
Abstract
We compared the diagnostic accuracy of 3-lead tele-ECGs to both 12-lead tele-ECGs and a conventional 12-lead ECG device (the gold standard). The subjects were older people (n = 107) with a mean age of 66 years. The overall agreement between two cardiologists on interpreting the 3-lead tele-ECG recordings was 97% (kappa = 0.96, P < 0.001) and it was 91% for the 12-lead tele-ECGs (kappa = 0.90, P < 0.001). We also found excellent agreement on the interpretation of the 3-lead tele-ECGs compared to the gold standard: 98% (kappa = 0.96, P < 0.001) and for the 12-lead tele-ECG compared to the gold standard: 98% (kappa = 0.96, P < 0.001). Bland-Altman plots showed that the apparent differences between the techniques were not clinically relevant. The use of a 3-lead tele-ECG device may be useful for reducing the delay in treating specific heart disease conditions, e.g. in older people affected by chronic heart disease who need frequent ECG monitoring.
Introduction
There has been increasing use of telecardiology in the last ten years, especially in older people. This allows a pre-hospital diagnosis to be made, and also plays a role in successfully managing treatment from a distance in older patients with chronic heart disease. Home tele-monitoring, including regular telephone interaction with medical staff, has been proposed to reduce health-care costs associated with long-term care in patients with chronic heart failure. 1,2 Furthermore, early detection of transient electrocardiogram (ECG) changes is essential in patients with cardiac arrhythmias due to the poor relation between intermittent arrhythmias and symptoms. 3 The ability to identify such alterations often holds therapeutic implications in the presence of a paroxysmal atrial fibrillation Transient Ischaemic Attack (TIA) or stroke risk patients, 4 as well as in patients with a history of TIA or stroke, 5 in patients with an atrio-ventricular (AV) nodal block 6 or in those with a supraventricular tachycardia needing ablation treatment. 7 The tele-ECG has also been shown to optimize drug treatment protocols in older people with chronic heart failure. 2
The use of portable devices for recording and transmitting a 12-lead tele-ECG, 8 as well as lead-less, patient operated ECG devices, 9 has been validated in large groups of younger adults. Even though the use of the 12-lead tele-ECG in older people has shown a beneficial role in coronary heart disease, its use in older populations remains limited because of the comorbidities and disabilities which inhibit rapid and simple ECG recording. We hypothesized that use of a simpler device, such as the 3-lead tele-ECG, might have an important advantage in older comorbid patients. Since there is only limited evidence regarding the clinical value of home tele-monitoring in older people 10 and to the best of our knowledge no studies have examined the performance of a 3-lead tele-ECG device in an older population, we tested the diagnostic accuracy of a 3-lead recorder compared to both a 12-lead tele-ECG and the conventional 12-lead ECG (gold standard).
Methods
The patients were enrolled from the pre-surgical evaluation unit in the outpatient Day Surgery Service at the Italian National Research Center on Aging in Ancona during a one-month period. The patients, 57 men and 50 women, were invited to participate in the study. The study was approved by the appropriate ethics committee. Patients were included in the study independently of the presence or absence of any heart disease. Their mean age was 66 years (range 60–72).
The first step consisted of recording ECGs using the following devices:
standard 12-lead ECG (the gold standard). This was performed using a standard ECG recorder (Archimed 42–20, Esaote Biomedical, Florence Italy); 3-lead tele-ECG. This was performed using a personal ECG recorder with three wires (CG-7100, Card Guard Scientific Survival Ltd, Rehovot, Israel). Twelve phases were calculated as follows: rhythm leads and leads I, II, III, aVR, aVL, aVF, V1, V2 in the first phase, leads V3 and V4 in the second phase, and leads V5 and V6 in the third phase; 12-lead tele-ECG. This was performed using a portable 12-lead ECG recorder (CG-7000DX-BT, Card Guard Scientific Survival Ltd, Rehovot, Israel).
All recordings were performed in the hospital on the same day. The tele-ECG recordings were transmitted from outpatient examination rooms (Day Surgery Service) to the Telemedicine Call Centre of the Division of Cardiology in the same hospital using telephone transmission with specific call centre software (Heartline version 6.5.0.15, Aerotel Medical Systems, Israel).
