
Abstract
We conducted a randomized controlled trial to investigate the efficacy and safety of a system for online glucose monitoring of type 2 diabetes patients. The software automatically filtered the self-monitored blood glucose data to reduce physicians' time. In the control group, the physicians had to contact the patients manually. We measured the time spent by physicians for online management in a 24-week study. Seventy-nine patients were recruited. The frequency of physicians' online monitoring of the patients was decreased by 55% in patients with HbA1c ≤ 6.5% and by 29% when HbA1c > 6.5% (P < 0.01). Physicians' log-in time was reduced by 67% and 55% in patients with HbA1c ≤6.5% and >6.5%, respectively (P <0.05). HbA1c levels were maintained at <6.5% during the study period in both groups. The study showed the efficacy and safety of the software for online communication in diabetes management. The results suggest that it could improve the cost-effectiveness of online communication systems and form the basis of future clinical applications.
Introduction
Type 2 diabetes mellitus is a serious, costly disease affecting about 8% of adults in the USA. 1 The International Diabetes Federation has predicted that the number of individuals with diabetes will rise from 240 million in 2007 to 380 million in 2025. 2 The diabetic population is increasing sharply, especially in Asian countries and in young people. 3,4 Current methods for treating diabetes, such as face-to-face outpatient management, remain inadequate, and new ways are needed to achieve the HbA1c targets. Recent reports show that interactive communication between caregivers and patients through the Internet or telecommunication are effective in diabetes management. 5–18
Compared to conventional outpatient-based care, information technology-based communication systems have the additional benefits of providing seasonal advice and feedback in near realtime, allowing continuous motivation for glucose monitoring, frequent encouragement, problem assessment and individualized practical education about diet, exercise and drug modification. 5 However, implementing an interactive communication system for diabetes management in real clinical practice requires the demonstration of its cost-effectiveness. The first important step in reducing the cost is to minimize the physicians' time required. In other words, supportive software is needed that requires less physician time and effort, and its effectiveness and safety must be demonstrated in practice. We have developed a monitored glucose data-filtering system called SAVE (System for Automatic Verification).
The present study was designed to answer the following questions. First, does the SAVE reduce medical staff time? Second, is its effectiveness for glucose control equal to that of the manual review system developed previously by our team, the Internet-based glucose monitoring system (IBGMS)?
Methods
A randomized controlled trial design was used. We invited patients who were registered with Seoul St Mary's Hospital to participate.
Participants
Eligibility criteria included men or women aged 20–70 years, who had had type 2 diabetes for more than one year. Only those whose baseline HbA1c was 6–10% and had used the diabetes management website (
All patients provided written informed consent to participate, and the study was approved by the appropriate ethics committees.
Design
Each participant was assigned to the intervention group or the control group by adaptive randomization. The intervention group used the algorithm-based SAVE with glucose decision software in an Internet-based interactive communication system. The control group had no access to the SAVE.
At the initial interview, body weight, height and blood pressure were checked. Laboratory tests included HbA1c, fasting and postprandial plasma glucose, lipid profile, serum blood urea nitrogen and creatinine. Every screened patient was explicitly told that dietary modification and increased physical activity had been proven to reduce the risk of diabetes complications. Participants were re-educated in how to use the IBGM system and how to perform SMBG according to practice guidelines. The patients visited the outpatient clinic 12 and 24 weeks after randomization unless they had serious hypoglycaemic events or acute illnesses. At the visit, HbA1c, fasting plasma glucose and the lipid profile were measured.
Intervention
The patients sent information about their SMBG before and after eating, and sent drug information including the types and dosages of insulin and oral antidiabetic agents (OAD). The patients communicated with the medical team only via the Internet with their individualized electronic chart system. The telephone was not used for follow-up. Advanced practice nurses checked participants' data from the website and provided routine recommendations to the participants if SMBG was not measured when required or when hypoglycaemia occurred. Hypoglycaemia was defined in terms of an SMBG level of less than 2.78 mmol/L. The doctor sent participants in the control group a recommendation through the Internet once every other week. In the intervention group, the SAVE engine screened the uploaded SMBG data according to the decision algorithm (Figure 1) and then sent a text message automatically to the patients with good glucose control. The SAVE engine reported to the doctors any patients with poor glucose control or with inadequately uploaded glucose monitoring data.
