
Abstract
We investigated the factors that affected the use of a realtime telemetry system (RTS) in emergency ambulances. During the study, a total of 7144 patients were transported to a hospital in the city of Wonju via ambulance. In 466 of these cases (7%), the Emergency Medical Technician (EMT) used the RTS. Based on the Elaboration Likelihood Model, we extracted variables from the run records, such as the qualifications of the EMT, level of the patient's consciousness and the transport time. The results indicated that EMTs with higher levels of expertise were more likely to use the RTS when the level of patient consciousness was low, regardless of transport time. Conversely, EMTs with low levels of expertise were more likely to use the RTS when the transport time from scene to hospital was long and were less likely to use the RTS when the transport time was short. There appear to be several ways of improving RTS usage in the pre-hospital situation.
Introduction
Online medical direction (OLMD) in the Emergency Medical Service (EMS) system can provide an Emergency Medical Technician (EMT) with medical direction for pre-hospital patient care. 1 Use of telemetry systems can be important during patient transport via ambulance and at the scene of incidents. It helps the EMT obtain medical direction for treatment and ambulance diversion and also provides the EMT with objective information about the patients. 2 However EMTs often do not use such systems to monitor vital signs during patient transport. For example, measurement of patient vital signs by the EMT occurs less than 10% of the time in South Korea. 3,4
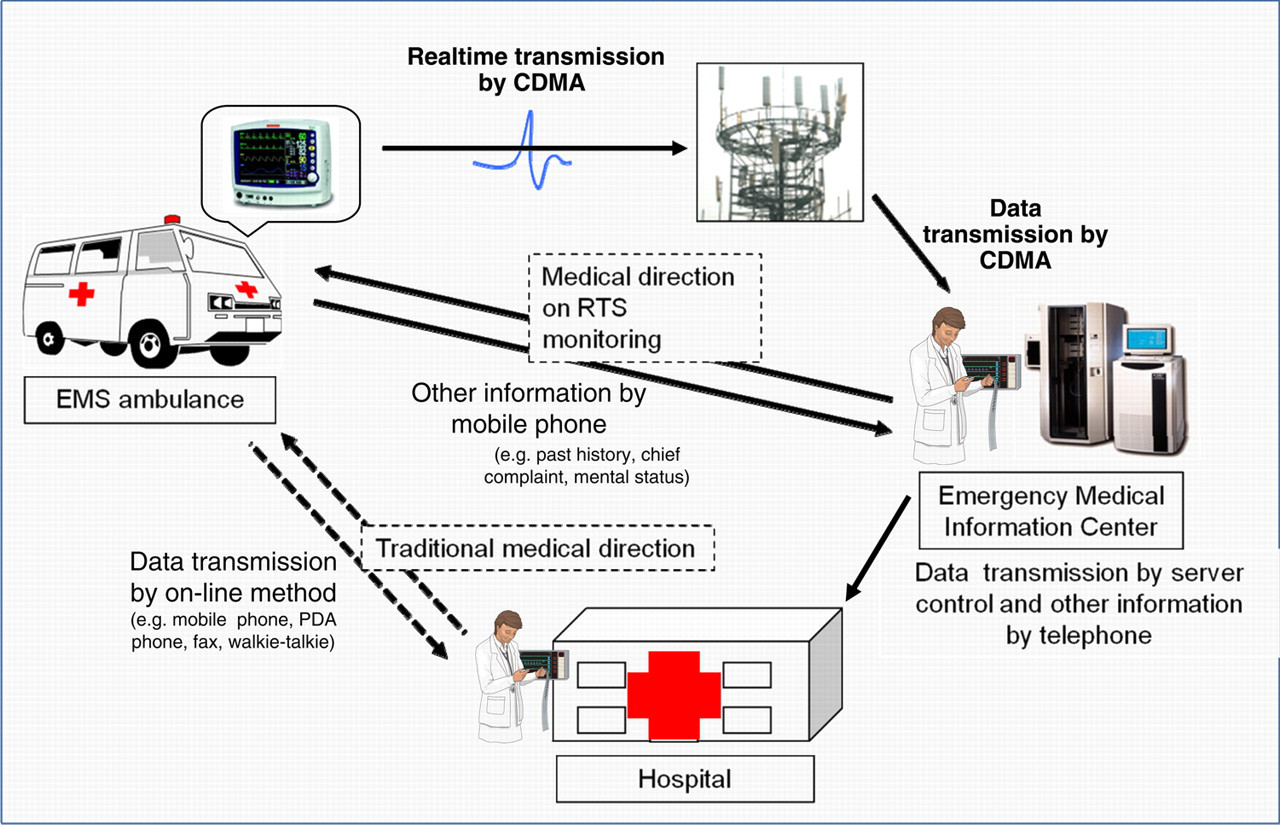
There are three levels of EMTs in South Korea: EMT level-I, EMT-level II and EMT-Basic. Generally, most pre-hospital care and transportation is performed by level II or Basic EMTs at most rural areas in South Korea. The number of people certified as EMT-level I is very low in most rural EMS regions and it is very difficult for EMTs, other than EMT-level Is, to make an accurate assessment of a patient's condition. To overcome these limitations and increase the quality of treatment provided by EMTs, appropriate and effective medical directions by a telemetry system are important. 