
Abstract
Mobile phones provide a low cost method of addressing certain health system needs in developing countries. We examined SMS-supported interventions for prevention, surveillance, management and treatment compliance of communicable and non-communicable diseases in developing countries. We searched both peer-reviewed and grey literature reporting the use of SMS messages for disease prevention, surveillance, self-management and compliance in developing countries. A total of 98 applications fulfilled the inclusion criteria (33 prevention, 19 surveillance, 29 disease management and 17 patient compliance applications). In 31 projects, the SMS applications were evaluated. The majority of applications focused on HIV/AIDS and were located in India, South Africa and Kenya. Most used bulk (push) messaging. In general, they were well accepted by the population. The review provides further evidence that mobile phones are an appropriate and promising tool for disease control interventions in developing countries.
Introduction
There is increasing interest in using mobile phones for health purposes (m-health). Much of the evidence for the effectiveness of m-health comes from work conducted in industrialized countries.
1,2
With the expansion of mobile phone coverage in the developing world, m-health is becoming a possible tool for health care. However, little is known about current practice, the effectiveness or the acceptability of m-health applications for disease control in developing countries.
3
The purpose of the present study was to examine current practice for using SMS for disease prevention, surveillance, management and treatment compliance in developing countries. We aimed to answer the following questions:
Where are the SMS health interventions taking place? What diseases and purposes are SMS health interventions used for? What types of communication are used in SMS health interventions? What are the outcomes of SMS interventions? What recommendations can be made to researchers, practitioners and policy makers regarding the future of the use of SMS in m-health development, implementation and evaluation?
Methods
We searched both peer-reviewed and grey literature. The decision to include grey literature evidence was motivated by a suggestion 4 that both grey and scholarly evidence should be included in reviews of new topics in order to reduce bias and improve the estimate of the effects of interventions. Documents and papers were included when they were related to interventions using SMS for disease prevention, surveillance, management or treatment compliance of communicable and chronic diseases in developing countries. Developing countries were identified from the International Monetary Fund's (IMF) World Economic Outlook 2008 report under the category “developing and emerging economies”. 5
Search
A search was performed for documents published between January 1998 and July 2009. The search terms were used with AND/OR and included:
health promotion, public health, preventive health services, disease prevention, population surveillance, patient compliance, patient care management, disease management, self care, HIV, acquired immunodeficiency syndrome, tuberculosis, communicable diseases, communicable disease control, chronic disease, non-communicable disease, cellular phone, mobile phone, cell phone, SMS, MMS, text messag*, picture messag*, developing countries, developing world, Asia, Africa, South America, Latin America, Europe, Eastern.
When possible, terms were translated into French and German (languages known by the research team), to reduce the potential bias of including only English language papers. The grey literature search strategy searched reports from sources, such as newspaper, magazine, research institutes, NGOs, think tanks or individual health projects, conference proceedings, websites, blogs, listserv or personal communications. 6 The strategy consisted of eight steps (see Table 1).
Search strategy

Data collection
Following the search, eligible documents were retrieved. Two members of the research team independently verified eligibility and full agreement on eligibility was achieved. Data extraction was based on suggestions provided in the Cochrane Handbook for Systematic Reviews of Interventions 7 and included information on author, year of publication, country setting, health topic and purpose, target population, sample size, intervention description, outcomes measured, results, conclusion and limitations. Data for each variable were taken directly from each paper. When data were not clearly stated (e.g. “the aim of the application was to…”) the coder read the full paper to ascertain that information. Conflicts were resolved through discussion.