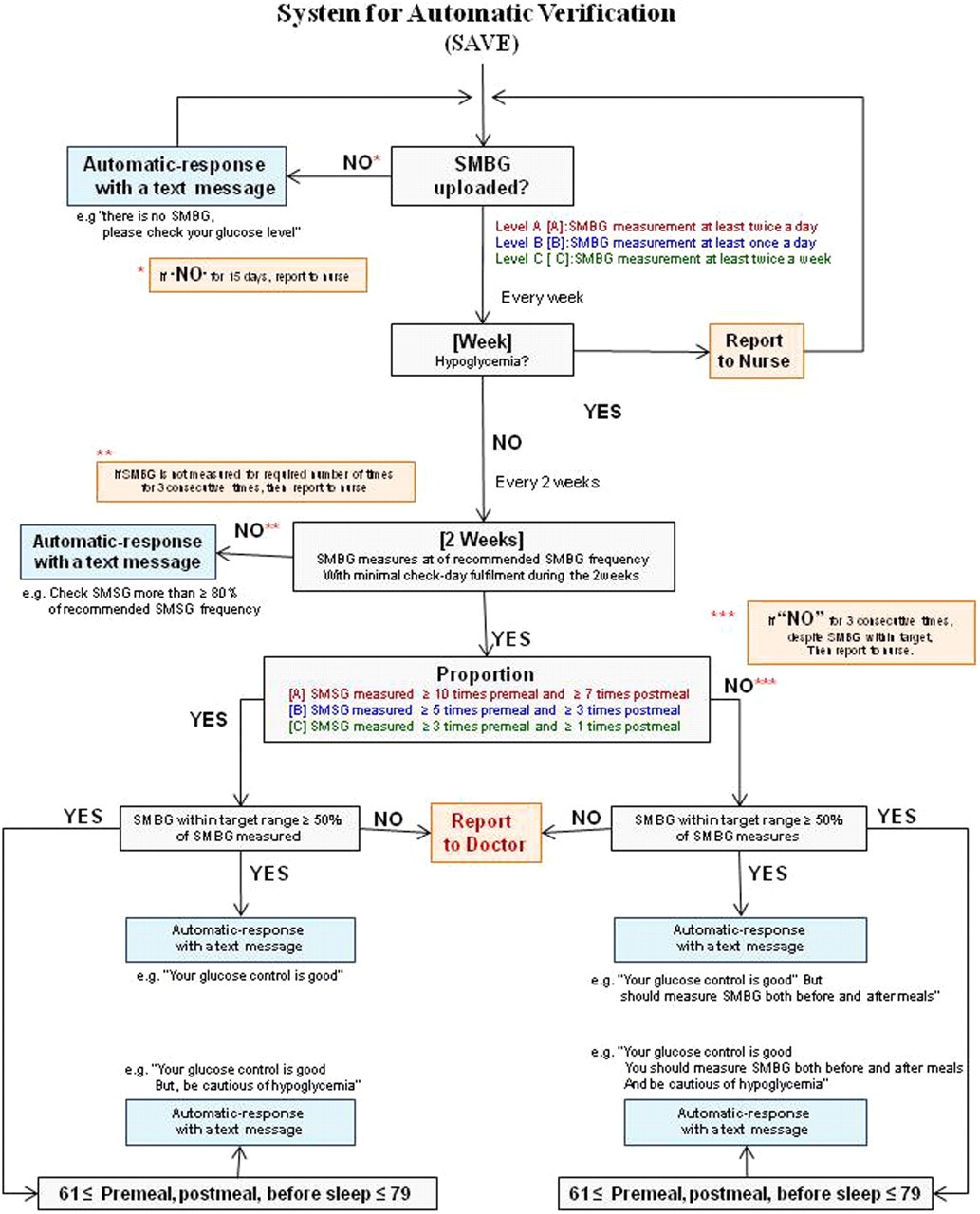
Decision algorithm of the SAVE engine
SAVE software
The clinical decision-support system could identify glucose data recorded by patients and make decisions accordingly. The SAVE engine assigned subjects to one of three levels according to the glucose control status and method. We defined a patient's SMBG frequency according to the level of control at the study enrolment. We reassessed and reassigned at the end of 12 weeks according to the HbA1c and mode of treatment. Patients in the severe group (level A), who were treated with insulin with/without OAD and whose HbA1c was >6.5%, were told to perform SMBG at least twice a day. Patients in the moderate group (level B), who were treated with insulin with/without OAD and whose HbA1c was ≤6.5% or who were treated with OAD and their HbA1c was >6.5%, were recommended to perform SMBG once a day. Patients in the mild group (level C), who were treated with OAD and whose HbA1c was ≤6.5% or were managed non-pharmacologically, were told to perform SMBG at least twice a week.
