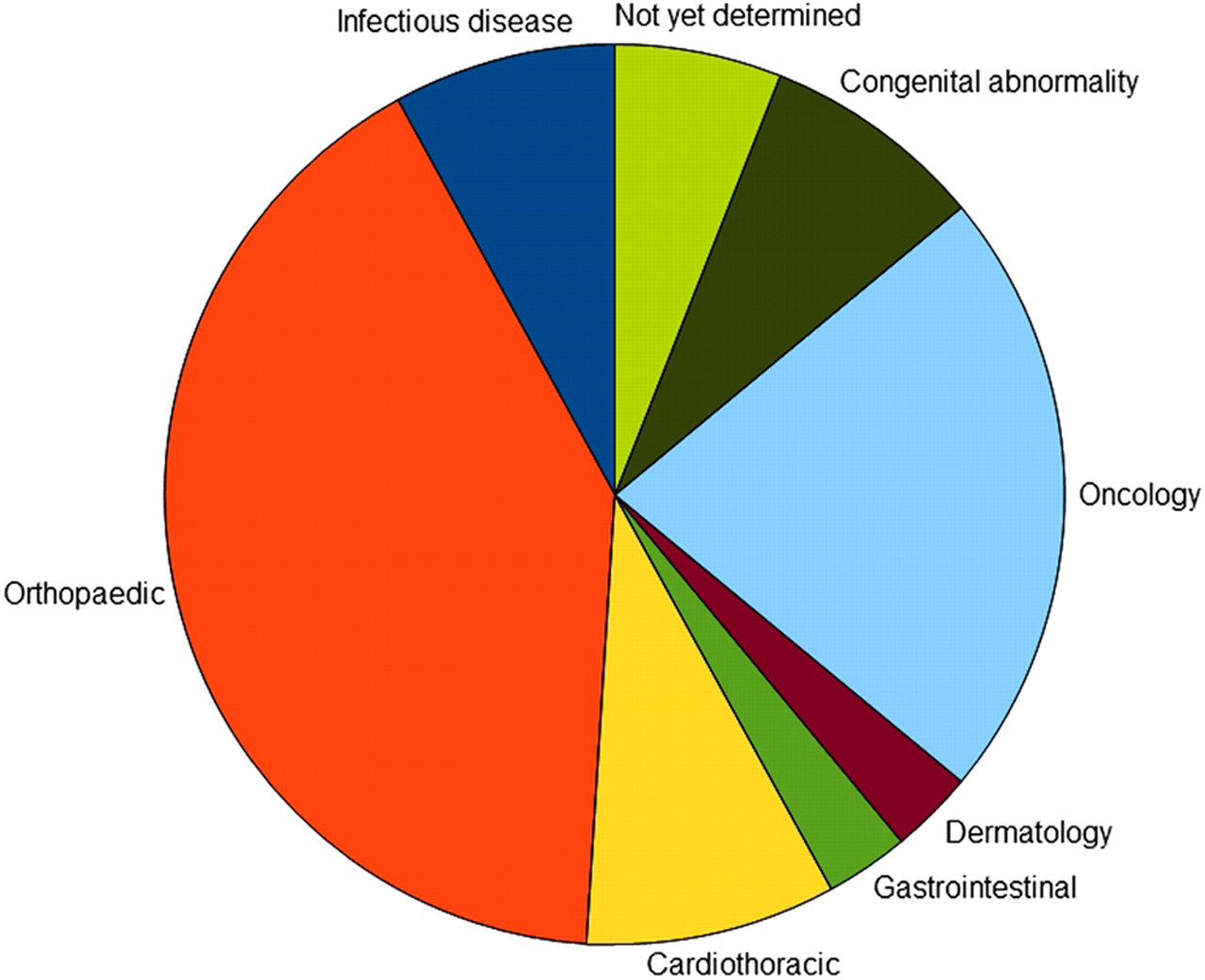
Diagnoses (n = 66)
When using the telemedicine system, referrers submit the case to a specific discussion group (Table 1). Most cases had been submitted to the orthopaedics group (25 cases; 38%), with the next most common group being the inter-island group (15 cases; 23%).
Type of cases, i.e. the group to which the referrer submitted the case
Since the iPath system is accessible via the web, cases can be responded to by health professionals from any country if the individual has access rights to the system. During the initial registration step, system users must enter their institution and specialization. However, there is no mechanism to ensure that the qualifications claimed are legitimate. During training, clinicians referring cases to the system are informed that they remain responsible for patient care, i.e. the telemedicine system provides them with advice.
The telemedicine system received cases from hospitals in the Solomon Islands, and also from Australia where Solomon Islands patients occasionally receive care through a memorandum of understanding between St Vincent's Hospital in Sydney and the NRH. The majority of cases were submitted by physicians at the NRH (52%) with the next most common being Gizo (26%) (Table 2). Cases can be sent to a specific user for reply, or sent to the wider network for anyone to respond. Most cases were addressed to the generic group ‘iPath’ or ‘telemedicine platform’ where anyone can respond.