The second step consisted of the interpretation of the ECG recordings in a blinded and independent manner by two cardiologists who were unaware of the study protocol. All ECG analyses were blinded to the result of the other ECG modality and the clinical information of the patient. Thus the cardiologists did not have the standard or tele-ECG (3 or 12 leads) of a given patient simultaneously. The heart rate and electrical axis of the ECG were calculated and an ECG diagnosis was given according to international standards. 11,12
Statistical analysis
Continuous ECG variables (e.g. heart rate, QT, PQ interval) and nominal variables (e.g. arrhythmias, bundle branch block, AV nodal block, abnormalities of repolarization) were analysed for reliability (agreement) for each investigator and total effect. The agreement between cardiologists on both the 3- and 12-lead tele-ECG trace scores and 3- and 12-lead trace versus gold standard was measured by computing weighted kappa statistics for each diagnosis. The inter-rater agreement was calculated using the kappa statistic. 13 Interpretation of the kappa statistic was as follows: kappa > 0.75 indicates excellent agreement; kappa > 0.40 and kappa < 0.75 indicates fair to good agreement; kappa <0.40, poor agreement. 14
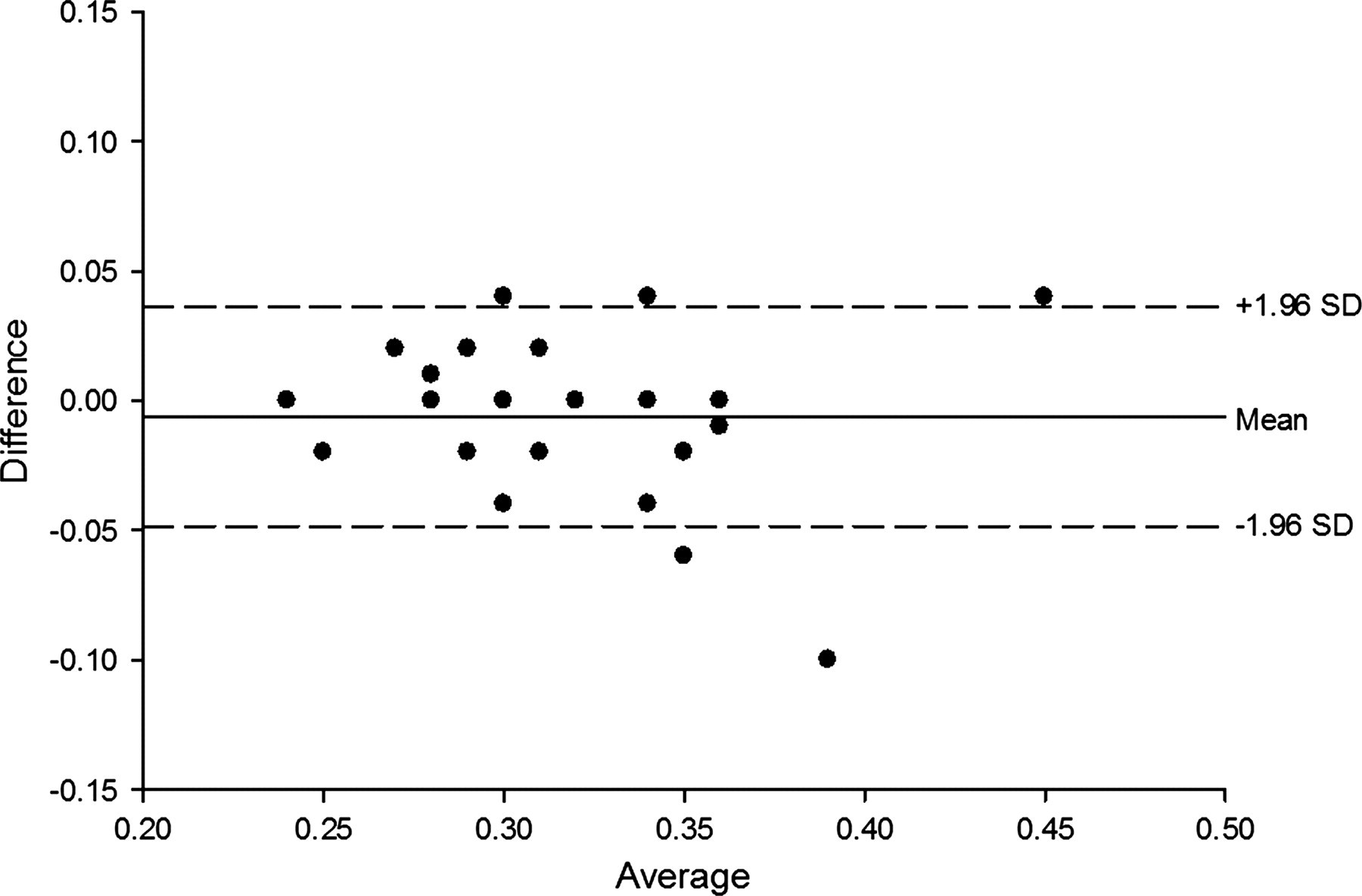
The Bland and Altman plot 15 was used to compare measurement techniques (HR, QRS interval and ST). In this graphical method, the differences between two techniques are plotted against the averages of the two techniques. Horizontal lines are drawn at the mean difference and at the mean difference plus and minus 1.96 times the SD of the differences. If the differences are not clinically important, the two methods may be used interchangeably. Data analysis was performed using a standard package (SPSS/Win version 17, SPSS Inc., Chicago, IL, USA).