Outcome measures
We measured physicians' labour time and frequency of contact with the online communication system required for reviewing the patients' information and sending recommendations. We defined the labour time as the physicians' log-in time from reviewing each patient's SMBG data to sending recommendations through the online system. Software embedded in the server automatically measured the log-in time of each physician whenever the physician logged in for each patient. Time for reviewing patients' personal information and answering their questions was not included in the log-in time. For the secondary outcome, we measured HbA1c at baseline and at 12- and 24-week follow-up.
Statistical analysis
Baseline characteristics were compared between groups using χ2-tests of independence and t-tests for continuous variables, after assessment for normality. We examined the difference between groups in physicians' log-in time and HbA1c from randomization to the end of the trial using an unpaired t-test. We also analysed the changes in within-group means of HbA1c, fasting and postprandial glucose levels and lipid profile from baseline to the end of the trial using paired t-tests. The differences in the mean values for the frequency of SMBG were also examined with t-tests. Unless noted, all analyses were conducted by applying intention-to-treat methods with baseline values carried forward for missing values. Data were analysed using a standard package (SAS, version 8.2).
Results
We screened 120 patients. Twenty-three patients were excluded based on age and duration of diabetes. A further 10 were ineligible because of their HbA1c level. Eight patients who used intensive insulin therapy were also excluded. Seventy-nine patients participated in the study and were assigned randomly to the two groups. Their baseline characteristics are shown in Table 1. Two subjects in the SAVE group and two in the control group did not complete the study, so that 36 in the SAVE group and 39 in the control group were included in the analyses. The baseline characteristics of the two groups were similar, although BMI and triglyceride were higher in the control group. However, these patients were not obese and triglyceride was still within normal range. The diabetes control methods did not differ significantly between groups.
Baseline characteristics of the participants
Therapeutic effect
Patients with baseline HbA1c ≤6.5% in both groups maintained their HbA1c at <6.5% during the study period of 24 weeks despite a slight increase in HbA1c between the baseline and 24-week follow-up (6.0 to 6.4% for the SAVE group; 6.1 to 6.4% for the control group; P < 0.01 for both).
HbA1c was also maintained in patients with baseline HbA1c >6.5% in both groups, although there was a tendency to increase between the baseline and 24-week follow-up (7.3 to 7.7% in the SAVE group, P = 0.062; 7.4 to 7.7% in the control group, P = 0.074). Postprandial glucose level decreased significantly at the 24-week follow-up in patients with baseline HbA1c ≤6.5% in the control group. The lipid profile did not differ significantly between the baseline and follow-up in either group except for LDL-cholesterol in SAVE group with baseline HbA1c ≤6.5% (Table 2).
Change in glucose control status and lipid profile
*P < 0.05 within group
†P < 0.01 within group
SMBG recording
In patients in the two groups with baseline HbA1c ≤6.5%, the total SMBG frequency per patient for 24 weeks was 225 (1.33 per day) and 211 (1.25 per day) in the SAVE and control groups, respectively; the frequency did not differ significantly between groups. However, in patients with baseline HbA1c >6.5%, the frequency was 202 (1.2 per day) in the SAVE group and 127 (0.75 per day) in the control group (P < 0.05). In patients with baseline HbA1c ≤6.5%, post-lunch SMBG frequency per patient for 24 weeks was 30.9, while those with baseline HbA1c >6.5% was 10.2 (P < 0.05). In the SAVE group, 71% of total SMBG was performed before meals and in the control group it was 69% (P = 0.657). In the SAVE group, 64% of total pre-meal SMBG was performed before breakfast and in the control group it was 64% (P = 0.968). The frequency of hypoglycaemia per person for six months was 0.4 and 0.9 in subjects with baseline HbA1c ≤6.5% in the SAVE and control groups, respectively (P = 0.565). In patients with a baseline HbA1c >6.5%, hypoglycaemia was experienced at a frequency of 1.5 per person for six months in the SAVE group and 1.3 in the control group (P = 0.862).
