
Abstract
We assessed the feasibility, image adequacy and clinical utility of a tele-echocardiography service which combined video compression with low-bandwidth store-and-forward transmission. Echocardiograms were acquired by a hospital geriatrician, compressed and transmitted using both near real-time (urgent) and delayed (pre-programmed) protocols via an Internet connection to the notebook PC of a remote cardiologist. Clinical utility was evaluated as a change in therapeutic management. During a one-year period, 101 tele-echocardiography consultations were successfully performed (feasibility = 100%) on 95 patients (age 22–95 years), admitted with cardiovascular or neurological diagnoses (24% of the consultations were urgent). In total, 4617 files (1.4 GByte of data) were transmitted, 2669 of which were short video clips. On average, 46 files (13.8 MByte) were transmitted (mean duration 10 min) at each examination. Consultations (both urgent and pre-programmed) were clinically useful in 83% of examinations. Logistic regression analysis showed that both a low left ventricular systolic function and the examination indication were determinants of clinical utility. The transmitted images were considered adequate for diagnosis in 100% of the pre-programmed teleconsultations. Tele-echocardiography using MPEG-4 video compression is a feasible, adequate and clinically useful tool for telemedicine.
Introduction
Tele-echocardiography can provide diagnostic imaging information to care providers independently from the location of the specialist. Previous clinical studies in tele-echocardiography have used video transmission techniques combined with videoconferencing. This requires high-bandwidth transmission. 1,2 The aim of the present study was to analyse the feasibility, image adequacy and clinical utility of a tele-echocardiography service established by a geriatric institute. This service combined video compression with low-bandwidth store-and-forward transmission of digital imaging data.
Methods
A prospective study was performed, to examine the feasibility, image adequacy and clinical utility of echocardiographic imaging transmitted between an echocardiographer and a cardiologist. The study was performed at the Golgi-Redaelli institute, a 630-bed rehabilitation unit in the Milan area. We included all consecutive echocardiography examinations performed over a one-year period from January 2008. Echocardiograms were requested by the medical staff (20 physicians). They were performed by a hospital geriatrician with expertise in transthoracic echocardiography (level I, ASE standards), who decided on the clinical priority of the examinations (urgent or routine). Routine echocardiograms were performed once a week, with an ultrasound unit (Sonoline G50, Siemens AG) fitted with a multi-frequency transducer (P4–2 Siemens AG). The acquisition protocol is shown in Table 1. All echocardiograms (urgent and routine) were reviewed remotely by a single consultant cardiologist, expert in echocardiography (level III, ASE standards), who discussed the echocardiographic findings with the operator, requested modifications or corrections to the scanning protocol if necessary, and decided modifications of patient therapy or management after discussing the clinical status with the geriatrician.
Echocardiographic imaging protocol
CW: continuous wave; PW: pulsed wave
Echocardiography transmission
All echocardiograms were transmitted between the institute and the portable PC of the consultant cardiologist through a low-bandwidth Internet connection. The analogue video output (s-VHS) of the echocardiography unit (image resolution 720 × 576 pixels) was fed into an analogue-to-digital conversion board (Movie Box DV, Pinnacle, Norderstedt, Germany), connected to a PC (Figure 1). Using the client side of custom-made software, the operator acquired the standard cine-loops (1–3 s duration), which were compressed (using the Microsoft MPEG-4 Windows Media Video 7 codec), cropped (to remove patient-related information), and both stored locally and transmitted to the server side of the software installed on the portable PC of the cardiologist. The original examination cine-loops were also stored locally on the ultrasound unit. Still frames were acquired with JPEG compression.