Results
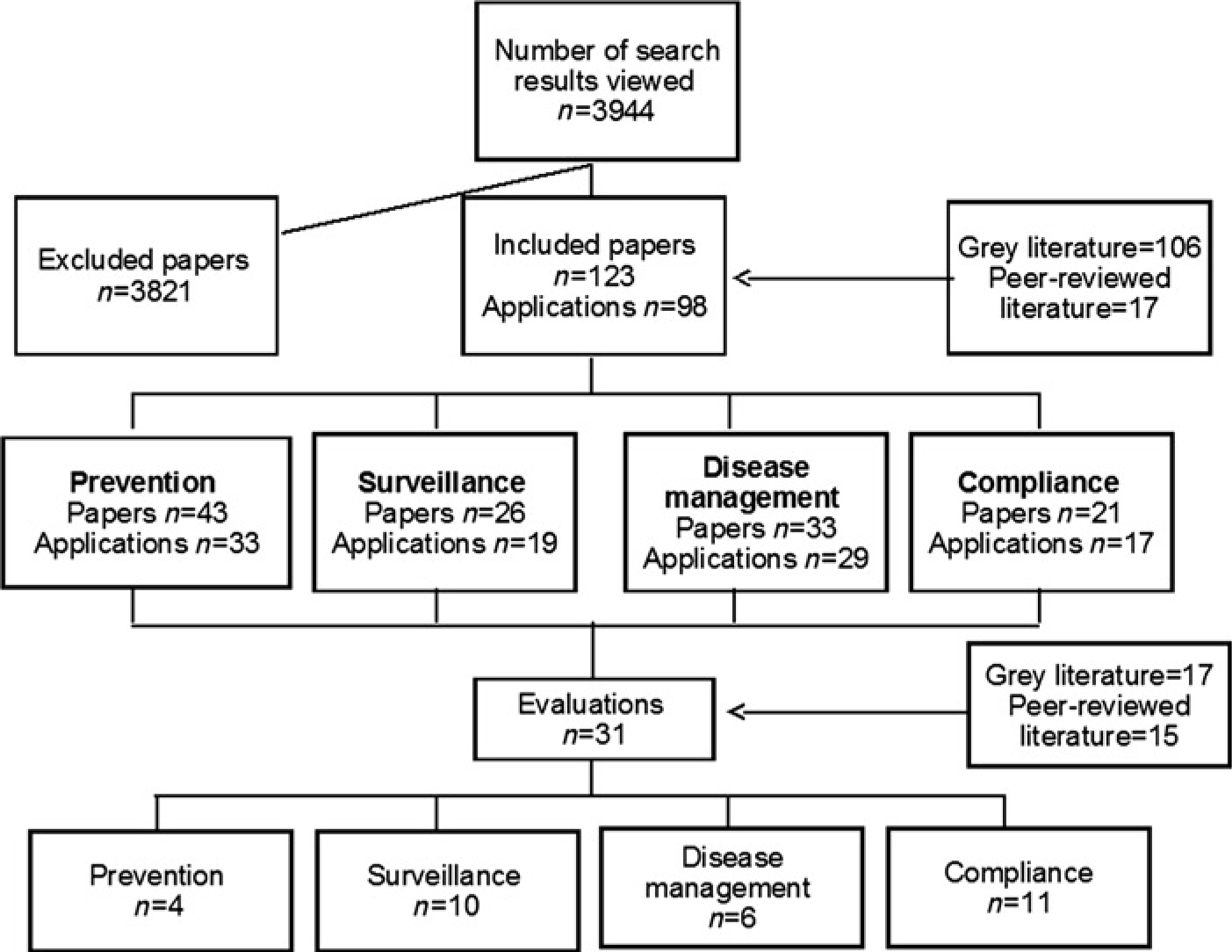
In the first screening, nearly 4000 citations were identified, see Figure 1. An additional 21 papers were retrieved through personal communication and another 17 by hand searching the reference lists of eligible articles. After an initial view of abstracts and titles, most were excluded because they related to industrialized countries, did not concern SMS applications, or did not report the development, implementation or evaluation of an SMS application for health. The final sample included 123 of eligible papers that reported 98 applications. Seventeen of the papers came from peer-reviewed sources and 106 from grey literature sources. Thirty-one evaluations were reported, of which 13 were published in peer-review literature.