Origin of the cases
The location of the first responder is shown in Table 3. The majority of responses came from the NRH in Honiara (18 cases; 27%) and the next most common responses did not provide a location (17 cases; 26%). Most cases received two or three responses (23 cases; 45% and 14 cases; 21% respectively), see Table 4. There were also 10 cases which received no responses (15% of total). There was no obvious reason why these 10 cases received no responses.
Location of the first person responding to the case
Number of responses to each case
Cases can receive comments from more than one clinician. In 13 of the cases, a single clinician responded (20% of cases). However, for 24 cases there were responses from two clinicians (36%) and in 13 cases (20%) three clinicians responded. A final, firm recommendation regarding patient diagnosis and/or care was given for 30 (46%) of the cases. The other cases were discussed but no firm recommendation was given.
The mean time from the first submission until a response was received was eight days (range 1–67).
Qualitative findings
Internet access was available at hospital sites at a cost of US$486 per month for 512 kbit/s bandwidth. Access at Gizo Hospital was half this speed. Interviews with Ministry of Health IT staff indicated that the NRH had 100 PCs, of which approximately 60% could connect to the Internet. Gizo Hospital had 15–20 PCs connected to the Internet and Kalufi Hospital had 1–2 PCs connected to the Internet.
The relatively slow Internet connections, high costs, poor IT infrastructure and limited IT human resources curtail the use of telemedicine in the Solomon Islands. In larger centres such as Honiara, some clinicians pay for Internet connections at home because they cannot rely on the hospital IT systems. Many remote hospitals have limited Internet and electrical power. In remote locations a group called PFNET uses a solar powered HF Radio Base to provide Internet access.
The iPath system appears to be sufficient for present telemedicine needs and is relatively simple to use. Nonetheless, some interviewees stated that they used email instead of the telemedicine system to contact colleagues about cases. These people saw email as more consistent and personal. However, the free text format of emails means it is more difficult to ensure that the relevant patient information is transferred in the correspondence. 11
Costs and benefits of telemedicine
Interviewees who were familiar with the NRH budget estimated that about 15% of the annual total health-care budget (approximately US$1.2 million per year) was spent on transporting patients back to their home villages after receiving care in Honiara. Inappropriate patient transfers and arrivals could be reduced by improved communication and/or telemedicine. The high transport costs are contributed to by patients who ‘get sick so they get a free flight to visit relatives’ according to interviewees. Another interviewee estimated that clinically, about half of these patients did not need to go to Honiara for care, but because of poor communication with the NRH, these patients arrived with a condition that could not be treated at the NRH or that could have been treated in their local facility. It was also estimated that about US$750,000 (US$1 ≈ AUS$1) was spent in transferring patients to Australia for care. One interviewee said that some of the patient transfers and costs of accommodation could be prevented by telemedicine. Improved communications using telemedicine are expected to improve referrals to Honiara, which was cited by interviewees as ‘a key policy issue’.
Human resources and telemedicine
Telemedicine has the potential to improve access to unevenly distributed resources. For instance, interviewees cited particular clinical areas that would benefit from telemedicine: ‘there is one psychiatrist and one pathologist in all of the Solomon Islands – so yes, telemedicine is needed’.
Several interviewees mentioned that the use of telemedicine was haphazard. The connections typically were based on personal links between individuals rather than being institutionalized. For instance, the good relationship between the NRH and St Vincent's Hospital in Sydney was largely due to the strong engagement of the Consul General in Sydney. Interviewees emphasized that this was not likely to be a sustainable approach. There were also problems caused by the high turnover of health-care and IT staff. The high turnover of staff means that new staff are rarely trained in IT or the telemedicine system.
Interviewees also noted that ‘user education on computers is needed – for instance people don't even know to try re-booting the computer if there is a problem.’ Another interviewee noted that ‘at one point, the Permanent Secretary for Health had 15 active email addresses’, that ‘the two Ministry of Health IT staff are swamped by telephone calls about user problems’ and thus cannot address larger, system problems such as firewalls, viruses or database use. Internet use has also been slow due to many staff using Internet bandwidth to download personal material such as music or photographs. Many interviewees noted that nurses have not been trained to use computers or the telemedicine system, yet they run most of the clinics on the remote islands which would be the ones most likely to benefit from telemedicine.
The Solomon Islands health-care system is assisted by visiting health-care workers, often arriving for short-term surgical missions. Interviewees felt that the telemedicine system might have a role to play in preparing visiting clinicians for their arrival as well as providing a more continuous quality of care after their departure. In particular, interviewees recommended that more of their colleagues from Fiji and Papua New Guinea visit the Solomon Islands to share their skills and that these colleagues should use the telemedicine system to refer cases as well as respond to cases on the system. These colleagues were felt by interviewees to be an important missing component to the telemedicine system because they were often skilled and also had local knowledge about endemic conditions.