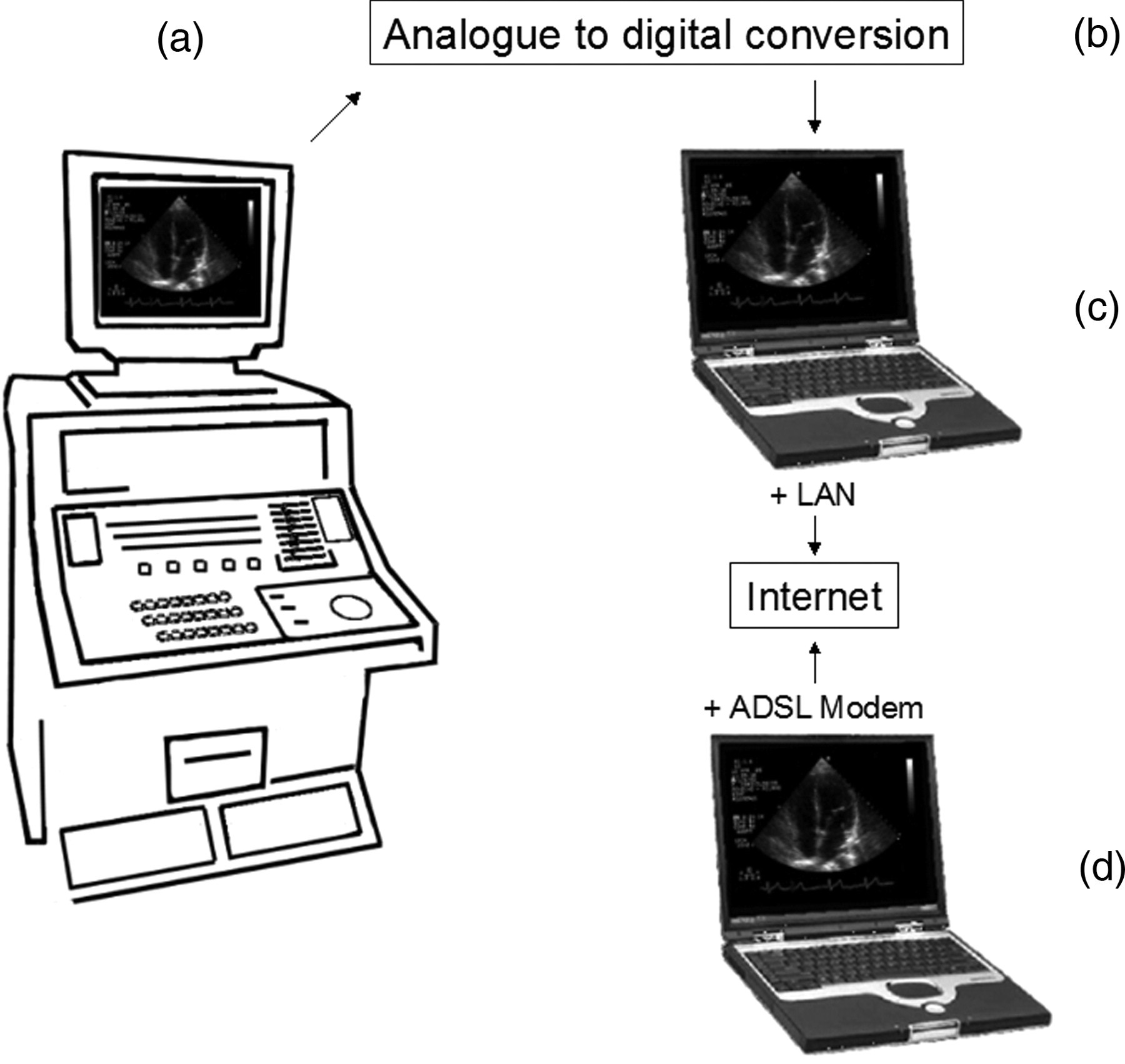
Tele-echocardiography acquisition-transmission system. The analogue video output of the echocardiography unit (a) is converted (limited compression) to digital video (MPEG-2) (b), which is formatted and compressed to user-defined MPEG-4 video files using software on a client notebook (c) connected to a server notebook (d) through an ADSL connection
The Internet transmission used the IP protocol over an ADSL connection (upload speed 200 kbit/s; download speed 1 Mbit/s). Patient clinical information was transmitted separately as a text file. Software password-protection, image cropping and use of VPN transmission ensured the security of patient data. The transmitted files were stored in a database on the server, which had the potential to receive video files from multiple PCs. The transmission protocol was initiated upon agreement between the geriatrician and the cardiologist. Urgent echocardiograms were transmitted online during patient scanning (in near real time modality for urgent consultations), whereas routine examinations were transmitted offline, after the scanning sessions (delayed modality for pre-programmed consultation). The transmission of the video files was always performed in store and forward modality. The term “near real-time”, which was used for the urgent teleconsultations, was because of the slight transmission delay that occurred for each video file. Thus, the video files during the urgent consultation were available on the server side within a few seconds of being uploaded on the client side.