Search results
Location of SMS health interventions
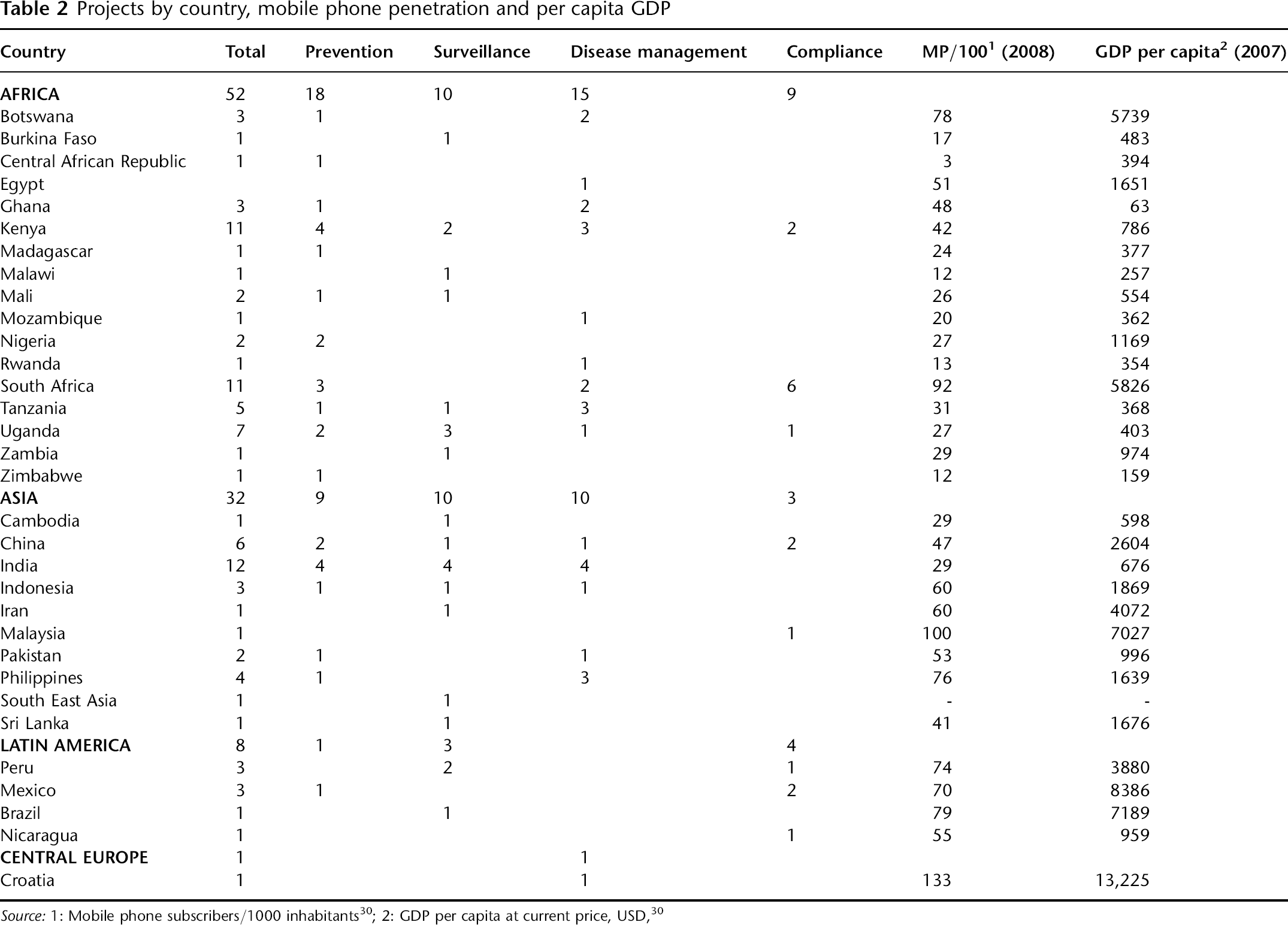
Although projects extended across all regions, initiatives were concentrated in several countries (see Table 2). Africa had the largest number of projects (n = 53) followed by Asia (n = 32). In Africa, applications were included from 17 different countries, but most took place in South Africa (n = 11) and Kenya (n = 11). In Asia, India had the highest number of applications (n = 12), followed by China (n = 6).
Projects were more frequent in emerging mobile phone markets, such as South Africa with higher household penetration (85–90%) and higher GDP per capita than neighbouring countries. 8 Many other African projects were concentrated around the Great Lake region, namely Kenya, Tanzania and Uganda, where the mobile market recently witnessed a significant increase in coverage and penetration. 8
Projects by country, mobile phone penetration and per capita GDP
Purposes of the SMS health interventions
The majority of the 98 interventions focused on HIV/AIDS (n = 29). Others concentrated on sexual and reproductive health (SRH) (n = 7), tuberculosis (TB) (n = 6), malaria (n = 6), avian influenza (n = 4) and a wide range of others with one-two interventions targeting them. In some cases applications targeted more than one disease, most of which were focused on disease management (n = 16). 34 interventions were designed for multiple conditions and diseases.