Australian user perspectives
Most of the Australian doctors who contributed to the telemedicine system had visited the Solomon Islands. Their contributions were voluntary. On average, Australian interviewees estimated that responding to a telemedicine case took 30 min and could be done within 1–2 days of the original submission in the Solomon Islands. Difficulties with using telemedicine were that images submitted with the case history were often photographs of X-rays and thus of poor image quality. In addition, some cases were complex and so it was difficult to reach a diagnosis. Australian interviewees noted that few clinicians had explored the professional liability and medical indemnity associated with participation in an online telemedicine forum.
Discussion
Telemedicine has been used in the Solomon Islands since about 2000. Although it is deemed useful, the use of telemedicine has not increased since 2006 but instead has remained constant. This is believed to be because of the fragile IT infrastructure of the country, where Internet availability is inconsistent which means that telemedicine cannot be relied on. Also, few clinicians know that the telemedicine system exists or know how to use it. However, IT capability in the Solomon Islands is developing.
One strength of telemedicine in the Solomon Islands is the use of strong personal relationships for liaison between clinicians. Interviewees noted that individuals were unlikely to use telemedicine to create a new working relationship, but they would use technology to maintain existing relationships. In the future it is hoped that telemedicine will assist in the referral of patients within the Solomon Islands and also help when Solomon Islanders receive care in Australia. However, we recommend that telemedicine use should focus primarily on inter-island communications to harness the specialists in Honiara and beyond to improve the quality of care in outer islands.
The main barriers to telemedicine in the Solomon Islands appear to be computer access and Internet connectivity. These are barriers that were highlighted in the year 2000 and thus it appears that little has changed since then. 12 There is however now a focus on ‘e-readiness’ in low-and middle-income countries (LMICs), i.e. the state of a country's information and communication technology (ICT) infrastructure, and the ability of its consumer, businesses and governments to use ICT for their benefit. 13 Another barrier to the use of telemedicine in the Solomon Islands is training. Starting to use telemedicine takes more time than people expect. 13 Since there are limited human resources available for patient care in the Solomon Islands, this is another barrier to the use of telemedicine. Potential future barriers are the ethical and legal considerations, where little investigation has yet occurred. A final barrier to the use of telemedicine is its reliance on personal links between clinicians.
Previous publications
Brauchli et al. (2004) summarized iPath data from the Solomon Islands for a period of over two years. A total of 333 pathology consultations were performed and 94% of the cases were diagnosed by a remote pathologist. 10 This helped to reduce the time for pathology evaluations from 28 h to 8.5 h for a preliminary diagnosis, and to 13 h for the final report. Our findings in the present study match the findings about telemedicine use in other developing countries. In particular, we observed a rather static rate of referrals, which may be because clinicians are too busy to use telemedicine. 7
Strengths and limitations
The present study was strengthened by its use of mixed methods to capture both quantitative and qualitative data. A limitation was that it could not describe patient outcomes following recommendations given by telemedicine. It was also unable to assess whether telephone calls or personal email messages were sent in conjunction with cases sent to the telemedicine system, or what the outcomes were for patients referred by these methods instead of telemedicine.
Recommendations
Several recommendations arise from the present study. First Internet access and the infrastructure of local IT systems should be improved. Plans are required for purchasing computers, software, controlling humidity and training IT staff. There is also a need for quantifiable goals for outputs, outcomes, impacts and measurements of process including guidelines for confidentiality and an economic analysis (how much is spent and saved using telemedicine). If an economic analysis proves positive, then the costs of telemedicine might be met by the government. Plans for telemedicine should take into account human resource planning and the urban/rural dispersion of staff. The interviewees recommended that telemedicine should focus on the NRH, Kalufi and Gizo hospitals initially. They also emphasized that telemedicine should focus on case sharing within the Solomon Islands, with connections to clinicians in other countries as a secondary benefit when particular expertise was required.
A telemedicine administrator would be useful. The interviewees recommended that telemedicine should be promoted in the Solomon Islands, e.g. pamphlets could be distributed explaining what telemedicine can be used for and with short instructions about how to use it. Staff who are in charge of the radios on remote islands could be trained to be Internet staff (i.e. to mend hardware and software, and maintain connectivity). Future research should examine the medical, ethical and legal perspectives and perhaps derive guidelines or codes of practice for telemedicine.
In conclusion, a long-term sustainable partnership among clinical telemedicine ‘champions’, the Ministry of Health and IT staff would facilitate the development of telemedicine in the Solomon Islands.
Footnotes
Acknowledgements
We thank Sir Trevor Garland, Consul of the Solomon Islands to Sydney, Australia for his support and the developers of the iPath telepathology software at the University of Basel. Alexandra Martiniuk was supported by a Canadian Institutes of Health Research Fellowship. Funding for data collection and for travel to the Solomon Islands was provided by Rotary International (Sydney Cove Club).