5,6 In Wonju, a realtime telemetry system (RTS) has been a part of the EMS for three years (Figure 1). 2 However, EMTs have not taken advantage of the RTS in pre-hospital situations.
The RTS flow
Real-time telemetry system
After the arrival of an EMS ambulance, the EMT attaches the RTS monitoring system to the patient. The patient's information, including vital signs, is transmitted via a mobile phone network (CDMA) to the emergency medical information center (EMIC) and to one of three emergency medical centres with monitors in the emergency room (ER). At the EMIC, the patient data, which includes ECG, blood pressure, respiration rate, oxygen saturation and body temperature, is stored and analysed. After evaluating the information from the ambulance, a medical director at the EMIC gives medical direction directly to the EMT in the ambulance and transmits the patient's information to the ER doctor at the hospital where the patient will be transported (Figure 1).
Acceptance of technology
The users' acceptance of information technology (IT) continues to be a constant theme inside and outside of the health-care domain. 7,8 IT acceptance includes IT usage intention and actual usage behaviour. Most studies in the health-care domain focus only on patient-related factors, such as health and treatment outcomes, and neglect social factors. 8
An EMT's activities in RTS usage are often influenced by a variety of information in a pre-hospital situation, including external sources other than telemedicine systems. However, we have not found a study that examines the interaction effect of such telemedicine systems in this context. The social influence imparted by the interaction effect with information has been explained by the Elaboration Likelihood Model (ELM) of social psychology. The ELM posits that the amount of thoughtful information processing of the receiver tends to influence the recipient's reactions on types of information. 