
Abstract
We reviewed our experience with the Tanzanian Telemedicine Network in supporting paediatric care at 40 small, rural hospitals in the country. The network began operating in 2008. Store and forward telemedicine was provided via the open source software iPath. The 33 volunteer consultants were based in several countries, although most of them had practical experience in Tanzania. During the first three years of network operation there were 533 referrals. There were 159 paediatric cases (median age five years). Three paediatric specialists provided most consultations (64%), but other specialists provided recommendations when required. The response time was usually less than two days (median 6 h; inter-quartile range 2–24 h). A precise recommendation was not always provided, but since all consultants had an intimate knowledge of the state of health services in Tanzania, their advice was usually well adapted to the local circumstances of the hospitals. Referral to a higher level of care was recommended in 26 cases (16%). A simple web-based telemedicine system combined with email alerts is feasible in remote locations in Tanzania, even where fast Internet connections are not available.
Introduction
Telemedicine may be a useful alternative approach for delivering health care and education in resource-constrained settings. 1–6 The Evangelical Lutheran Church in Tanzania (ELCT) is a non-governmental health-care provider and contributes about 20% of all Tanzanian health facilities, covering about 20% of the population. The ELCT owns one university hospital, 22 mostly rural hospitals, one mental hospital, eight health centres and 145 dispensaries. As in the rest of the country, the rural hospitals lack specialists (for example only three paediatricians) and sufficient numbers of health staff. 7,8 Because of the limited health service provision, the health department of the ELCT started a telemedicine network in 2008 to serve its own and other remote hospitals and health institutions in the country. 7
Telemedicine network
The aim of the telemedicine network was to provide rapid clinical problem-solving in all specialities and continuous medical education for health staff in remote locations throughout the country. 7 The network used the iPath web-based system, originally developed at the University of Basel, which is available as open source software. It provides a simple store-and-forward telemedicine system, which can be used in low bandwidth settings. 6,9,10 The intention was to offer the service to all health institutions, not only those of the ELCT. Therefore, a collaboration with governmental activities in this sector was established. 7
Simple digital cameras (costing about € 250 each) were provided to the 14 hospitals which expressed interest in participation. Only those hospitals that had access to the Internet were included. Computers and digital cameras are not essential to the use of the iPath system, as it can also be used with smartphones which have a built-in camera. The initial funding for the project (€ 100,000) came from the Dutch non-governmental organisation CORDAID and the International Institute for Communication and Development (IICD). The use of the iPath server was free, but fees for Internet access had to be met by the hospitals themselves. A typical telemedicine case could be managed for a cost of less than € 0.1.
A workshop was held to train 14 key users from the hospitals. Subsequently, on-site technical training was conducted at the participating health institutions at least once-per-year. Other hospitals were invited to join the network and were offered the same training and digital cameras as the first 14 hospitals.
Health staff at the rural hospitals submitted the patients' clinical information and where appropriate digital images of X-ray films, ultrasound, ECG, CT scans or clinical photographs to the website (
The consultants accessed the individual cases as requested by the iPath system and wrote their recommendation into a standard reply box. The replies were then available to the requesting physicians/health staff and to other consultants who could provide their opinion as well. Final responsibility for treatment remained with the staff at the rural health institutions.
In principle, consultants could provide continuous medical education to the staff at the participating institutions, using the same system. 7,11 However, this feature has yet to be used due to lack of consultant capacity. Nonetheless, the telemedicine network provides an opportunity for consultants and health institutions in industrialised countries to consolidate their knowledge and expertise in diseases which are almost non-existent in their home countries. 12 Thus the telemedicine system facilitates reciprocal learning and exchange.
We have reviewed the use of the network in the first 36 months with regard to paediatric consultations.
Methods
We performed a retrospective analysis of all case data files which were stored on the iPath system. We collected the following data for paediatric patients (i.e. those aged under 18 years): age, sex, reason for consultation, speciality of consultant, consultant's country of residence, time to first response by consultant and patient's outcome. Non-paediatric cases were excluded.
During their regular visits to the participating hospitals, the ELCT telemedicine team conducted unstructured, informal interviews with staff about progress and problems with the system.
Results
During the first three years, the network expanded from 14 to 40 referring institutions. Between March 2008 and February 2011, about 250 physicians and non-physician health workers were trained in the use of the telemedicine system. A total of 33 volunteer consultants from outside the rural hospitals participated in the network. They came from the following discipline: paediatrics, obstetrics and gynaecology, surgery, anaesthesiology, radiology, dermatology, internal medicine, infectious diseases or ophthalmology. They were based in Tanzania, Britain, Germany, Switzerland, Finland, Norway, US, India, Australia and New Zealand.
