
Abstract
We have devised an inexpensive, web-based tele-ultrasound system using commercially-available video streaming equipment. We examined the spatial and grey scale resolution, and the delay time of the system. The receiving PC was tested at various distances from the transmitting site, from 3.2 km to 4828 km. Standard resolution targets and echocardiography movie strips recorded on DVDs were used to assess the image quality. A qualitative assessment was made by an expert sonographer. As the distance between the transmitter and the receiver increased, the scan smoothness decreased and the delay increased. At a distance of 3.2 km the delay was 2–3 s, and at 4828 km it was 10–15 s. The delay was short enough to allow realtime guidance of the scanning technician by telephone. The system allows inexpensive, readily available, realtime tele-ultrasonography.
Introduction
In tele-ultrasonography, transmission bandwidth is often a limiting factor. Several studies have examined the bandwidth needed to transmit ultrasound images. Early studies on tele-ultrasound used microwave links or ISDN 30 lines at 2 Mbit/s. 1,2 For remote fetal tele-ultrasound, a study analyzing the effect of bandwidth from 256 kbit/s to 2 Mbit/s on image quality found that 384 kbit/s was satisfactory, with little increase in perceived image quality when the bandwidth was increased to 1 Mbit/s. 3 A study of obstetric ultrasound found that the majority of images transmitted at 384 kbit/s were deemed acceptable by an observer, whereas the majority of images at 128 kbit/s were deemed unacceptable. 4
However, perception of image quality by experts might not be the best method of analysing scans. The desired end-point, clinical diagnostic accuracy, should also be assessed, and one study found that perception of image quality did not correlate with diagnostic accuracy. While there was no perceived difference in scan quality between 384 kbit/s and 1920 kbit/s, the lower bandwidth was associated with a significant rate of misdiagnosis (31% versus 15%), suggesting that higher bandwidth is required for accurate diagnosis. 5
Different clinical applications probably require different resolutions to ascertain clinically-important changes and thus require different bandwidths for transmission. A comparison of 256 kbit/s and 384 kbit/s for obstetric ultrasound found that both were similar, although 256 kbit/s had significantly more motion artefact, thus suggesting that tele-ultrasound of rapidly moving systems like the heart requires higher bandwidth. 6
In addition to the transmission of static ultrasound images or videos after performing the ultrasound examination, studies have been performed analysing the potential of realtime transmission of ultrasound images for immediate review. The development of guided ultrasonography from remote locations has been limited due to the need for high-bandwidth Internet connections and expensive proprietary software. 2,7–10 A bit rate of 0.6 Mbit/s at 30 frames/second was found to be the threshold needed to maintain image quality. 7 The development of high-speed Internet connections and inexpensive computer software has led to the development of an inexpensive system for transmitting video between two locations. 11 However, this system only delivered 3–6 frames/s, which was felt to be of marginal quality by experts, and was limited by the need for a video-capture card and a computer at the transmitting and receiving sites. A recent study was performed using 3-G mobile phone transmission to stream ultrasound video which found that the frame rate was low. 12
The literature in radiology, obstetrics and cardiology all support the power and utility of realtime ultrasound. However, their adoption has been limited by the cost. In order to make tele-ultrasound more feasible, we have devised an inexpensive, web-based tele-ultrasound system using commercial video streaming equipment. We have examined the spatial and grey scale resolution and delay time of the system at varying distances between source and receiver.
Methods
The video streaming device (Slingbox PRO, Model SB100–100, Sling Media, Foster City, CA, USA) was inexpensive (US $180) and relatively small (35 cm wide, 4 cm tall, 12.5 cm depth with a weight of 0.55 kg). The analogue composite video, or S-video, output from the ultrasound system was connected to the video input on the Slingbox (Figure 1). The Slingbox compressed the video using a standard codec (Windows Media 9) and optimized the video stream automatically for the available bandwidth. A high speed, broadband Internet connection (384 kbit/s upload; 1.5 Mbit/s download) was used both at the transmitting and receiving ends. At the receiving end, software (SlingPlayer 2.0) was used to receive the image on a laptop computer. The system incorporated both encryption and password protection. All data was sent in encrypted format.
