
Abstract
In one-to-one telephone coaching, the patient receives regular telephone calls from a health professional. We have reviewed the evidence for one-to-one telephone coaching. Following a literature search we retrieved 41 articles which reported on the development and the efficacy of 34 separate telephone coaching interventions for LTC management. Telephone coaching for LTC management has only occurred in the last ten years, is becoming increasingly prevalent, and is dominated by interventions in North America and Europe. Twenty-seven (79%) of the studies reported on randomised designs involving at least one control or comparison group/condition. Of the 34 interventions reviewed, 17 (50%) were aimed at diabetes management and 17 (50%) were designed to manage chronic cardiovascular conditions. Most studies (32 or 94%) reported outcomes in favour of the telephone coaching intervention, although few (15%) employed any form of cost-benefit analysis (CBA). In order to obtain a better impression of overall service efficacy, more clearly defined service outcomes are required in future.
Introduction
A Long Term Condition (LTC) is one that cannot be cured, but can be controlled by medication and other therapies. One form of telemedicine, which has been used to support people with LTCs, is one-to-one telephone coaching. 1 This means that the patient receives regular telephone calls from a health professional. The purpose of the calls is to provide support and encouragement to the patient with the aim of promoting healthy behaviours, such as medication control, healthy diet, physical activity/mobility, rehabilitation and good mental health. The expectation is that the patient will then maintain their own health more independently and that the professional (and patient) will be in a position to identify potential problems before they become critical. 2
In the UK, some telephone coaching services have been in operation for several years (e.g. Birmingham Own Health 3 ), while others are in an early stage of development. We have reviewed the evidence for one-to-one telephone coaching.
Methods
Cochrane review guidelines encourage the use of rigorous quantitative designs. 4 However, in situations where reviews cover a broad range of comparisons and limited evidence is available, a more narrative approach is recommended. In the present review, considerable variation in the type of the evidence available was expected. Therefore, we followed a descriptive, semi-quantitative review protocol. 5
Sources
The following methods were used to locate relevant published studies. First, electronic searches of the following databases were carried out: MEDLINE, PsycINFO and Web of Science. Second, citations in articles identified by the electronic searches were also examined. Third, hand searches of the following journals were conducted: International Journal of Telemedicine and Applications, Journal of Telemedicine and Telecare, Telemedicine and e-Health. Where existing relevant review articles were identified, these were also hand searched.