During the three years of the review, a total of 533 telemedicine cases were submitted. Of these, 159 were related to paediatric patients (median age five years; 48% female). They were submitted from 35 hospitals (Figure 1). Among the ten hospitals with the highest number of consultations, only two had attended the initial workshop, and the remaining staff had been trained during the site visits. Most consultations were related to common paediatric problems like infectious diseases or neonatal disorders. Less than 20% of all consultations concerned rare diseases like congenital syndromes.
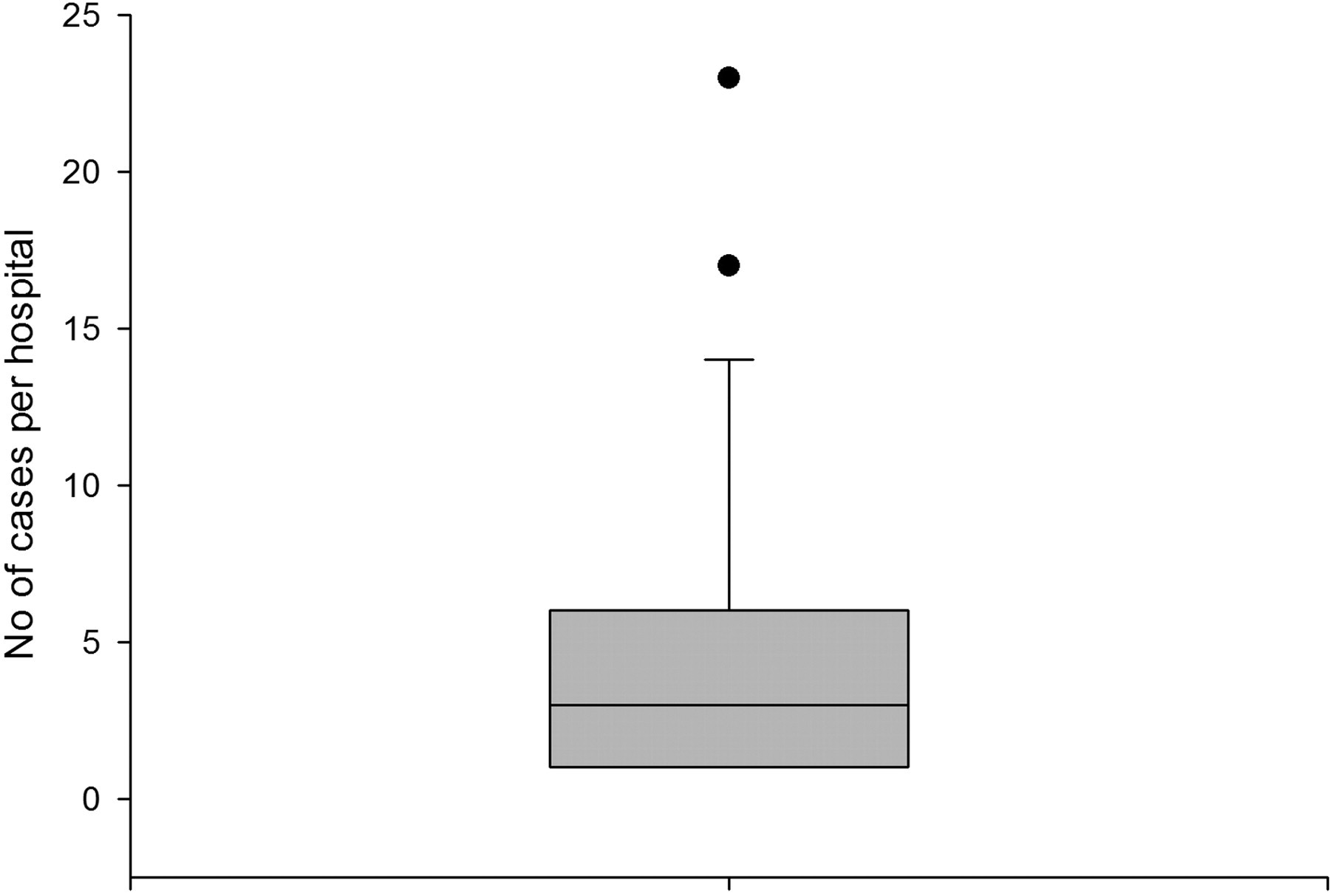
Numbers of paediatric referrals from the participating hospitals. The box defines the 25th and 75th percentiles, with a line at the median, and the error bars define the 10th and 90th percentiles
Three experienced paediatricians (one in Germany, one in Tanzania and one in the US) provided recommendations in 101 cases (64%) (Figure 2). In the other 58 cases (36%) the recommendations were provided by two obstetricians, four physicians, four dermatologists, three radiologists, one ophthalmologist, one anaesthesiologist and five surgeons. Only in two cases did consultants not respond to a new consultation. The response time was usually less than two days (median response time 6 h; inter-quartile range 2–24 h) as many of the cases required urgent recommendations (Figure 2). 51% of the consultations were answered within the first six hours, and 76% within 24 hours.