Echocardiography data
We analysed the following information for each patient: demographics; number of echocardiography files acquired, subdivided by still frames and video clips; minimum and maximum dimension of acquired files; total size (MByte) of the transmitted files; total duration of file transmission; type of transmission (near real-time or delayed); clinical indication of the echocardiographic examination; echocardiographic diagnosis; left ventricular (LV) ejection fraction class (normal or reduced: <45%); analysis of LV diastolic function (performed/not performed); systolic pulmonary hypertension (normal or increased >40 mmHg); pericardial effusion (present/absent); image adequacy and utility of the teleconsultation (see below).
The quality of the imaging (acquired and transmitted by the geriatrician) was defined by the consultant cardiologist as adequate (additional imaging not required) or not adequate (additional imaging requested). Furthermore, a random sample of 100 original cine-loops (stored on the ultrasound unit) and 100 corresponding compressed cine-loops were evaluated blindly in random order by a second cardiologist (with level three experience in echocardiography), who judged image quality as adequate or not adequate for clinical use.
The clinical utility of the echocardiographic teleconsultation was defined as a change in therapeutic management based on the additional information provided by the consultant cardiologist through tele-echocardiography. In this respect, either a new finding (e.g. a significant pericardial effusion prompting diuretic therapy or pericardiocentesis) or the exclusion of a clinical suspicion (e.g. cardiogenic dyspnoea) were considered clinically useful echocardiographic findings. Utility was assessed by consensus of two of the researchers, based on the clinical and echocardiographic data.
Statistical analysis
The chi-square test was used to compare different categorical variables between near real-time and delayed, and between clinically useful and non-useful, echocardiographic teleconsultations. Logistic multiple regression analysis was used to screen for significant predictors of the clinical utility of the tele-echocardiographic consultation. Statistical analysis was performed with a standard package (SPSS version 8.0, IBM Corporation, New York, USA).
Results
Over the 12 month study period, 101 tele-echocardiographic consultations were requested for 95 patients (in six patients, two consultations were performed at separate times). No technical problems were noted during acquisition, compression and transmission of the echocardiography video clips during the delayed consultations (which were the majority, 76%) or the near real-time consultations (24%).
File acquisition and transmission
The patient demographics are summarised in Table 2, which also shows the number of still frame and video files acquired and transmitted to the cardiologist, and the duration of file transmissions. The number of files acquired for each patient reflected the standard echocardiographic acquisition protocol used (complete examination when feasible, Table 1). Use of MPEG-4 compression during file acquisition reduced the video file sizes, so the maximum transmitted for any examination was 25.5 MByte. There was a wide difference in the duration of file transmission between near real-time and delayed echocardiography teleconsultations (Table 2), because during the latter the video files were transmitted sequentially without interruptions, whereas during urgent, near real-time teleconsultations the duration of the transmission was equal to the total duration of the echocardiography examination (and the cardiologist could follow the whole echocardiography examination). The remaining file acquisition and transmission variables were similar between near real-time and delayed teleconsultations (Table 2).
Patient demographics, and echocardiographic acquisition and transmission data
* P < 0.001, near real-time vs. pre-programmed teleconsultations
Echocardiographic data
The indications for the requested echocardiography examinations were: assessment of valve function (heart murmur) (20 patients); dyspnoea (24); evaluation of LV function and mass (31); chest pain or suspected myocardial infarction (10); suspect endocarditis (3); suspect pericardial effusion (7); assessment of left ventricular function prior to/during chemotherapy (2); other (4). Echocardiographic diagnoses included: normal examinations (14 patients); wall motion abnormalities in coronary artery disease (33); dilative and hypertrophic cardiomyopathies (3); hypertensive heart disease (16); aortic valve stenosis (9); mitral valve regurgitation (15); volume/pressure overload of the right heart (4); paroxysmal atrial fibrillation (3); miscellaneous (4). There were no differences between near real-time and delayed echocardiography teleconsultations, except in LV diastolic function, which was performed more frequently in the near real-time consultations (Table 3). The transmitted imaging was considered adequate to answer the clinical indication, and the cardiologist, in all the 77 pre-programmed teleconsultations, requested no additional scanning. On the other hand, because of the near real-time interaction between the geriatrician-operator and the cardiologist, imaging adequacy could not be objectively evaluated in the 24 urgent teleconsultations. Furthermore, all of the randomly selected images were judged as adequate for clinical use by the second cardiologist.