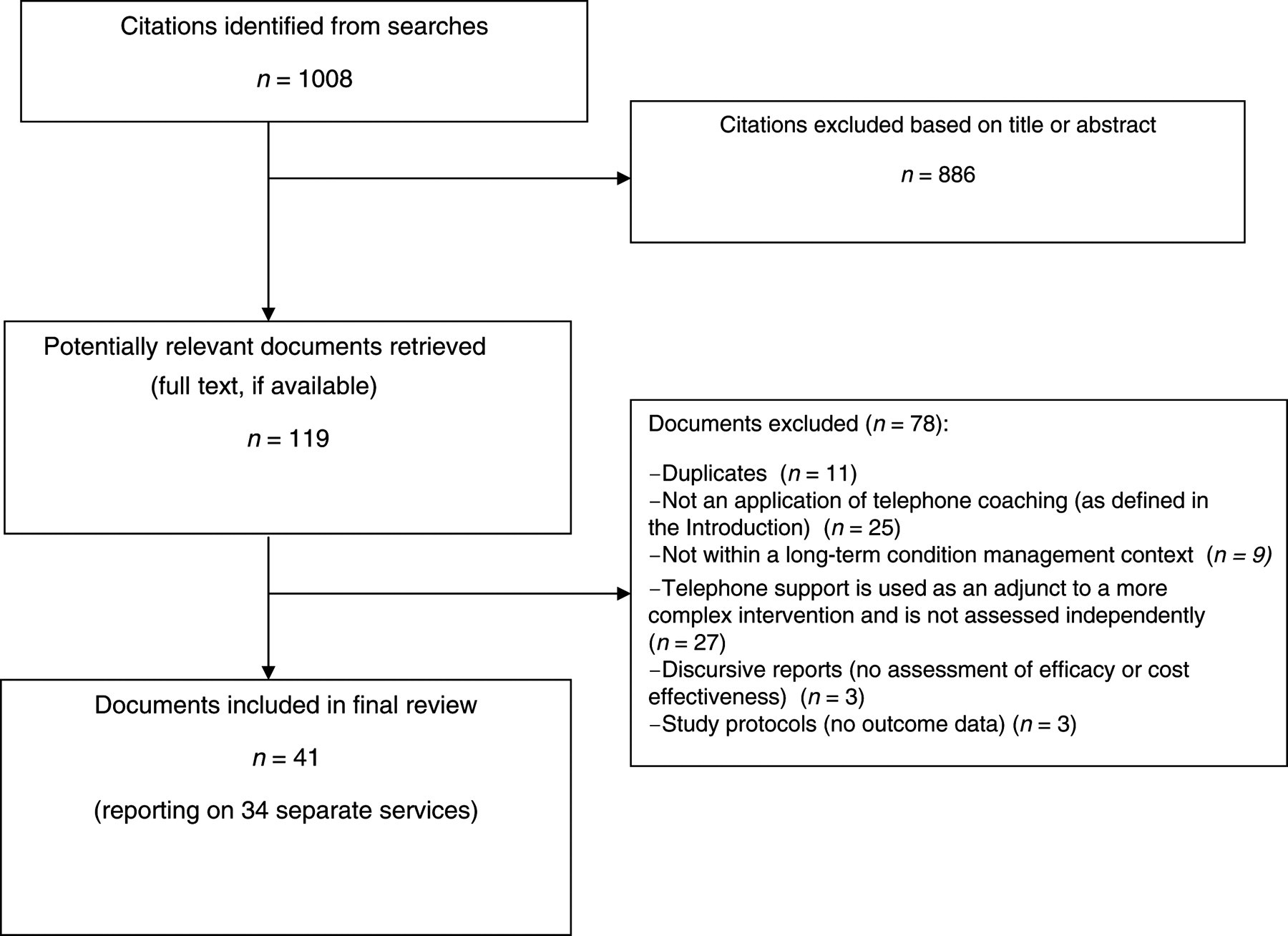
The following keywords were used for electronic database searches: [TELEMEDICINE], [TELEPHONE COACHING], [TELECOACHING], [TELEHEALTH], [TELEPHONE SUPPORT] with either [LONG TERM CONDITIONS] or [CHRONIC ILLNESS]. The study selection process and the filtering process are summarised in Figure 1. The inclusion criteria were:
English language articles; Randomised Control Trials (RCTs), preliminary reports, pilot investigations; reports of the use of telephone coaching as a method of supporting people with LTCs; reports on the efficacy and/or cost effectiveness of telephone coaching; literature available up to September 2010.
Study selection process
Procedure
Hard copies of relevant publications were obtained. Each intervention was allocated an ID number (see Table 1). Where randomised experimental designs were included, the Jadad scale 6 and Delphi list 7 were used to assess the quality of the trials.
Summary of the evidence
Results
The characteristics of the included studies are summarised in Table 2. The outcome data are listed in Table 3. The percentage figures in Tables 2 and 3 demonstrate the proportion of the total number of studies, which demonstrate specific characteristics or report specific outcomes. In some of the categories identified, studies demonstrate multiple characteristics and/or outcomes. Therefore, the combined percentage figures in each section will not always total 100% as they are relative to the total number of studies, not each other.
Sample characteristics
aIndicates that the sample in this instance were not patients with LTCs but the carers of those patients
Outcome data
aIndicates a significant (P < 0.05) beneficial effect in favour of the telephone coaching intervention for the outcome variable in question, e.g. an improvement in mental health/health related quality of life or a reduction in hospital readmissions
bIndicates that, for evidence where a comparison condition (e.g. face to face support) is included instead of a control group, the telephone support described is beneficial (P < 0.05) and also similar to the alternative condition
cIndicates that a beneficial effect is reported but due to the qualitative or descriptive nature of the data, the effect is not quantifiable
Overview
The review process resulted in 41 articles being retrieved, which reported on the development and the efficacy of 34 separate telephone coaching interventions for LTC management. Although searches were not restricted by date or country, telephone coaching for LTC management has only occurred in the last ten years, is becoming increasingly prevalent and is dominated by interventions in North America (predominantly the USA) and Europe (these accounted for over 80% of the available evidence). Twenty-seven (79%) of the studies reported on randomised designs involving at least one control or comparison group/condition. Seven (21%) represented pilot studies and six (18%) were non-randomised prospective cohort designs. Sample sizes ranged from less than 20 to cohorts of up to 750 participants.