The interventions included 33 for disease prevention, 19 for disease surveillance, 29 for disease-management and 17 for improving compliance with a health treatment (see Table 3). The 33 disease prevention interventions aimed to provide the public with information about resources, services and health behaviours. The most common prevention topic addressed was the transmission of HIV (n = 19). The 19 SMS-based applications for disease surveillance were primarily used for tracking infectious diseases, including malaria (n = 1) and Avian Influenza (n = 2), but also included surveillance of malnutrition (n = 1). The 29 disease management interventions were used to monitor patients at homes or in clinics, support remote health workers, facilitate communication between health workers and patients, provide a way to record medical data, and for clinical diagnostic decision support and telemedicine. Most interventions targeted multiple diseases (n = 16). Finally, 17 compliance programmes were used to boost patient compliance with reminders for medication or appointment and the majority focused on patients with HIV/AIDS (n = 10) or TB (n = 3). Details about interventions are further described in Tables 4–7 (see online only supplementary data:
SMS-based interventions by diseases and areas of applications
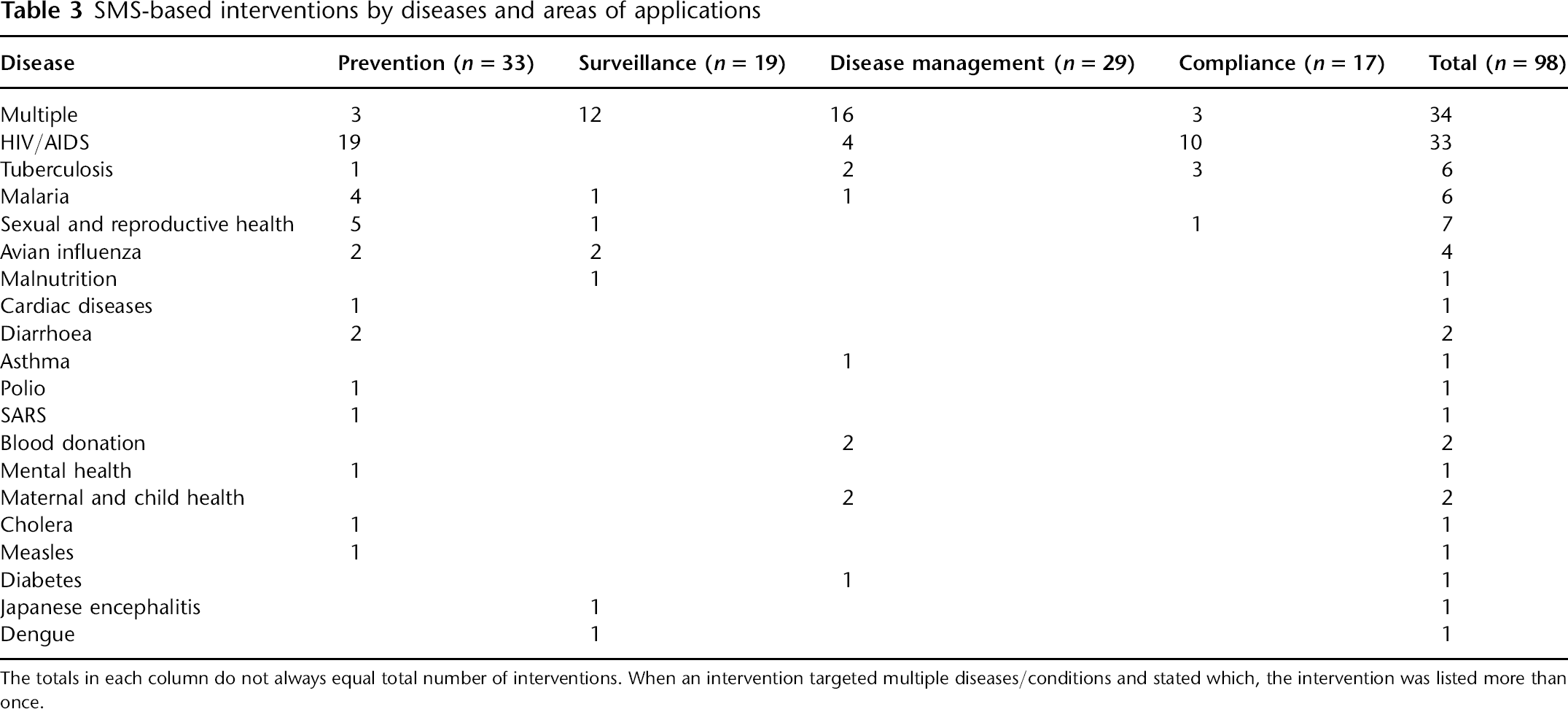
The totals in each column do not always equal total number of interventions. When an intervention targeted multiple diseases/conditions and stated which, the intervention was listed more than once.