Results
No technical problems occurred during the ECG recordings made using the three devices. Thus three complete ECG recordings were obtained from each patient (n = 107). According to the gold standard method, there were 50% with a normal ECG, 7% with AV nodal block, 9% with a QRS ≥ 0.12 s, 11% with ST trait deviations and/or T wave abnormalities, 1% with atrial fibrillations, 11% with right bundle branch block and 11% with left bundle branch block.
Both tele-ECG recordings correctly diagnosed sinus rhythm in 106 patients and one atrial fibrillation. Thus, rhythm analysis was 100% correct. The overall agreement between the two cardiologists on interpreting the 3-lead tele-ECG recordings was 97% (kappa = 0.96, P < 0.001) and on the 12-lead tele-ECG recordings was 91% (kappa = 0.90; P < 0.001). The kappa coefficients between cardiologists for different diagnoses from ECG recordings are shown in Table 1. There was good agreement between investigators on the interpretations drawn from both the 3- and 12-lead tele-ECGs.
Agreement (kappa values) between the observers for the ECG diagnosis in the 3-lead tele-ECG and the 12-lead tele-ECG (n = 107). All values are significant at P < 0.001
The overall agreement percentage between the two cardiologists on interpreting the 3-lead tele-ECG recordings compared to the gold standard was 98% (kappa = 0.96; P < 0.001) and for the 12-lead tele-ECG compared to the gold standard was 98% (kappa = 0.96; P < 0.001). There was also excellent agreement on the ECG diagnoses made using the 3- and 12-lead tele-ECG recordings compared to the gold standard method, see Table 2.
Agreement (kappa values) on ECG diagnoses in the tele-ECG devices compared to the gold standard method (n = 107). All kappa values were significant at P < 0.001
Finally, we investigated if heart rate (HR), and the intervals of PR, QT and QRS, as well as ST abnormalities could be adequately measured using 3- and 12-lead tele-ECGs. The Bland-Altman plots showed that the apparent differences were not clinically relevant and the statistical tests (paired t-test) confirmed that the mean differences of the measurements were zero. There was good agreement between both techniques compared to the gold standard – as well as good agreement between the 3- and 12-lead tele-ECG recordings – on heart rate, PR interval, QRS interval, QT interval and ST abnormalities. The Bland-Altman plots of the QT interval and ST abnormalities are shown in Figures 1–6.