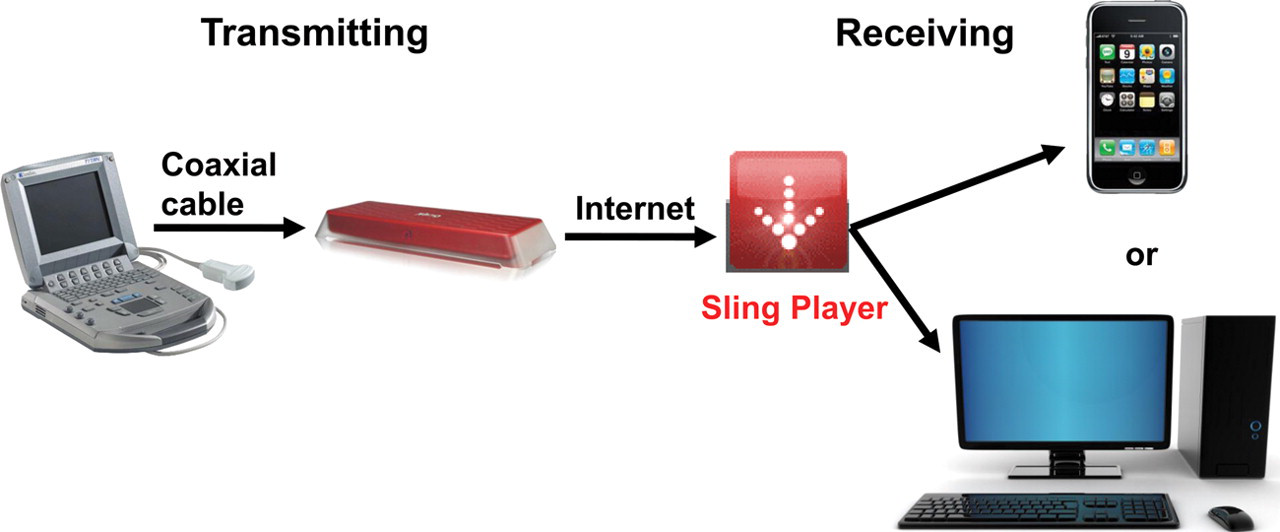
The Web-based, realtime tele-ultrasound system. At the transmitting end there is an ultrasound machine connected by an analogue composite video cable to the Slingbox. At the receiving end there is a PC with the software SlingPlayer. The software can also be used on mobile devices such as iPhones, BlackBerries and Palms. Both ends need an Internet connection
Image assessment
Image delay was assessed by people at the transmitting and receiving ends who were in telephone contact when image transmission began. A stopwatch was used to determine the delay time at the receiving end. Each measurement was averaged over three transmissions.
Transmitted image quality was assessed in two ways: a standard resolution target transmission and review of common ultrasound images for quality. For assessing the system and determining its grey scale and spatial resolution, standard resolution targets and echocardiography movie strips were recorded on DVDs. A DVD Player (LiteOn It Inc, Fremont, CA, USA) was used to play the resulting DVD with resolution targets and echo movie strips, and the analogue video output from this device was connected to the video input of the Slingbox.
Study design
The receiving PC was tested at various distances from the transmitting site in the US: at 3.2, 402, 2414 and 4828 km. Thus many Internet nodes were traversed in the transmission path. The image was also assessed through qualitative review of the image quality and smoothness of videos. The qualitative review was performed by an expert sonographer and judged subjectively from poor to excellent and also a diagnosis was determined from the images. The total of 14 transmitted cases included vascular, cardiac, gallbladder and liver pathology of de-identified patient teaching cases.
Some difficulty was experienced in recording the transmitted images without severe degradation of image quality. We tried different methods of generating the videos, including the use of camcorders, but all resulted in significant image degradation due to the proprietary encryption system used by the Slingbox and our inability to save the transmitted video files directly. The best method we found was using Debut Video Capture Software (NCH Software Inc, Greenwood Village, CO, USA) to capture the transmitted video images from the computer screen and record them in a video file. Using this technique, the main degradation in the videos was the frame rate when they were played. Some example video images are available as online supplements (See website). The recording software used for both image and video recording was the At-Large Recorder 2 (Applian Technologies, San Anselmo, CA, USA).
Results
Evaluation of the transmitted standard resolution targets (Figure 2) and echocardiography movie strips showed an image that was deemed acceptable for clinical management for all transmitted Internet speeds. We attempted different connection bandwidths by altering the location (with known different Internet speeds) of ultrasound transmission and receiving to include standard bandwidths from 56 kbit/s to 10 Mbit/s. We found that only with dial-up 56 kbit/s Internet speed did the images appear pixelated. Bandwidths of 384 kbit/s achieved good quality images without pixelation and degradation found at lower bandwidths. Pathology was readily apparent in the transmitted cases, including gallbladder (Figure 3A), vascular (Figure 3B), cardiac and liver pathology.