Types of communication in SMS health interventions
Intervention mode and communication initiation varied between projects (see Tables 4–7, available online only at
Excluding preventive activities, most interventions were interactive, allowing participants to send in texts and receive a response, play games and quizzes and obtain feedback. They were initiated by face-to-face contact, enabling participants to consent to using the service. Incentives were used for preventive and compliance interventions, in particular in the form of mobile phone airtime or handsets. One compliance programme treated SMS slightly differently from the others. The mobile phone served as a social network for medication compliance and social support with each SMS message sent by users going to every subscriber to the service. 10 Users could then respond to questions and to concerns others raised.
Outcomes
Of the 98 interventions, 31 assessed the effectiveness of SMS interventions (see Table 8, available online only at
Prevention
Of the 33 disease prevention interventions, four reported the results of an evaluation, all of which were published in the grey literature. All were process outcomes and none included information about behaviour change. Nevertheless, case studies reported that such interventions were well accepted by the population. While some projects used incentives, the effect and level of interaction and the use of incentives on patient satisfaction and retention were not explored. Participation decreased if the campaign was deemed too long, even when using games. Differences in utilization, responses and perception between urban and rural areas, as well as between men and women were observed. Language problems, SMS cost, anonymity, data security, 21 high mobile phone turnover in the population and mobile network fluctuations were also reported as concerns and potential barriers. 22
Disease surveillance
Of the 19 disease surveillance interventions, 10 reported an evaluation. Four of the ten evaluations were published in the peer-reviewed literature. Most interventions were found to be feasible, see Table 8.
Peer-reviewed studies showed promising results in reducing transmission delays and error rates, as well as saving time compared to conventional paper-based systems. However, there were no statistical comparisons between areas or groups. Case studies emphasized that users believed SMS reporting to be easier, faster and more reliable compared with paper-based systems. They valued immediate communication in case of emergencies but also for day-to-day activities. Cost, mobile network coverage, electricity access and high personnel turnover 17 were perceived as potential challenges. Over-reporting and duplicates were also reported in some projects.
Disease management
Of the 29 disease management interventions, six reported evaluations; one was published in the grey literature. 23 Information on clinical outcome was found in one RCT, which reported significant clinical improvement. 13 Applications helped to facilitate communication between remote health workers and specialist, 15 and to register and monitor patients. Pilot project reports showed that both patients and health workers had positive perceptions of using mobile phones for healthcare delivery. It was also shown that a country-wide rollout of a health information system for HIV/AIDS was possible. 24 Cost, charging the phone as well as data accuracy and consistency were problems reported in the disease management interventions.
Patient compliance
The 17 compliance interventions ranged from basic SMS reminders systems to more complex applications for monitoring treatment and appointment adherence. Eleven of these were evaluated. Most compliance projects targeted HIV/AIDS (n = 10) and TB (n = 3). Timing of message delivery seemed to be important. In one study, 40% of the TB patients said that the nurse selected the time that the TB treatment reminder would be sent each day. 25 As 50% of patients did not carry their medication when not at home during the day, if the prompt arrived during the day, they were not able to take it at the time of the prompt. In another study, 35% of patients said they took their medication more than 30 min after the reminder was sent. 18
Five of the compliance studies examined health outcomes, and some clinical improvements were observed after the interventions. An evaluation of an application aiming to improve TB treatment adherence showed slight improvement of treatment completion rate, but no improvement of the cure rate. 25 Two similar RCTs reported significant improvement of attendance rate to primary healthcare appointments with telephone and SMS reminders, and one suggested that SMS messaging could be cost-effective. Another project reported a reduction in patient non-attendance at follow-up appointments with SMS alerts for HIV/AIDS medication and appointment reminders. 26 An RCT examined the effects on adherence to hypertension treatment and found a significant increase in patient understanding of the importance of adherence (83% vs. 20% in the control group) and increased knowledge about hypertension, but no difference in blood pressure change. 27 Other descriptive and qualitative surveys reported good acceptance of such interventions. SMS-based support groups also seemed to improve the well-being of patients suffering from the isolation of stigmatizing and chronic diseases. 10 An implementation model showed the need to facilitate ownership and maintain face-to-face relationships. 25 The main challenges were language barriers, difficulty in monitoring adherence and receiving feedback, as well as confidentiality and data protection concerns.