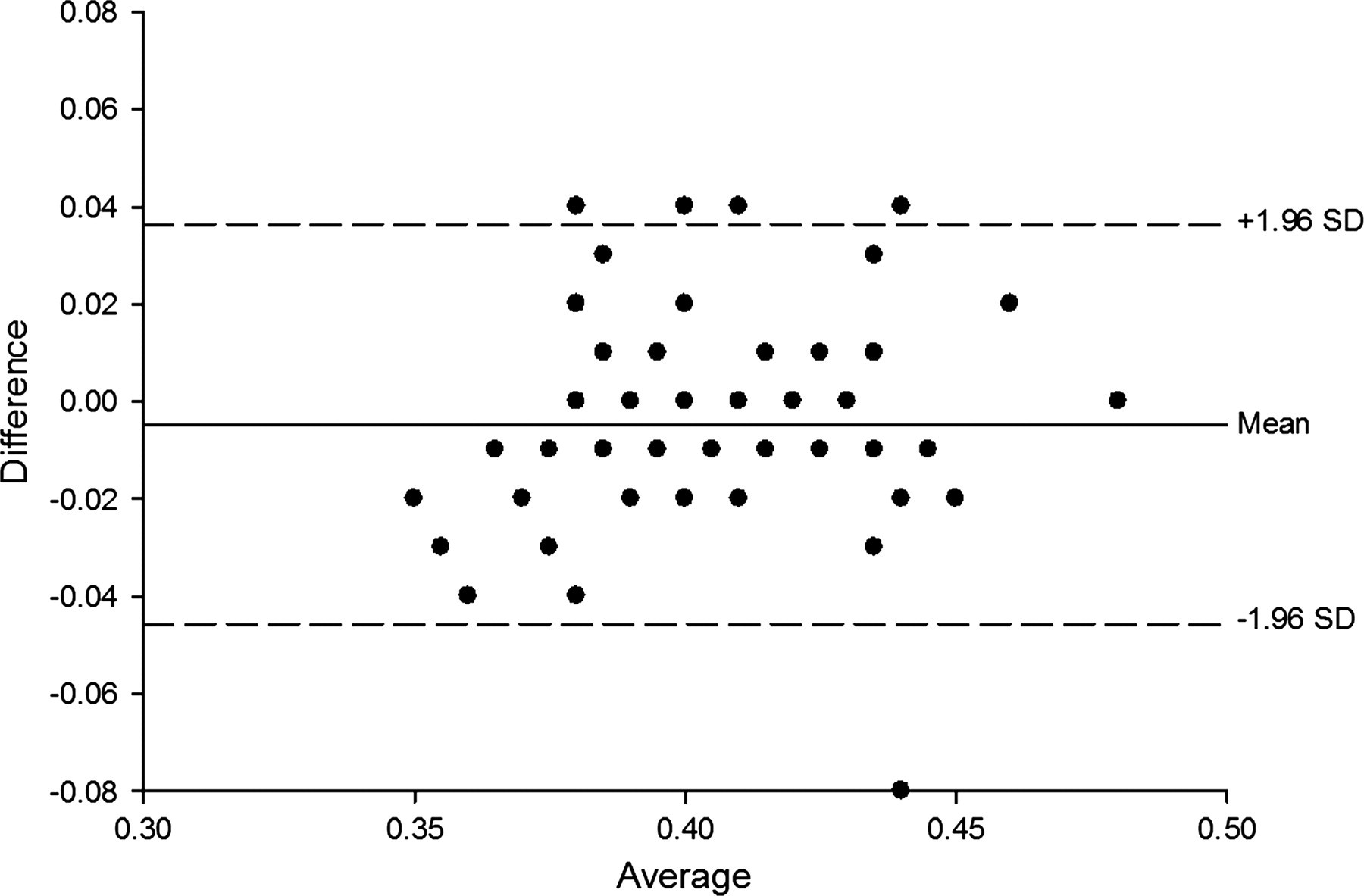
Bland and Altman plot for the QT interval. QT_GS is from the 12-lead ECG gold standard method. QT_tele-3 is from the 3-lead tele-ECG
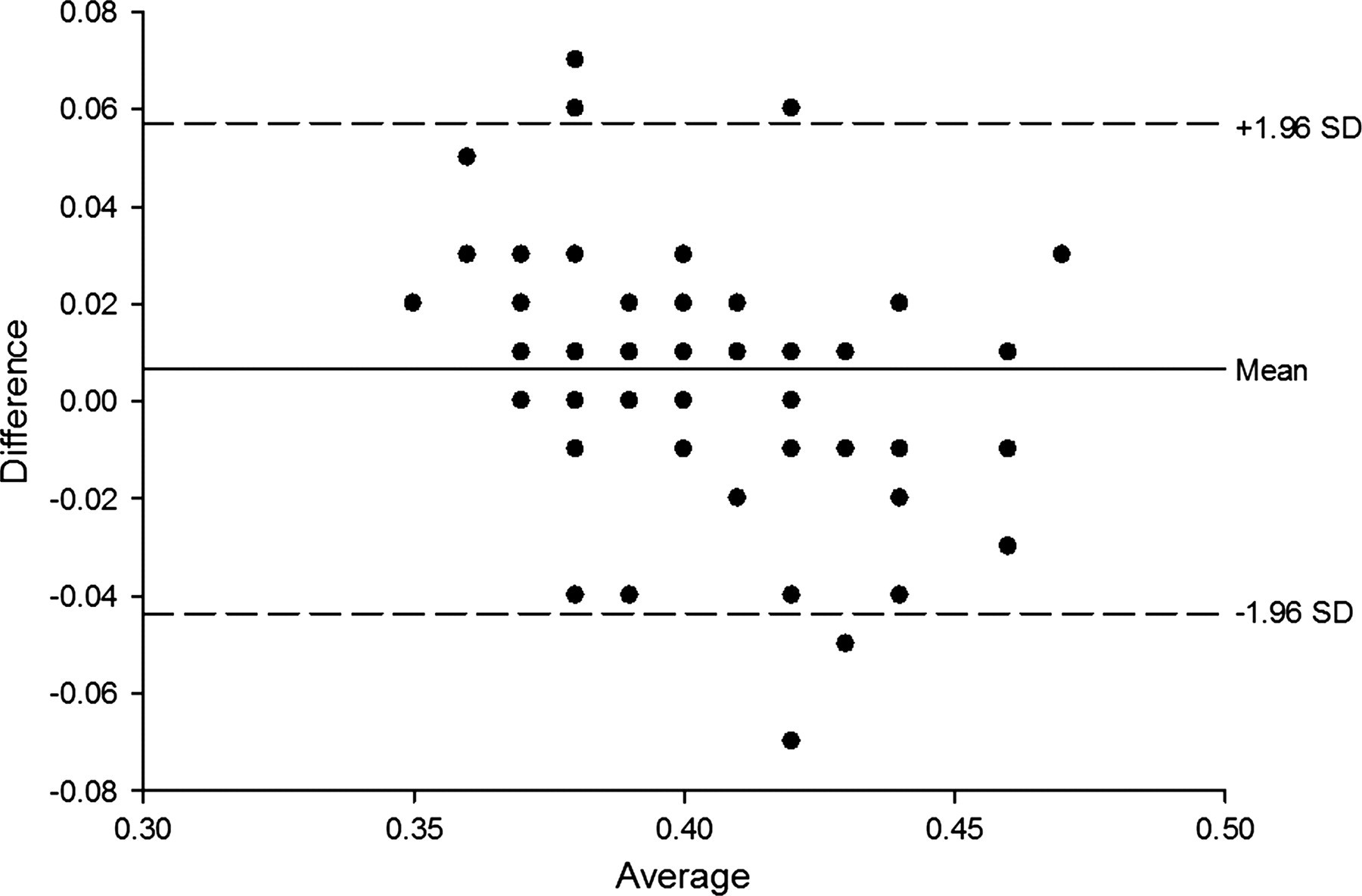
Bland and Altman plot for the QT interval. QT_GS is from the 12-lead ECG gold standard method. QT_tele-12 is from the 12-lead tele-ECG
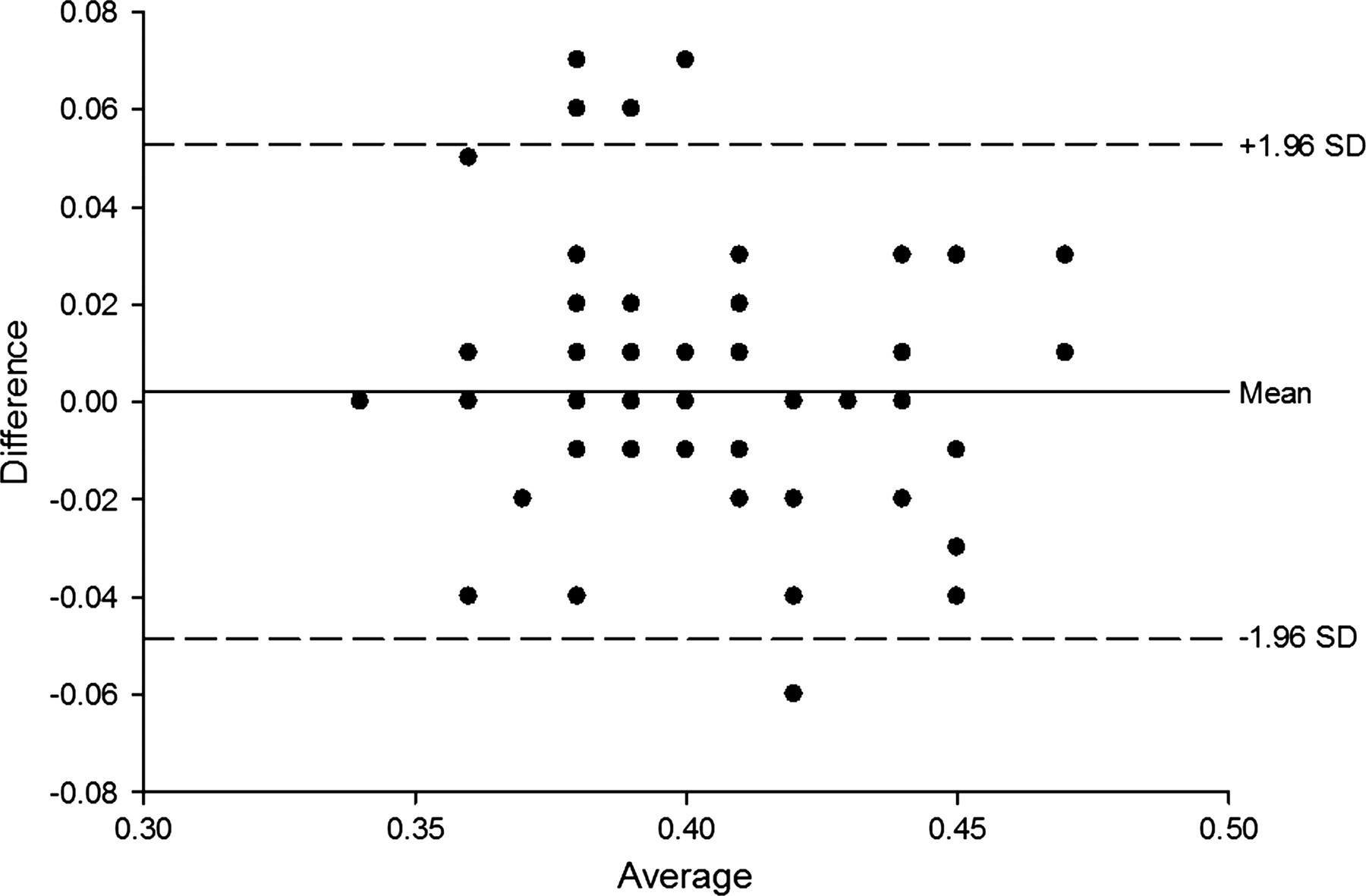
Bland and Altman plot for the QT interval. QT_tele-3 is from the 3-lead tele-ECG QT_GS is from the 12-lead ECG gold standard method
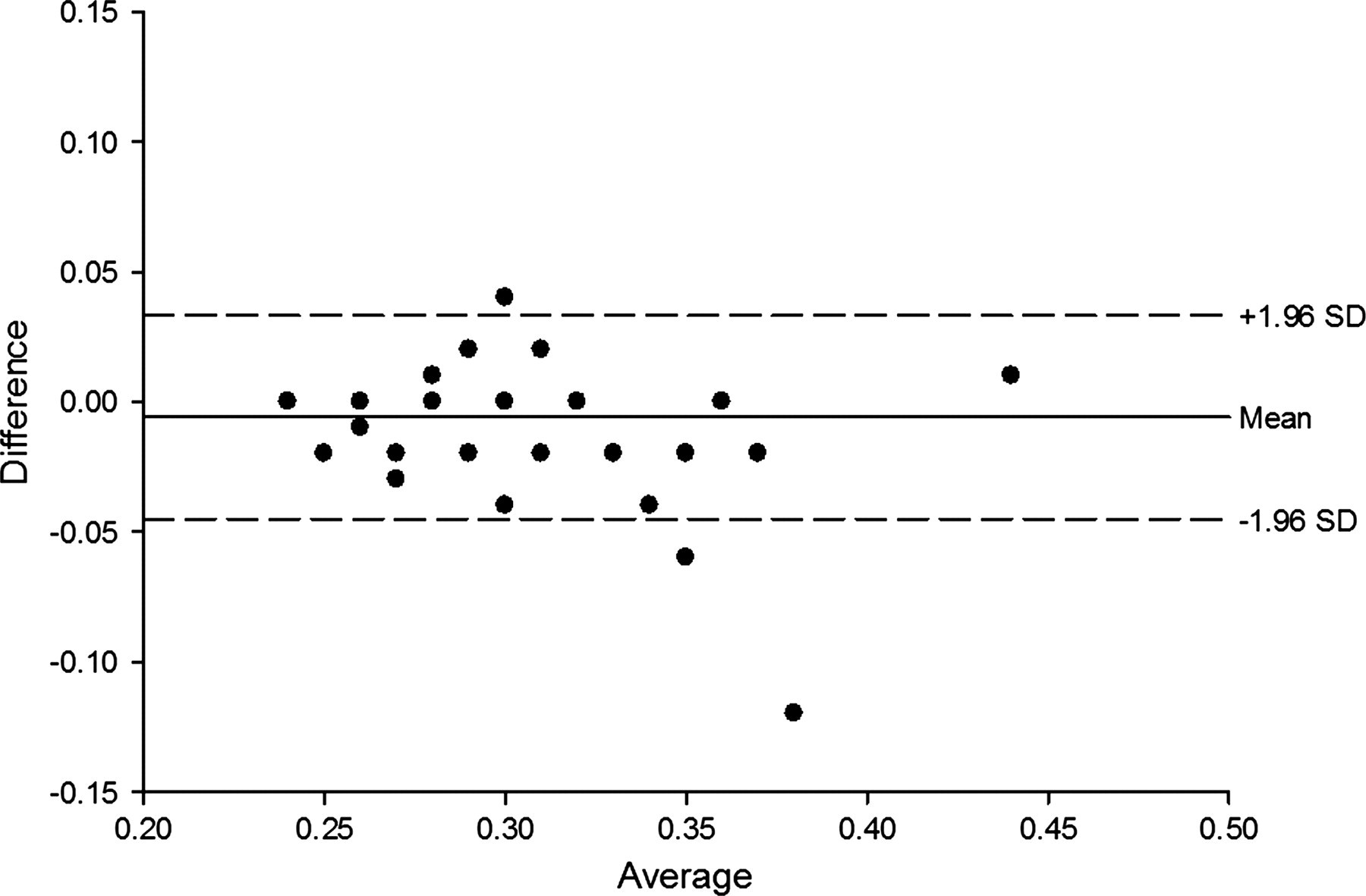
Bland and Altman plot for the ST interval. ST_GS is from the 12-lead ECG gold standard method. ST_tele-3 is from the 3-lead tele-ECG
Bland and Altman plot for the ST interval. ST_GS is from the 12-lead ECG gold standard method. ST_tele-12 is from the 12-lead tele-ECG