9 In the IT research domain, evidence is mixed regarding the role of ELM on IT acceptance in the workplace. 10,11
Elaboration Likelihood Model
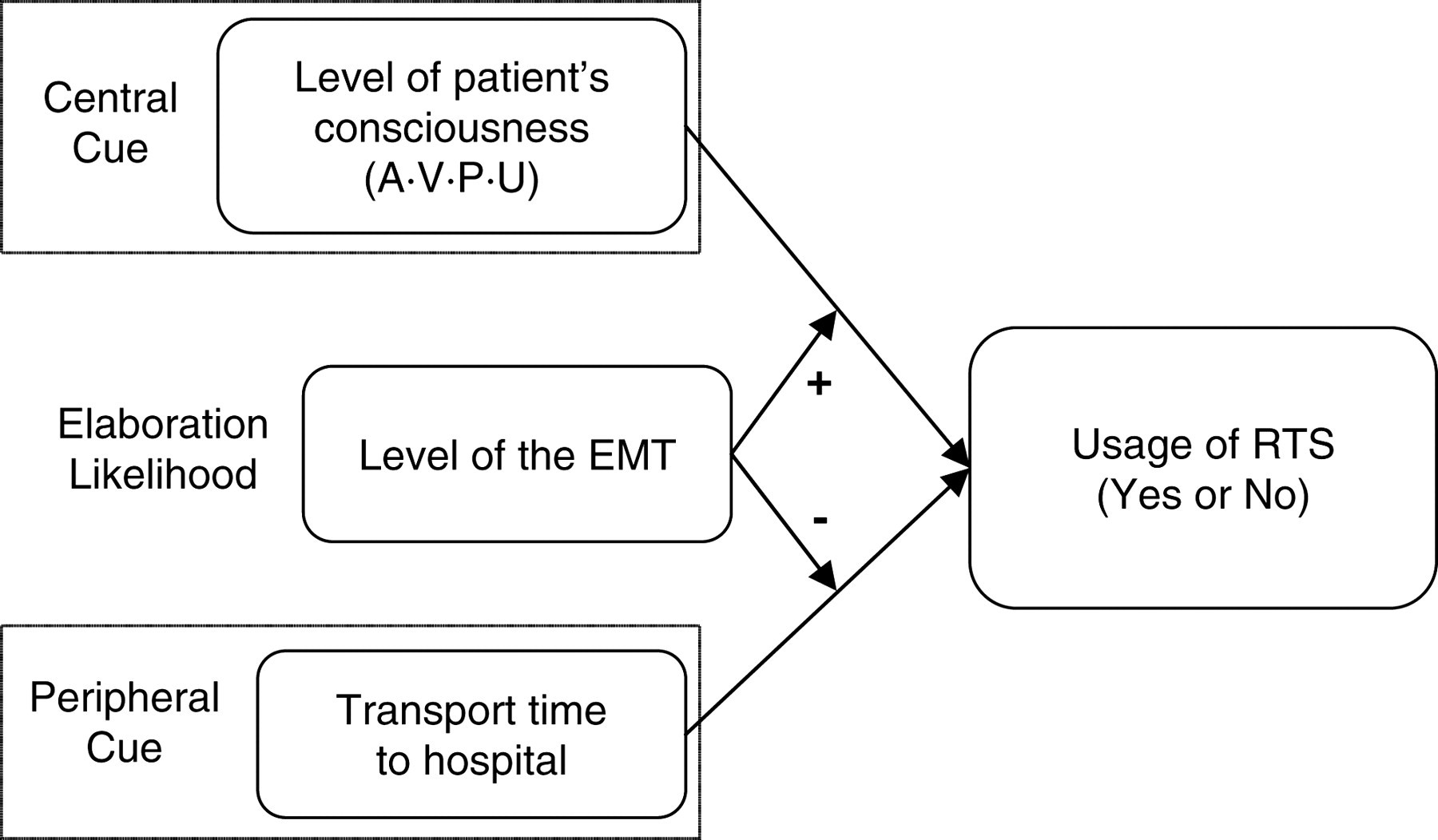
The ELM applied to IT acceptance posits that a change of attitude related to IT acceptance may be caused by two ‘cues’ of information, the central cue and the peripheral cue, which differ in the amount of thoughtful information processing or ‘elaboration’ demanded of people. 12,13 The central cue in pre-hospital situations is the level of patient's consciousness. The peripheral cue in pre-hospital situations includes other elements surrounding the central cues (e.g. transport time, transport distance, hospital preference of patient's guardian, guardian's requirement). Elaboration represents the extent to which relevant knowledge is needed to carefully evaluate information related to issues. These factors such as the EMT's expertise or education level determine elaboration. Which cue is taken is determined by the extent of elaboration. 12,13 If EMTs are able to accurately assess the patient's condition, they are considered to have high elaboration. The EMT will choose the central cue, patient consciousness and use the RTS to determine contents of the pre-hospital treatment. If EMTs lack the ability to accurately assess the patient's condition (low elaboration), they will choose the peripheral cue.
Thus, applying the ELM theoretical framework to pre-hospital situations in Wonju, we assumed that the lack of RTS use by EMTs may be the result of an interaction between the EMT's individual characteristics and various external factors. Based on this assumption, we investigated the factors that affect RTS usage, and how interaction effects between these factors affects RTS usage.