Summary characteristics
Of the 34 interventions reviewed, 17 (50%) were aimed at diabetes management and 17 (50%) were designed to manage chronic cardiovascular conditions. Some of the interventions were designed to address multiple conditions, such as respiratory conditions (e.g. COPD), cancer, arthritis, depression and Parkinson's disease. Some variation was observed in the exact nature of the different telephone coaching services reviewed. Specifically, 19 (56%) described stand-alone telephone coaching based support, whereby patients are telephoned and given verbal advice by a health professional or trained coach. Other studies reported the use of videophones (24%), SMS (9%) and automated voice messages (9%) as methods of delivering telephone advice. The review evidence also revealed that advice delivered to patients was often based on information received using remote telemonitoring procedures (e.g. remote monitoring of blood glucose levels). Fourteen (41%) of the interventions involved remote telemonitoring. Consequently, the evidence for stand-alone telephone support is considerably less than when remote telemonitoring and alternative advice delivery methods are taken into account. For LTC management, medically trained coaches (e.g. nurse practitioners) usually delivered the intervention material/advice to the patients (65%). However, in situations where the advice is consistently structured (i.e. generic information) or delivered not in person (e.g. via SMS), specially trained interventionists were also employed (34%). The frequency of the support provided ranged from more than one call (or SMS text) per week (15%) to one every four to six weeks (9%). It was also not uncommon for the frequency to decrease as the intervention progressed (in 32% of studies), in order to encourage patient independence and self-management. Sixteen (47%) of the studies identified an intervention framework or an underpinning theory, which dictated the content or nature of the telephone advice. These included protocols outlined by the American Diabetes Association (12% of total studies) and specific models of counselling practice (3%).
Quality of randomised designs
Most studies provided a description of an appropriate randomisation process (e.g. use of a table of random numbers, computer-generated). Six of the 27 interventions reported as employing randomised designs did not describe the randomisation process. One described an inappropriate method of randomisation (patients were allocated alternately to intervention or control group). None of the reviewed studies reported a process of blinding participants, interventionists or outcome assessors to the group allocation. All of the studies described eligibility criteria and details of drop-outs or participants lost to follow-up.
Outcomes
A range of different outcomes were reported, see Table 3. These included physical (50%) and mental health (38%) markers, health related quality of life (29%), self-reported health perceptions (29%), patient's utilisation of health-care services (27%) and self-care regimen compliance (34%). Some interventions also conducted a process evaluation to examine patient satisfaction with the telephone coaching service (27%).
Only five (15%) of the reviewed interventions demonstrated any assessment of cost-effectiveness or cost benefits. The methods used to establish this information also varied considerably. Two of the five studies reported differences in costs associated with hospital readmission charges; one study reported cost savings associated with a reduction in caregiver working hours; two studies examined the costs associated with delivering telephone coaching and those associated with hospital readmissions and then made direct comparisons between the intervention and control groups. Where some form of cost-effectiveness or cost benefit analysis was reported, 80% of these studies reported that the telephone coaching intervention resulted in a cost benefit.
Of the 34 studies reviewed, 32 (94%) reported outcomes in favour of the telephone coaching intervention. Of those, 27 (79%) reported at least one quantifiable statistically significant (P <0.05) beneficial effect in favour of the telephone coaching intervention. For stand-alone telephone coaching interventions (n = 22), 19 (86%) reported outcomes in favour of the telephone coaching intervention. Of those, 16 (73%) reported at least one quantifiable significant (P < 0.05) beneficial effect in favour of the telephone coaching intervention. The most notable benefits of telephone coaching interventions were improved self-care regimen compliance, increases in self-confidence towards disease management, improved mental health and reductions in hospital readmissions. Finally, 80% of the studies which evaluated patient satisfaction with the intervention demonstrated positive patient perceptions of the services provided.
Discussion
The aim of the present review was to draw together the evidence for one-to-one telephone coaching services, to help relevant stakeholders (e.g. service developers, commissioning bodies, service providers and practitioners) better understand the case for telephone coaching. The results demonstrate a significant rise in the implementation of telephone coaching services in the last 10 years, particularly in the US and Europe. However, there is considerable variation in the development and implementation of these services, with a number of inconsistencies in the reporting of research findings. Consequently, a more robust approach to the development, monitoring and evaluation of telephone coaching services is required to allow the overall efficacy of these approaches to be accurately determined. However, the present review can highlight a number of important implications regarding the development of future telephone coaching services.