Patients' time
Patients with baseline HbA1c >6.5% in the SAVE group logged in to their web-chart at a frequency of 37 times per 24 weeks and spent 3552 s per patient over 24 weeks. The values in the control group were 15 times and 2501 s reviewing their web-chart and recording their glucose data. In contrast, patients with baseline HbA1c ≤6.5% in the SAVE and control groups used their web-chart at a frequency of 39 for 24 weeks and 19, respectively (P = 0.329), and spent 12714 s and 17075 s for 24 weeks using the online system (P = 0.867). The SAVE group had a greater tendency to log-in to the system compared with the control group.
Feedback to patients
During the 24 weeks, the SAVE software sent an average of 25 automatic recommendations per patient to participants with baseline HbA1c ≤6.5% and 50 to those with baseline HbA1c >6.5% (P < 0.05). The study protocol meant that no automatic messages were sent to patients in the control group. In the SAVE group, patients with baseline HbA1c ≤6.5% received an average of 5.3 recommendations per patient from the physician, and patients with baseline HbA1c >6.5% received 8.7 recommendations (P < 0.01). In the control group, physicians sent 11.1 recommendations per patient to participants with baseline HbA1c ≤6.5% and 11.3 to those with baseline HbA1c >6.5% according to the protocol (Figure 2).
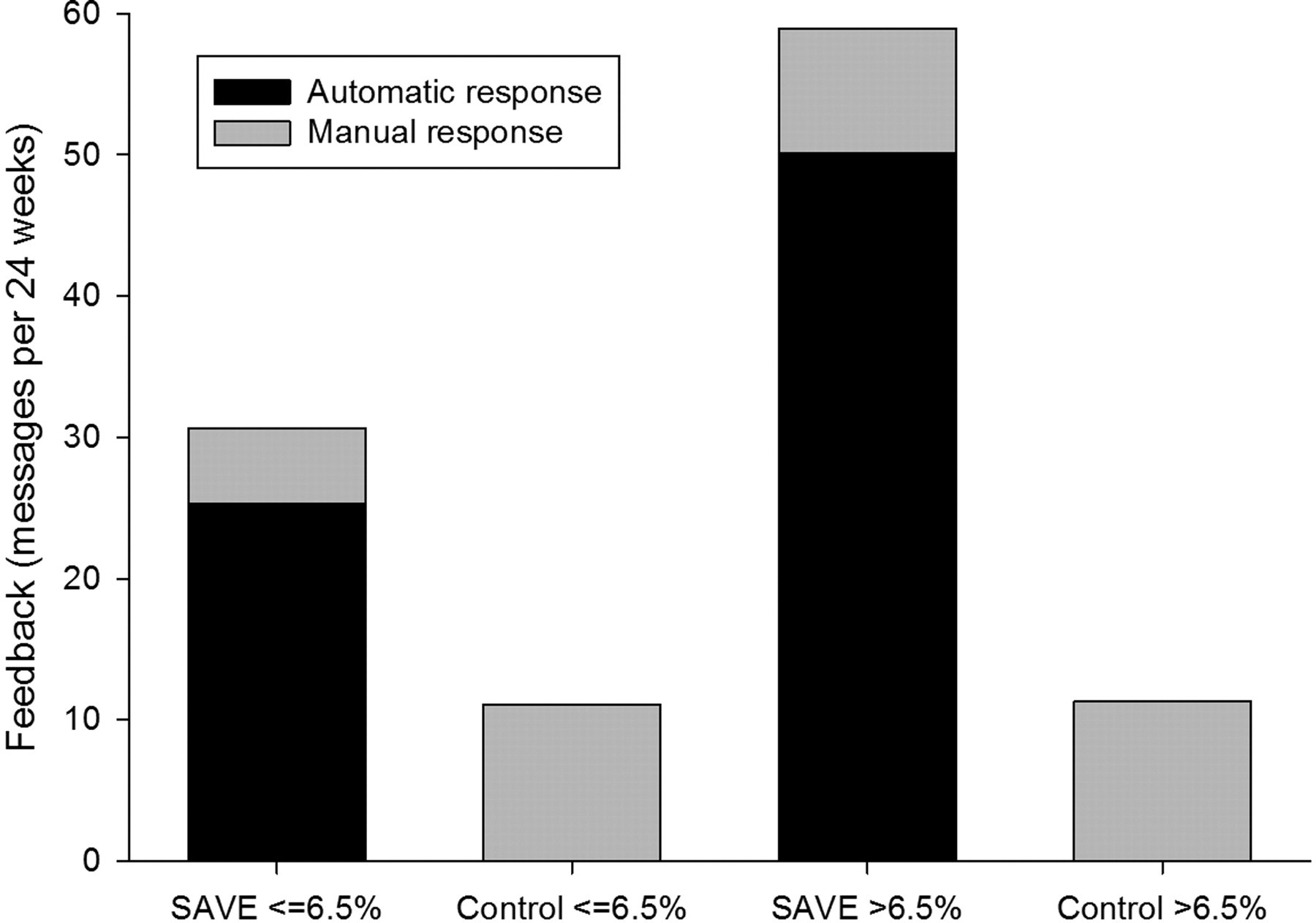
Frequency of feedback
Physicians' time
Physicians visited the online system at a frequency of 5.5 times per patient with a baseline HbA1c ≤6.5% in the SAVE group, which was significantly lower than that in the control group (12.2 times per patient on average, P < 0.01). For patients with a baseline HbA1c >6.5% in the SAVE group, the physicians logged in to the online system at an average frequency of 9.7 times per patient, which was higher than that of the baseline HbA1c ≤6.5% (P < 0.01). Physicians logged in to the online system at an average frequency of 13.6 times per patient with a baseline HbA1c >6.5% in the control group (Figure 3). Therefore, the frequency of physicians' online visiting was decreased by 55% when HbA1c was less than 6.5%. Also, the frequency was decreased by 29% when HbA1c was greater than 6.5%.