Differences in echocardiographic variables between pre-programmed (delayed) and near real-time (urgent) teleconsultations
* P < 0.01 (chi-squared analysis)
Clinical utility of the teleconsultations
The echocardiographic teleconsultation was considered clinically useful in 84/101 examinations (83%), and this proportion was similar for near real-time and delayed consultations (Table 2). In the logistic regression analysis, both a low ejection fraction and the indication for echocardiography were independent predictors of the clinical utility of the teleconsultation (P = 0.035). All the indications were related to clinical utility (Figure 2), with the exception of half of the examinations requested for heart murmurs/valve function and half of the examinations requested for evaluation of LV function and/or mass. Finally, the utility of the teleconsultation was evenly distributed across all the echocardiography diagnoses considered, see Figure 3.
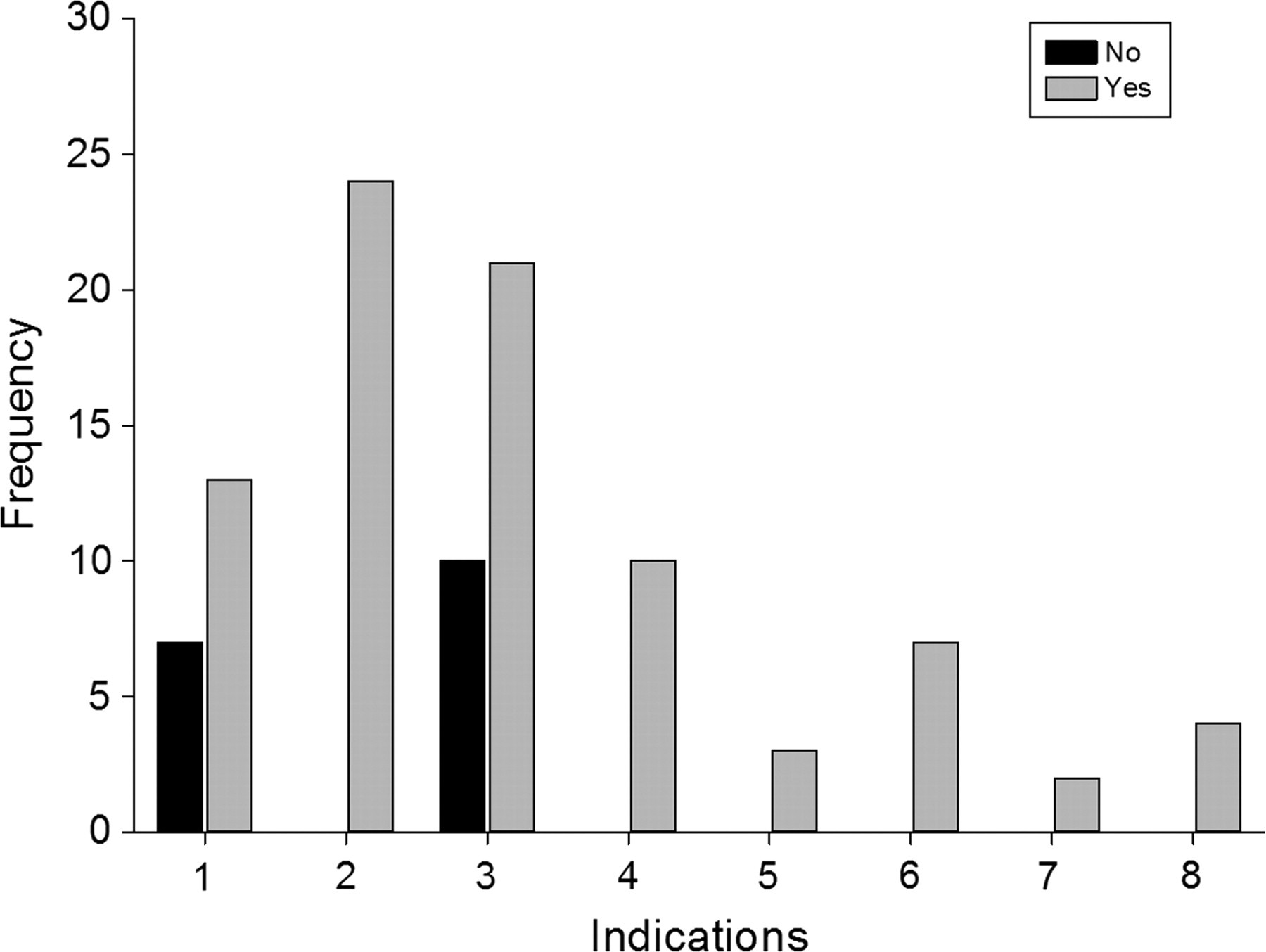
Utility of the teleconsultation in relation to the examination indication. The indications are: (1) Assessment of valve function; (2) Dyspnoea; (3) Evaluation of LV function and mass; (4) Chest pain or suspected myocardial infarction; (5) Suspect endocarditis; (6) Suspect pericardial effusion; (7) Assessment of left ventricular function prior to/during chemotherapy; (8) Other

Utility of the teleconsultation in relation to the echocardiography diagnosis. The diagnoses are: (1) Normal; (2) Wall motion abnormalities in coronary artery disease; (3) Dilative and hypertrophic cardiomyopathies; (4) Hypertensive heart disease; (5) Aortic valve stenosis; (6) Mitral valve regurgitation; (7) Volume/pressure overload of the right heart; (8) Miscellaneous; (9) Paroxysmal atrial fibrillation
Discussion
The present study is the first to report the use of low-bandwidth, store and forward transmission of complete echocardiograms for teleconsultation purposes in a clinical setting. In contrast, previous experiences have made use of videoconferencing transmission modalities requiring high bandwidth and non-validated (for clinical echocardiography) video compression codecs. 1–13 Our study confirms the feasibility, adequacy of imaging and the clinical utility of low-bandwidth, store and forward tele-echocardiography.
Low- vs. high-bandwidth tele-echocardiography
The DICOM standard in echocardiography is characterized by a low degree of digital compression of the echocardiographic cine-loops. 14,15 A typical standard transthoracic examination may thus produce up to 200 MByte of data, which is cumbersome to transmit if a high bandwidth connection is not available. In contrast, in our study a mean of 13.8 MByte of video files was transmitted over a 10 min period. Although the DICOM standard is considered the standard for digital echocardiography, most of the tele-echocardiography work which has been published has used proprietary non-DICOM techniques for real-time video transmission. 1–13 However, a high bandwidth connection is required. Few codecs used in commercially available videoconferencing equipment have been validated for use with clinical echocardiography: that is, the loss of information during lossy compression has not been related to the quality of imaging and its diagnostic content. 16 The solution described in the present study combines a store and forward transmission modality (rather than real-time video transmission), a validated MPEG-4 video compression technique (rather than DICOM video or non validated videoconferencing codecs), and low cost/low-bandwidth transmission channels (Internet ADSL with VPN) instead of expensive high-bandwidth connections. 1 This combination of low-cost, readily available technologies has not been described previously, and makes tele-echocardiography projects feasible.