Time between paediatric referral and first response from a consultant
A precise recommendation was not always provided, sometimes because of lack of a detailed case history or missing investigations. However, since all consultants had an intimate knowledge of the state of health services in Tanzania, their advice was usually well adapted to the local circumstances of the hospitals. Referral to a higher level of care was recommended in 26 cases (16%).
Feedback on the final outcome was rarely provided. Only in 20 consultations (13%) was feedback provided by the rural hospital staff. Ten patients died and ten recovered. Thus the accuracy of the initial consultant diagnosis could only be assessed in a minority of cases. No information was available about whether the consultations improved the clinical management skills of the referring doctors.
The problems encountered by the health staff in the remote health institutions were computer illiteracy, insufficient training in utilisation, uploading of data and figures and reporting skills and sometimes inaccessibility of the Internet due to interrupted connectivity, leading to reduced utilisation of the network. Therefore, a manual referral form was created for those who were not computer-literate. This form could be given to another person at the hospital, such as an administrator, who could upload the consultation request on behalf of the referrer.
Discussion
One important feature of the Tanzanian Telemedicine Network is that it was developed in a developing country and not from outside like in many other projects, thus facilitating a sense of ownership and empowerment in the rural hospital and in the ECLT health department. 1,3,12 The final responsibility for the treatment remains with the staff at the health institutions, and the consultants only provide their recommendations and ideas. Even hospitals in areas with slow access to the Internet can submit referrals. 5,6,7,13 Thus the participating remote health institutions are not dependent on fast connections and can still benefit from specialist recommendations.
Apart from the technical feasibility and low cost, the telemedicine system allows rapid reply and management of clinical cases. Most consultations concerned common diseases like infections or neonatal disorders, which allowed the consultants to explain the typical diagnostic and therapeutic approach in these conditions along with their case-specific recommendations. The short response time, which was similar to other reports, 2 has been very encouraging. The automatic email alerts and reminders by the administrator were essential in achieving this. In many cases, urgent decisions had to be made concerning the management of the patients.
The informal interviews with the staff at the health institutions revealed that the network supported staff motivation as well. People felt that they were not working in isolation and that their work was valued by the medical community. Another important aspect was the cheap and fast service to patients, compared with having to travel to referral hospitals. The cost of sending patients to referral hospitals has been estimated to be 10–100 times higher than using telemedicine, due to the travelling and accommodation costs and missed income during the time of absence from home. 7
The main challenge has been to change the attitude of the health staff at the remote health facilities. The utilisation rate is too low compared to the number of paediatric patients who are seen each day. Other authors have estimated that only 0.1% of possible consultations in the developing world are dealt with by telemedicine. 1 This is probably due to the high workload so that the health workers do not have time, are not motivated to use the teleconsultation service or fear technical difficulties.
Assessing the accuracy of the consultants' recommendations and confirming the correct diagnosis are rarely possible in telemedicine systems, especially as feedback on outcomes is available too infrequently. 12,14 Furthermore, we do not know yet whether the quality of paediatric services has improved at the participating institutions. This would be an important task for the future evaluation of the telemedicine network. Another challenge is the long-term financial sustainability of the network, as charges apply for Internet access, for using the server and for maintenance of the hardware. A formal cost-effectiveness analysis has been commissioned.
The legal aspects of telemedicine have not been settled in Tanzania. 12,15,16 There is no national regulation concerning the limits and responsibilities of those asking for and providing expert advice. This problem exists in many other telemedicine projects and needs to be addressed seriously in the future. 16 Furthermore, ethical issues like technical standards, allocation of scarce financial resources, informed patient consent, confidentiality, quality of medical advice and provision of care need to be discussed. 12,15,16 Is it justifiable to use financial resources for a telemedicine system whose technical capabilities (e.g. quality of images) may not be acceptable? Would it be better to spend these resources on actual patient care? Do patients really understand the implication of their confidential data being transferred to another health-care provider? How is the quality of advice controlled? Does the system improve service delivery? These matters need to be addressed in future work.
Conclusion
The present review has shown that a simple store-and-forward, Internet-based telemedicine system combined with email alerts is feasible in remote locations in Tanzania, even where fast Internet connections are not available. The Tanzanian Telemedicine Network provides a tool for non-specialists in remote health institutions to discuss difficult paediatric cases (and others) with experts and thus to improve their clinical management and their knowledge.
Footnotes
Acknowledgements
We thank the donors, participating health institutions and the volunteer consultants of the Tanzania Telemedicine Network for their support. Funding was provided by CORDAID and the IICD.