Methods
We retrospectively collected patient data using six ambulances which had been fitted with the RTS. During the period January 2008 to December 2009, the EMT recorded whether they used the RTS during patient transport. A total of 21,576 patients were transported by the six ambulances in the city of Wonju. Of these, 7144 patients who were classified as emergency by an EMT in run records were included in this observational study. These patients were divided into two: the usage group used RTS monitoring and the non-usage group did not use RTS monitoring. This information was collected at the Wonju EMIC and EMS ambulance centres in Wonju. During June 2007, EMTs were educated on the RTS and the importance of medical direction prior to its use. The education continued periodically after June 2007. In total, 46 EMTs were educated: seven of level EMT-I, 32 of EMT-II and seven of EMT-Basic. For this study, the use of patient clinical data in run records was approved by the Ministry of Health and Welfare. Ethics approval was not required.
We selected the following factors for study: the level of patient consciousness (central cue), the transport time to a hospital (peripheral cue), the usage of RTS and the level of the EMT (elaboration). RTS acceptance was assessed by analysing usage data obtained from run records, not from self-reported usage. The research questions were:
What type of information does an EMT interact with as a decision rule for the usage or non-usage of RTS? How different is the association between the level of patient consciousness and RTS usage among EMT levels? How different is the association between the transport time to the hospital and RTS usage among EMT levels?
Based on the data collected, we investigated the interaction effect between the level of patient consciousness and the level of the EMT and between the transport time to the hospital and the level of the EMT on RTS usage.
Statistical analysis
The data were analysed using a standard package (SPSS 17.0 for Windows, SPSS, Chicago, IL, USA). A Chi-square test was used to compare usage group (the group using the RTS) and non-usage group (the group not using the RTS), and variable order data was compared using one-way ANOVA. The level of the EMT (Basic (1) - Level I (3)), the level of patient consciousness (A: Alert(1), V: Verbal response(2), P: Pain response(3), U: Unresponsiveness(4)), and the transport time to the hospital (0–5 min (1), 6–20 min (2), 11–20 min (3), 21–30 min (4), 31–40 min (5)) were all on an ordinal scale, while the usage (1) and non-usage (0) of RTS was measured by a nominal scale. Based on the ELM (Figure 2), we built interaction terms between two factors that is, the level of patient consciousness × the level of the EMT (4 × 3), and the transport time × the level of the EMT (5 × 3). We utilized all of these interaction terms and the dependent variable (RTS usage) as variables for logistic regression analysis. First, we verified the goodness-of-fit for the ELM-based model (Figure 2) using logistic regression analysis. Second, we validated the effect of two interaction terms on RTS usage after ensuring the significance of the model.
Research model based on the Elaboration Likelihood Model
Results
A total of 7144 patients were transported to a hospital via ambulance, and of these, 466 (7%) had EMTs that used the RTS. Eighty patients (17%) received medical control and there were 10 (2%) ambulance diversions. The average age of the patients who were transferred was 53 years. There was no significant difference in age and sex between the usage group and the non-usage group. However, the RTS usage rate in patients with lower levels of consciousness was lower than that in patients with a high level of consciousness. There was also a significant difference in RTS usage by the level of the EMT. Furthermore, the usage group took more time to arrive at the hospital than the non-usage group (Table 1). There was also no significant difference in treatment time between the usage and non-usage groups. This means that treatment time and the time to connect patients to the RTS at the scene did not influence transport time.
Baseline characteristics
To determine whether the model adequately described the observed data, we assessed the goodness-of-fit. 14 The Hosmer and Lemeshow χ2 was 1.31 (P = 0.988) and the model coefficient χ2 was 404.7 (P = 0.001). R2, which is a measure of the model's success in predicting the dependent factor from the independent factor, was also assessed. 15,16 Cox and Snell, and Nagelkerke's R2 were 5.5% and 14.4%, respectively (Table 2). Hence, the model did indeed describe the observed data (Figure 2).
Test of the overall model
We then analysed the interaction between the level of the EMT and the level of patient consciousness. The results suggested that there was an interaction effect between these factors. The higher the EMT level, the more the central cues, such as the level of patient consciousness, affected RTS usage. Specifically, the higher the level of the EMT, the more they interacted with patients presenting with a low level of consciousness (Figure 3).