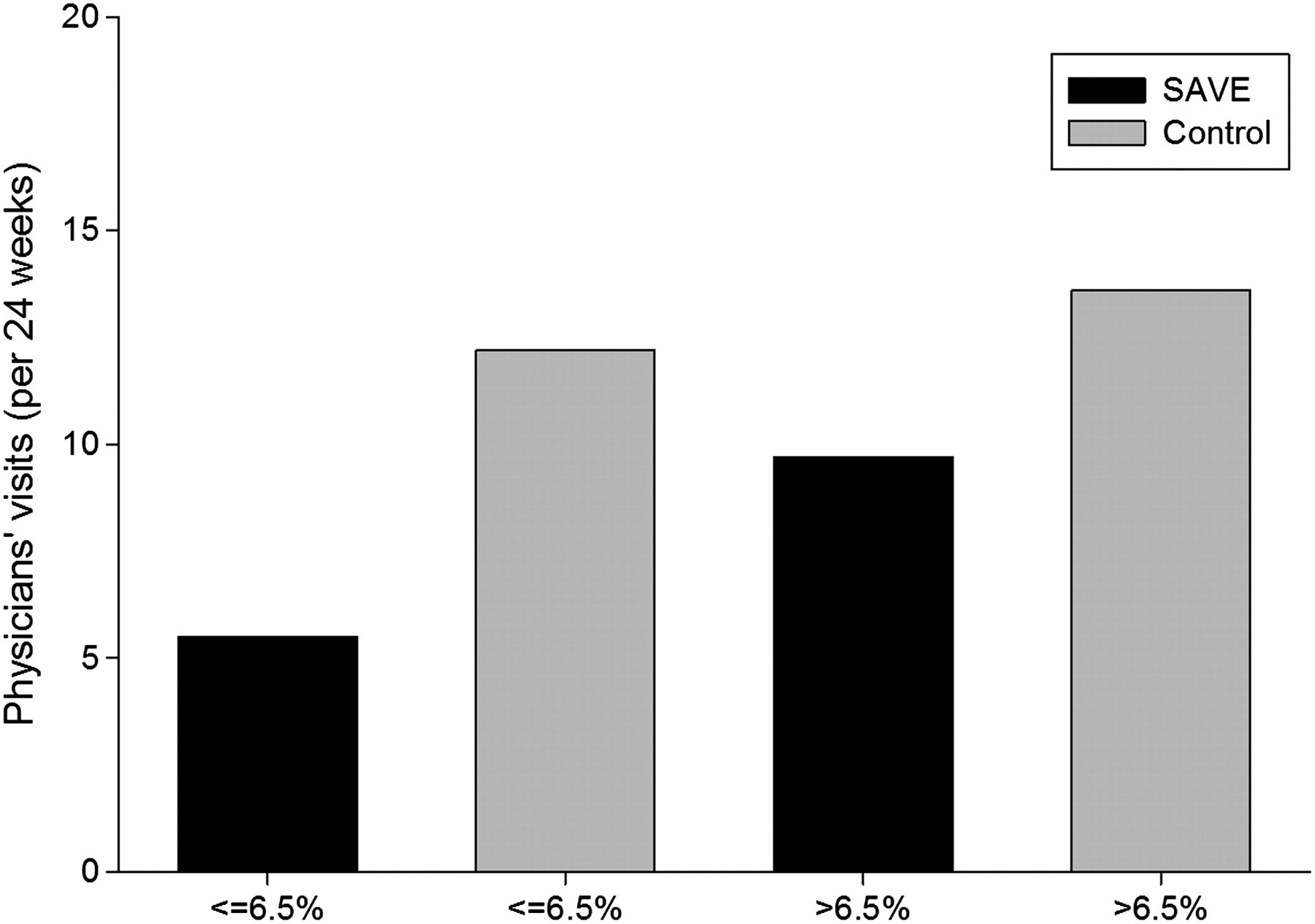
Frequency of physicians' visit time
Physicians' log-in time to review SMBG data and send recommendations was reduced by 67% and 55% in patients with HbA1c <6.5% and >6.5%, respectively.
Discussion
In our previous study, we reported the short-term and long-term effects on glucose control of our IBGM system. 5,8 To expand such systems to the general population, we needed information about labour costs, because the labour cost of physicians is a major limitation in clinical practice. We found no definitive data to estimate labour cost for maintaining such an online management system. The present study is the first to provide evidence about the labour cost and the application of such online management systems to the general population. We developed new algorithm-based glucose analysis software and examined its efficacy and safety in a randomized controlled trial. The system can reduce physicians' labour time significantly compared with manually operated systems, and our findings suggest that such software could improve the cost-effectiveness of the management system without reducing therapeutic quality. We believe that such a system will be crucial for developing other kinds of online management systems and extending their use in the general population.
The SAVE software filtered the patients with good glucose control and reported only those whose glucose levels were not within the normal range. The system reduced both frequency and duration of physicians' log-in time. These data show that the system can reduce labour costs by more than half. However, the time spent per log-in was about 20–30 s in the study, which was relatively short. This might be because participants were those with diabetes lasting more than one year who had used the website more than six months before enrolment and the log-in times included