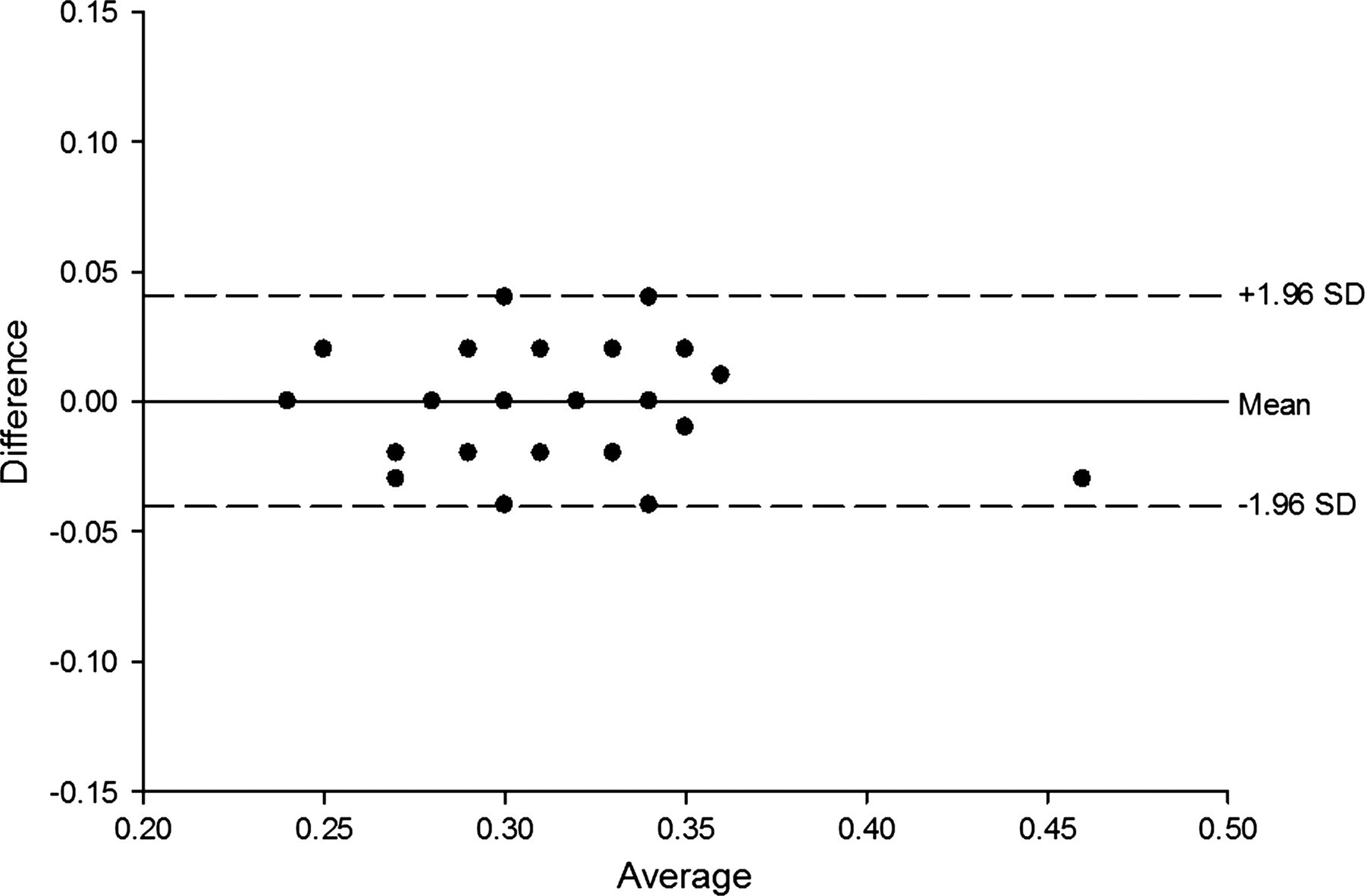
Bland and Altman plot for the ST interval. ST_tele-3 is from the 3-lead tele-ECG. ST_tele-12 is from the 12-lead tele-ECG
Discussion
The present study showed a high level of concordance between the ECG diagnosis using a simple home telecardiology device (3-lead tele-ECG) and more complex instruments like the 12-lead tele-ECG and the gold standard technique. The study also demonstrated that a simple 3-lead tele ECG can be used to detect cardiac alterations, like arrhythmias, atrio-ventricular blocks and repolarization abnormalities with good agreement compared to the 12-lead tele-ECG and the conventional gold standard technique in older people. We also found that heart rate and standard PR, QT, QRS