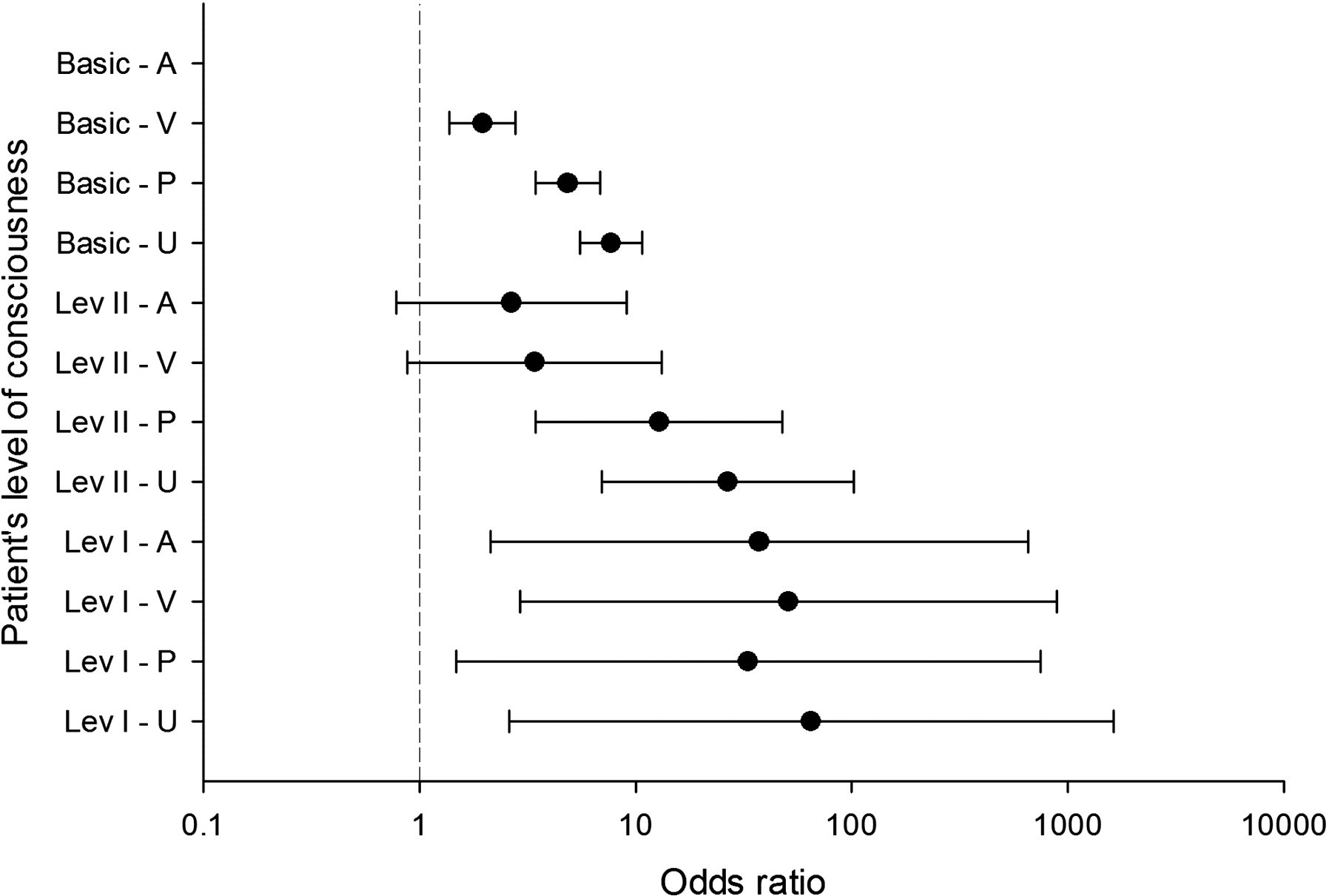
The odds ratios for RTS usage and the interaction term (the level of patient consciousness x the level of the EMT)
Next, we categorized the transport time from the scene to the hospital to determine the interaction effect between the level of the EMT and the transport time to hospital (Figure 4). The time increment was reduced to 10 min based on the longest and shortest time required for transport. Since there were only 173 (2%) cases that required more than 40 min, we excluded transport times of more than 50 min. Because of the number of cases in the 10-min range, we divided them into two groups: 0–5 and 6–10 min. There were 1896 (27%) cases with transport times under five min and 2024 cases (28%) requiring 6–10 min. These two groups accounted for 3920 (55%) of the total number of patients who were transported while the RTS was being used. The interaction effect was verified for each category.