Discussion
The present paper provides the first summary of practices and outcomes of SMS interventions for disease control in developing countries.
Where were the SMS health interventions taking place?
Most interventions took place in Africa with variation among countries. Geographical differences may result from the tendency of aid organizations to group their efforts and focus on key countries, thus creating a kind of “prototype” or “pilot” country. But the localization of the projects may also be influenced by the penetration of mobile services, itself correlated with network coverage and per-capita income (Table 2). Market conditions and the availability of an ICT policy may also affect the adoption of m-health applications.
For what topics and purposes were SMS health interventions used?
The largest number of applications focused on HIV/AIDS. This may be because patients play a key role in the fight against this pandemic. It is vital that individuals comply with preventive measures (e.g. condom use), are tested to find out if they have the virus, and if infected, adhere to treatment and comply with medication and clinic appointments. A large body of work has focussed on improving patient-centred HIV/AIDS care and the type of knowledge required to prevent the spread of and manage HIV and AIDS. This may be well suited for short messages that prompt specific actions, such as using a condom or going to a local clinic to be tested. Moreover, given the burden of the pandemic in developing nations combined with human resource and financial burdens, SMS may be one of the most cost-efficient methods of reaching a mass audience.
What types of communication are used?
Previous research found that most of the behaviour change interventions using SMS (nearly all in industrialized countries) used tailored messages adapted to the participant's name, nickname, age, gender, timing preferences or personal barriers. 28 In the present study, initiatives used a mixture of tailored and generic messages. Prevention applications tended to use generic messages, while surveillance, disease management and compliance tended to use tailored messages. This is probably the result of the purpose of the applications, which in most cases was clinical management and communication between health workers and with their patients. In one case, the communication was peer-to-peer with each message sent over the network to all its members. 10 This provided social support for medication adherence, feelings of anxiety and depression, and about feeling stigmatized from living with HIV.
What are the outcomes of SMS interventions?
Promising findings were found in the four key areas of applications, see Table 8. Overall, text messaging seemed to improve the process of care and was well accepted by both health workers and the targeted population. The majority of users and beneficiaries were familiar with mobile phones and SMS for private and professional utilization, and the technology was reliable. Moreover, they reported that mobile phones could bring new opportunities to improve their health. 29
While there was evidence suggesting that mobile phones are a promising channel for health communication and disease control, there was a lack of high quality SMS-based intervention studies in the peer-reviewed literature, especially those measuring clinical outcomes. Most outcomes reported were process and satisfaction. Of the 98 applications included in the present review, 31 had been evaluated and 15 of those evaluations were reported in the peer-reviewed literature. Nonetheless, the characteristics of SMS present considerable advantages for controlling disease in developing countries. There are opportunities in mass awareness campaigns, tailored behavioural change communication, enhanced diseases surveillance, support for remote health workers by facilitating patient registration and clinical decision making as well as for patient compliance. Indeed, several of the evaluations in the present review showed promising results. Further research is required on need, relevance, applicability and cost-effectiveness.
Limitations
The present review had certain limitations. The innovative aspects and the commercial implications of the field may have affected the reporting of studies. The findings could have been influenced by a tendency to highlight positive results, by the time lag problems of a fast-moving field, or by unwillingness to share information in order to protect innovation. There may have been involuntary omission of documents from the grey literature, which can be difficult to find. In addition, there may have been relevant papers in other languages, e.g. Chinese.
Conclusions
The findings of the review can be summarized in the following three recommendations:
Establish monitoring and evaluation of projects with assessment of clinical and economic outcomes; Promote high quality research to facilitate better-informed decision making; Encourage collaborative design and implementation that involves the target population and stakeholders in the design of the programme.
The main challenges will be putting these recommendations into policy and practice. Nonetheless, the use of m-health to improve and support public health and health care delivery in developing countries appears promising.
Footnotes
Acknowledgements
We thank Ms Sepideh Dianat and Mr Joel Lehmann for their assistance.