Real-time vs. store and forward transmission
Previous experiences in fetal, paediatric and adult tele-echocardiography have commonly made use of real-time video transmission techniques combined with videoconferencing equipment, 1–13 rather than store and forward transmission of cine-loop video. 17,18 However, there are a number of advantages of store and forward transmission.
The video quality of real-time transmission depends on the available bandwidth, and a change in bandwidth may significantly reduce the diagnostic value of the ultrasound examination. 10 In contrast, in store and forward modality the quality of a transmitted video clip depends on the compression algorithm used, and this may be chosen as a trade-off between video quality and available bandwidth. 16 A reduction in bandwidth will increase transmission time, but will not reduce the video quality.
To reduce risks during realtime transmission, the operator normally stores (in the background) all of the streamed video, or has to decide which loops to store on-the-fly. In the first case, a lot of redundant information will be stored, thus making information retrieval cumbersome and slow, because only a portion of the video streaming will be clinically significant. In the second case, the decision about which loops to store on the fly will slow down the diagnostic process and the teleconsultation. On the other hand, in store and forward tele-echocardiography only the clinically significant images will be transmitted and then archived. This greatly reduces the load on the transmission bandwidth, and helps to focus the attention of the cardiologist on the diagnostic content of the transmitted examination, also speeding up the whole teleconsultation process. Long scan sweeps (especially useful in paediatric and adult congenital cases) can still be performed in the narrow-bandwidth environment, because high-compression codecs are used. Finally, the cardiologist has the possibility of suggesting corrections to image acquisitions, because highly compressed video clips are available remotely in near real-time (i.e. with minor time delay) even when using a low bandwidth. In this setting, the delay between image acquisition-transmission and availability on the monitor of the consultant cardiologist can be precisely predicted by adjusting the degree of image compression to the available bandwidth. In the present study the compression ratio was set at approximately 1:250, and we have previously demonstrated that a wide range of image compression ratios – up to 1:500 – with different codecs are available for clinical use without significant loss of image quality. 16
Feasibility of low-bandwidth teleconsultation
The feasibility of the tele-echocardiographic consultations was 100% in all the 95 patients for which they were requested, and all the video clips acquired during the echocardiography examinations were successfully transmitted. The acquisition and transmission of the video clips did not increase the time needed to complete the echocardiograms, because the tele-echocardiography workflow was embedded within the echocardiographic examination. Furthermore, the workflow of our store and forward teleconsultation modality resembled videoconferencing teleconsultation modalities, because it allowed near real-time remote visualization of a sequence of video-clips.