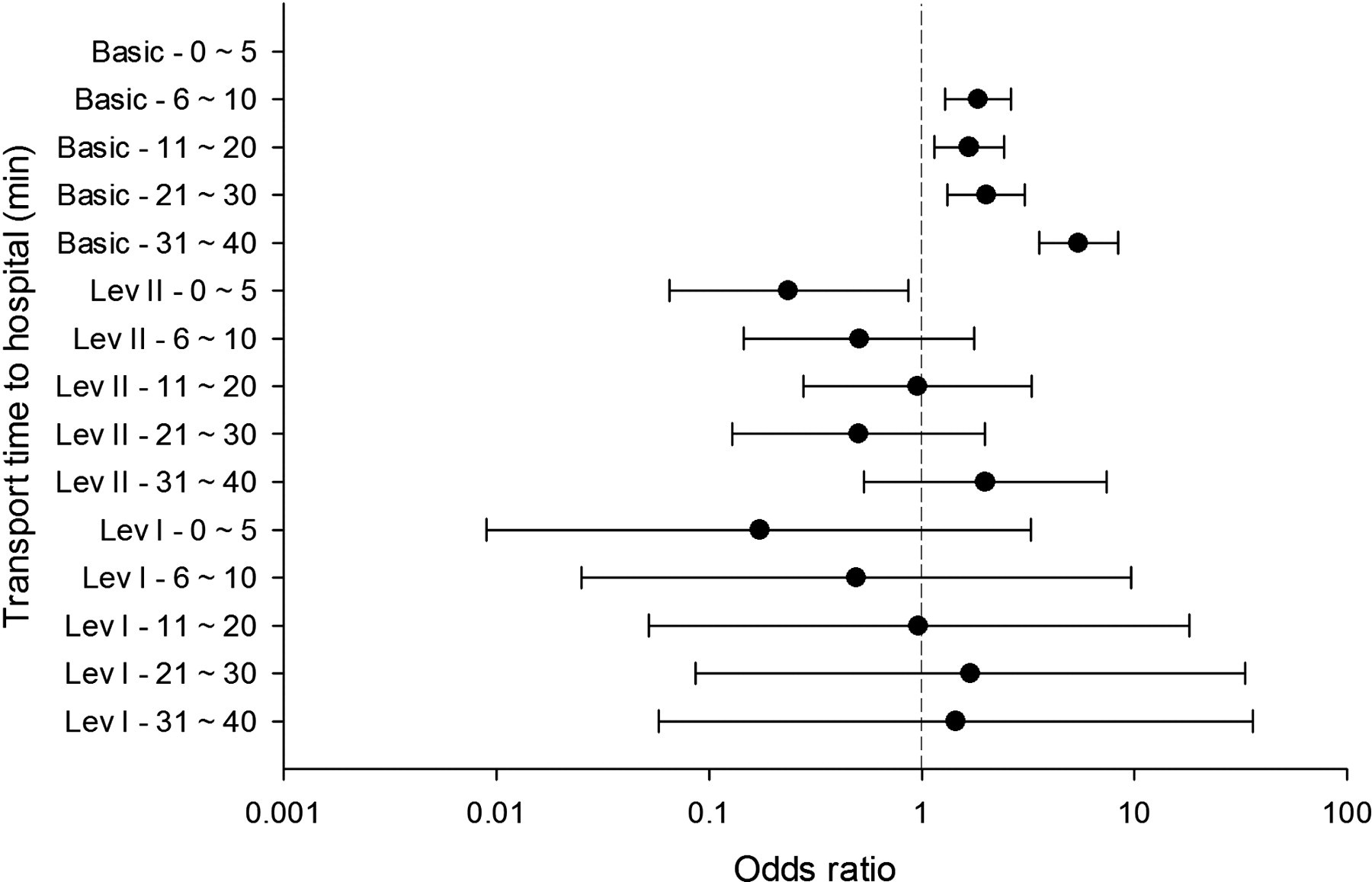
The odds of RTS usage and the interaction term (transport time x the level of the EMT)
In summary, there was an interaction effect between the factors. The lower the level of the EMT, the more peripheral cues, such as the transport time to the hospital, affected RTS usage. Specifically, higher level EMTs interacted less with peripheral cues (Figure 4).