Evaluations of telephone coaching services have mainly involved randomised experimental designs (79%) with at least one control condition (e.g. participants receiving treatment as usual rather than telephone coaching). This suggests an awareness of the need to provide high quality evidence where possible. However, previous systematic reviews of telehealth based services have questioned the methodological quality of research in this area and of RCT designs specifically 8–10 Consequently, we conducted a quality assessment of the randomised experimental designs identified in the present review. Overall, the results of this reflect favourably on the included studies, demonstrating that most studies reported appropriate methods of randomisation, clearly definable inclusion criteria and a transparent account of any loss to follow-up. Although quality assessment criteria emphasise the importance of blinding in randomised experimental designs, 6,7 due to the nature of telephone coaching, both the participants and interventionists could not be blinded from the experimental group allocation. Therefore, a lack of blinding in this instance should not be interpreted as a methodological flaw. Based on this, the methodological limitations highlighted in previous reviews may actually reflect a lack of methodological ‘consistency’ as opposed to ‘quality’.
Although telephone coaching interventions have been applied to a range of LTCs (e.g. respiratory illnesses, arthritis, Parkinson's disease and mental health problems), results appear particularly promising in diabetes management 11–13 and chronic cardiovascular conditions. 14,15 Variations are evident in the way telephone and mobile communication technology has been used to deliver coaching to patients. Services range from SMS 16 and automated voice messages 17 to videophone 18 and personal telephone support, 19 with or without remote telemonitoring. Such variations make it difficult to obtain an overall picture of effectiveness.
Considerable variation is also evident in the exact nature of the human element of these interventions, which raises concerns in regard to the fidelity and consistency of application and efficacy. For example, only 47% of the reviewed studies identified an intervention framework or underpinning theory which dictated the content or nature of the intervention. However, where an underpinning theory or framework was specified, significant findings in favour of the telephone coaching service were always reported. Results also revealed that nearly two-thirds of services were delivered by medically trained coaches, although the exact nature of that training and the assessment of competence (if applied) were rarely reported. Future studies should consider applying treatment fidelity processes 20,21 to encourage researchers to accurately implement (and fully report) the exact nature of their interventions/telephone coaching services. Treatment fidelity refers to a clearly defined set of methodological procedures, which can be used to ensure that appropriate theoretical models are applied accurately and that those delivering the services are competent at applying the theoretical concepts appropriately. Treatment fidelity therefore provides a systematic process for the design and implementation of interventions and should ensure consistent and reliable results. 22
From a financial perspective, the evidence is limited, with few (15%) of the reviewed interventions employing any form of cost-benefit analysis (CBA). This seems particularly surprising since improved efficiency is a common goal in telemedicine. Where some form of CBA was reported on, four of these services (80%) indicated financial benefits in favour of telephone coaching interventions over existing services. However, these findings should be interpreted with caution because there was considerable variation in the types of cost benefits reported and the methods used to establish them. In addition none of the reviewed studies reported an attempt to calculate Incremental Cost Effectiveness Ratios (ICERs), a technique commonly employed in heath economics to explore the cost benefits of new services or therapeutic interventions when compared to established alternative practices. 23 These findings are echoed in a previous telemedicine reviews, which have criticised economic evaluations for failing to take into account important costs, neglecting associated indirect costs and not using standard economic evaluation techniques. 24,25
While evidence demonstrating CBA in telephone coaching is limited, a range of other positive outcomes were reported. These outcomes varied across the studies reviewed, although most reported physical benefits, mental health improvements, self-reported health perceptions and self-care regimen compliance. Other services resulted in increased confidence (and self-efficacy) towards disease management and reductions in hospital readmissions (which although not reported, are likely to be associated with cost benefits). Consequently, despite the observed heterogeneity in outcome measures and study designs, the range of positive outcomes reported suggests that telephone coaching can provide an adaptable approach to LTC management, which can be tailored to suit the needs of specific services and patient groups. However, in order to obtain a better impression of overall service efficacy, more clearly defined service outcomes are required. This inconsistency in the outcomes applied across reportedly similar services makes comparison difficult and as a result the findings from the present study have to be interpreted with caution.
In conclusion, our review found an increase in the popularity of telephone coaching as a means of managing LTCs and a range of potential benefits. However, the results also highlight inconsistencies in the development and implementation of telephone coaching interventions. Those developing telephone coaching based services must recognise the need to adopt consistent and transferable frameworks, monitoring and evaluation systems and robust outcome measures. Moreover, the reliability and consistency of the intervention (including the human components) should be made more explicit, be theoretically underpinned and fully articulated. In addition, the evidence synthesis indicated a need for future studies and LTCs services, to fully report how interventions have been developed in line with their intended aims.