only time from reviewing SMBG data to sending messages. Thus we need to consider additional time for reviewing the personal information of patients or answering questions. If patients were newly diagnosed or they used the online communication system for the first time, the log-in time would be higher and the SAVE software would show a larger labour saving effect.
In the present study, subjects with a baseline HbA1c ≤6.5% had a similar SMBG frequency in both groups. In contrast, patients with a baseline HbA1c >6.5% in the SAVE group reported their SMBG more frequently than those in the control group. This means that subjects with good glucose control status used the system more diligently. Such diligence could help reduce HbA1c level to within the target range and maintain it there. We expected that frequent feedback to patients to remind them to check their SMBG will increase the frequency of SMBG measurement.
In summary, the algorithm-based glucose analysis software that we have trialled can reduce physicians' labour time and improve the cost-effectiveness of online communication for diabetes management. Online communication between patients and the medical team can be expected to be increasingly important in the future. Our study did not examine safety matters, such as hypoglycaemia in the two groups. But we have shown that SAVE is effective and safe as an online communication system, and the study provides evidence for extending the online communication system to the general population. In future, more advanced software will be needed to help medical staff manage diabetes patients more cost effectively, and their efficacy and safety need to be demonstrated in further clinical trials.
Footnotes
Acknowledgements
We thank Kyung-Hwa Song for collecting and inputting all the data and Jung-Ah Oh for coordinating the study. We also appreciate Young-Hwan Pack's technical assistance in developing the software. The work was supported by a Seoul R&D project grant and the Ministry for Health, Welfare and Family Affairs (A080872).