and ST intervals using the 3-lead tele-ECG were as accurate as the gold standard and 12-lead tele-ECG methods. There was almost complete agreement between the tele- and standard ECG concerning diagnoses for normal ECG, AV nodal blocks, bundle blocks, long QRS intervals, ST trait and T wave abnormalities.
The findings suggest that a simple device for ECG recording and interpretation may be useful in home care for elderly people. It is also simpler to apply the recording electrodes, since a trained nurse or caregiver is not necessarily required. The technique can provide a pre-hospital diagnosis of arrhythmias, atrio-ventricular blocks and repolarization abnormalities known to be associated with critical complications. 4 It should be emphasized that the 3-lead tele-ECG has lower cost compared to the 12-lead device. In the Italian medical system the use of the 3-lead tele recorder is approximately half the cost of the 12-lead recorder. The use of this simple and accurate device by patients, caregivers or non-medical staff can reduce the delay in obtaining heart disease treatment. It has been recently reported that immediate home ECG screening increased diagnostic rates by approximately 50%, in older patients with ST-elevated myocardial infarction. 16
There have been a few studies of the validity of tele-ECG recorders. 8,17–20 In a study on 20 patients with various heart conditions, 82% of the transmitted ECG tracings were correctly interpreted compared to the hospital-based ECG recorder. 21 To the best of our knowledge there have not been any studies validating the use a 3-lead tele-ECG in older patients with diverse heart conditions compared to the 12-lead tele-ECG and standard ECG recorders. However, the present study had certain limitations. The electrodes for both the 3- and 12- lead tele ECGs were applied by trained nurses and not by the patients themselves. On the other hand, when asked to re-apply the electrodes for the 3-lead recorder and activate the recorder, only one patient experienced difficulties. When the patients were asked to self activate the 12-lead tele-ECG, 75% (80/107) experienced significant difficulties and needed help from the medical staff.
Although further work is required, the present study demonstrates that the 3-lead tele-ECG is similar to the more sophisticated 12-lead tele recorder in older patients.