Discussion
Advanced life support during pre-hospital care decreases mortality and morbidity. 17 At the scene or during transportation, the EMT can give more professional and accurate advanced life support with a doctor's medical direction using a telemedicine system. The utilization of a telemedicine system by the EMT is affected by the level of patient consciousness. EMTs tend to use a telemedicine system more when the patient's level of consciousness decreases. However, in Wonju, when the transport time to the hospital is short and the patient's level of consciousness is low, the reality is that simple emergency treatment is given to the patient by transporting the patient to the closest hospital. More often than not, the RTS is not used to evaluate the severity of the patient's condition or to obtain correct medical guidance, thus, adequate pre-hospital emergency treatment is not provided. We believe that this phenomenon is the result of social factors that arise from various sources, 18 because the EMT interacts with a variety of information prior to making an informed decision regarding the appropriate mode of action in a pre-hospital situation. Thus, we aimed to address three research questions based on the ELM of social psychology to help provide insight into this phenomenon: (1) What type of information does the EMT interact with, (2) How different is the association between the level of patient consciousness and RTS usage, compared to the level of the EMT? (3) How different is the association between the transport time to hospital and RTS usage, compared to the level of the EMT?
The results show that (1) the higher the level of the EMT, the more they interact with central cues, such as the level of patient consciousness. An EMT with advanced training does not interact with peripheral cues, such as the transport time to hospital, whereas an EMT with basic training interacts mostly with peripheral cues; (2) the higher the level of the EMT, the more central cues affect RTS usage. In particular, the higher the level of the EMT, the more they interact with patients with a low level of consciousness (Figure 3); and (3) the lower the level of the EMT, the more the peripheral cues affect RTS usage (Figure 4). These results are supported by previous studies of IT acceptance outside the health-care field, which found that the higher the level of the user's expertise, the more the central cues affect performance factors (e.g. IT usage intention or IT adoption). Moreover, the higher the level of the user's expertise, the less the peripheral cues affect performance factors. On the other hand, the lower the level of the user's expertise, the less the central cues affect performance factors. Furthermore, the lower the level of a user's expertise, the more the peripheral cues affect performance factors. 10,11
Based on these findings, we can suggest several ways of improving RTS usage in the pre-hospital situation. An EMT's standard judgement regarding RTS usage varies depending on the level of the EMT. Therefore, we need to modify management methods at different levels. First, medical directors at the EMIC (Figure 1) should focus on providing the EMT-Basic with educational services, such as an RTS usage manual. Second, the number of higher level EMTs who are deployed in pre-hospital situations should be increased. Also, a standard protocol for pre-hospital RTS use should be established and enforced, regardless of the level of the EMT.
The present study identified the interaction factors that affect RTS use by employing a theoretical framework (ELM). Most previous studies have measured IT usage intention and predictors using a self-report method. 19,20 However, our study employed direct testing with actual IT usage data obtained. As a result, we can conclude that our results strongly support the results of previous studies of IT acceptance. The results of the present study can be used to increase RTS acceptance amongst health-care providers in pre-hospital situations.
Limitations and future work
A limitation of the present study was the use of a limited set of potential variables. There are other variables that affect IT usage or acceptance. 18 In fact, practitioners and sponsors (e.g. medical directors, the Ministry of Health and Welfare) adopting and supporting telemetry systems such as the RTS seem to have not understood the reason for users to not accept telemetry systems in South Korea. The focus on training for adopting telemetry system reflects this. However, work in emergency medicine is complicated by multiple health-care providers interacting across organizational boundaries. Thus IT is needed that supports, enhances, fits with and does not disrupt emergency care processes. Therefore future studies need to investigate the effect of factors of four distinct types (technological, individual, organizational and social) and interaction among them to predict implementation success. 18 Finally we used the run record that had been recorded by EMTs, although the record may be inaccurate. However our study is the first which studied the factors affecting the usage of a telemetry system for medical direction in the pre-hospital situation.