Imaging adequacy and clinical utility
Although imaging adequacy could not be evaluated during urgent teleconsultations, because of the continuous on-line interaction between the geriatrician-operator and the cardiologist, adequacy was considered good in all the pre-programmed teleconsultations, where the cardiologist never requested additional scanning. The high image adequacy (100%) was explained by the fact that the geriatrician-operator had previously been trained by the cardiologist, and by the consideration that the store and forward protocol used maintained the original image quality (see above) even during transitory reductions in bandwidth. Furthermore, image compression did not appear to cause a significant reduction of video quality, as assessed by an independent blinded observer.
The echocardiographic characteristics of the urgent near real-time teleconsultations did not differ from the pre-programmed examinations with respect to LV systolic function, systolic pulmonary pressure and presence of pericardial effusion. A possible explanation is that the echocardiograms were not requested by a cardiologist, i.e. they were not always appropriate (Table 3); this was also consistent with the observation that half of the examinations requested for heart murmurs or evaluation of LV function were not useful (Figure 2). On the other hand, a higher frequency of analysis of LV diastolic function in the urgent examinations was related to the investigation of patient dyspnoea, especially when LV systolic function was normal.
We found an 83% clinical utility for the tele-echocardiographic consultations, which was evenly distributed across all patient diagnoses (Figure 3). This result was higher than that found (60%) by our group in a previous study of routine outpatient transthoracic echocardiography in a tertiary care referral centre in the same geographical area (metropolitan area of Milan). 19 This difference could be explained both by the different clinical settings and referral patterns of the two studies (specific clinical indications in geriatric care versus an outpatient clinic), and by the fact that the utility of the teleconsultation was defined in the present study by a change in patient management based on the additional information provided by the consultant cardiologist. An 83% utility is clinically meaningful, thus supporting the use of a teleconsultation strategy, in particular when a low cost tele-echocardiography system is employed.
The two factors which were significantly associated with clinical utility were, not unexpectedly, a low LV ejection fraction and the examination indication. In the latter case, all indications led to a clinically useful tele-consultation with the exception of half of the examinations requested for heart murmurs and evaluation of LV function. Although all echocardiographic consultations could have been considered useful, in the sense that the diagnoses made by the geriatrician were confirmed, modified or rejected by an expert cardiologist, we preferred a slightly more restrictive definition of clinical utility based on a change in clinical management brought about by the echocardiographic findings.
Limitations
We did not perform a blinded comparison of the video clips stored in the ultrasound equipment (low compression) with the transmitted MPEG-4 video clips (high compression), because a multi-centre clinical validation of the compression algorithm used in this study has been recently published by our group. 16 Although a cost analysis comparing the tele-echocardiography consultation strategy with that of an on site cardiologist was not included in our study, the economic advantages of the former strategy appear obvious.
We conducted our study in a specific clinical setting (a geriatric care and rehabilitation institute). Although the technical protocol we employed – image acquisition, compression and low-bandwidth transmission – was independent of the clinical location, its clinical utility was not. Thus our results may not be generalizable to other clinical settings (paediatric, primary care or emergency first aid teleconsultations).
Conclusions
Our results suggest that store-and-forward tele-echocardiography using MPEG-4 video compression is a feasible, adequate and clinically useful tool for telemedicine, and has the potential for widespread use where telecommunications are scarce or expensive. The demonstrated clinical utility of the low cost tele-consultation modality has the potential to substantially reduce the time to diagnosis, as if the specialist were available on-site.