Standard resolution target images. The recorded images demonstrate the output from the SlingBox after transmission and recording. The most severe degradation occurs in the final recording of the data
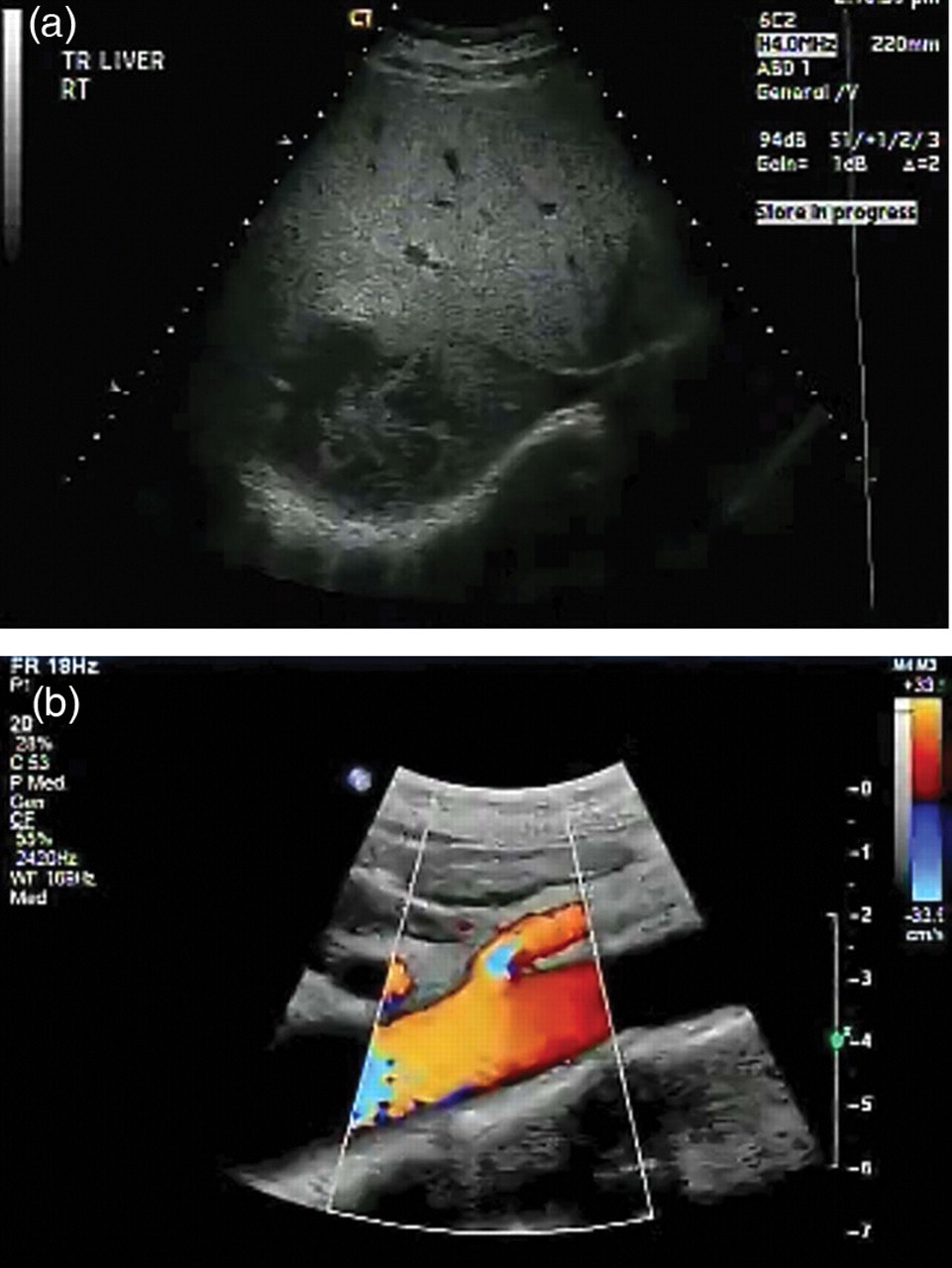
Recorded ultrasound images. A. Liver with a mass. B. Abdominal aorta and superior mesenteric artery
As the distance between the transmitter and the receiver increased, the scan smoothness decreased and the delay increased (Figure 4). At a 3.2 km distance between transmitter and receiver, the delay was 2–3 s. This delay was the same at 402 km separation, but increased to 5–6 s at 2414 km and 10–15 s at 4828 km. The delay was short enough to allow realtime guidance of the scanning technician by telephone.

The relationship between the time delay between transmission and reception and the distance between the sites. Note the log scale
Discussion
In the present study, the quality of transmission was assessed by two tests: standard resolution target transmission and a review of image quality. In future work, we think this could be expanded to include a panel of expert opinion about the diagnostic accuracy of ultrasound to test its clinical utility. It would also be useful to develop a recording system to allow readers to review the images themselves without such a severe degradation of the image as we obtained using the At-Large Recorder 2.
For the purpose of guiding a less experienced sonographer at a remote location, the Slingbox provided robust transmission so that the best possible pictures could be obtained in a given circumstance. The resolution necessary to achieve clinical utility in realtime tele-ultrasound is probably low, especially for imaging static organs. If there is a need for increased resolution, a single frame of video could be transmitted without compression to improve both the grey and spatial resolutions. A realtime guided system can guide less experienced ultrasound scanners to achieve ideal scanning locations and images in a given patient.
With an inexpensive Slingbox connected to an ultrasound machine and using a broadband Internet connection, an ultrasound scan can potentially be transmitted around the world with little loss of resolution and a delay of only a few seconds. The recipient only needs free software, which is available for a variety of operating systems including Windows and Macintosh computers, and mobile devices like the Palm, iPhone and BlackBerry. The transmitted data is encrypted and only one user is allowed to view the signal via password protection, thus ensuring patient confidentiality in the scan transmission.
Footnotes
Acknowledgements
We thank D Elliott Wolfe, Thomas Tsai, Maneesh Singh and the students and teaching assistants of Medicine 227: Bedside Ultrasound course at the Stanford School of Medicine. We also thank the engineering students from Dr Thompson's course.