
Abstract
We conducted a mixed-methods case study to explore the perceptions of family caregivers and palliative cancer patients of home telehealth, and their experience with it. The intervention in the randomized controlled trial from which study participants were selected consisted of specialist nurses available 24 hours per day who communicated with patients and families using videophones, with optional remote monitoring. Qualitative data were collected from interviews with five patient/caregiver dyads and seven bereaved family caregivers, direct observation and nursing documentation. Quantitative data were collected from computerized nursing documentation and analyzed for patterns of use. During the study there were 255 contacts, including videophone, telephone or face-to-face visits, between tele-nurses and families. Overall the patients, family caregivers and tele-nurses felt that home telehealth enabled family caregiving, citing increased access to care, and patient and family caregiver reassurance. Pain management was the most common reason for initiating contact with the nurse, followed by emotional support. Concerns included lack of integration of services, inappropriate timing of the intervention and technical problems. The case study confirmed the importance of timely and accessible care for a group of clinically vulnerable, dying cancer patients and their family caregivers.
Introduction
The literature suggests that home telehealth may be helpful for caregivers of patients with chronic conditions, 1,2 newly diagnosed paediatric oncology patients and their families, 3 and palliative patients 4–8 and their family caregivers. 9,10 The purpose of the present study was to explore family caregivers and palliative cancer patients' patterns of use, perceptions of, and experiences with home telehealth. The research question was: what are family caregiver and palliative cancer patients' patterns of use, perceptions of, and experiences with home telehealth?
Methods
An exploratory case study was carried out, as part of a larger randomized controlled trial, the Telehomecare In Palliation Study (TIPS). The randomized trial took place in the community based palliative care service of a large teaching hospital between October 2004 and April 2006. Registered Nurses with expertise in palliative care communicated with patients and family caregivers via telephone or videophone 11 as required (referred to as tele-nurses). They could also use devices for remote monitoring of blood pressure, blood oxygen levels, and heart, lung and abdominal sounds. If care needs could not be met remotely, the tele-nurses provided face-to-face visits or referred to community nurses.
In the present study, a mixed methods approach was employed, emphasising qualitative methods. Multiple patient/family caregiver sub-units were embedded within the case and included health care professionals working in the randomized trial. The study was approved by the appropriate ethics committees.
Participants were selected from palliative oncology patients, their primary family caregivers, and multidisciplinary healthcare professionals who had been exposed to home telehealth in the randomized trial. Maximum variation sampling was employed to identify a sample of multidisciplinary health care professionals who had varying views on home telehealth (n = 14). All those approached agreed to participate in a focus group, the results of which have been reported elsewhere. 12
Data collection and analysis
Quantitative data were collected from routine computerized nursing documentation using a chart abstraction form, and analysed for patterns of use of home telehealth. A qualitative analysis was conducted on data from interviews (caregivers, patients and tele-nurses), direct observations (families engaged in video-based communication with tele-nurses) and computerized nursing documentation. All interviews were audio recorded and transcribed verbatim.
The qualitative data were coded using latent content analysis and constant comparison techniques, coding data chunks of 2–3 sentences. 13 Diagrams and tables were created to clarify codes and levels of abstraction, and emerging themes were identified. Emerging codes and themes were cited using examples from the interview transcripts to ensure clarity. Data analysis and collection were iterative and occurred simultaneously using standard software (QRS NVivo7 14 ).
Results
Telephone contact was not made with 2 of 18 eligible caregivers, despite repeated attempts. Four caregivers declined to participate in the study. Five patient/caregiver dyads and seven bereaved family caregivers agreed to a home visit (n = 17), and subsequently provided informed written consent. The types of family caregiver were: spouses (n = 7), children (n = 2), siblings (n = 1), friends (n = 2). The types of cancer diagnosed were: breast (n = 3), lung (n = 3), bowel (n = 2), prostate (n = 1), kidney (n = 1), brain (n = 1). The median patient age was 61 years (range 34–91). There were 7 male and 4 female patients. The mean length of exposure to home telehealth for the subjects in the study was 3.5 months (range 2 weeks–6 months).
Data abstracted from the documentation indicated that 255 contacts, including videophone, telephone or face-to-face visits, occurred between tele-nurses and families (Table 1). Only 10 contacts (4%) involved a face-to-face visit by a tele-nurse. Data from documentation and interviews indicated that the preferred mode of contact for families did not appear to change over time.
Patterns of use
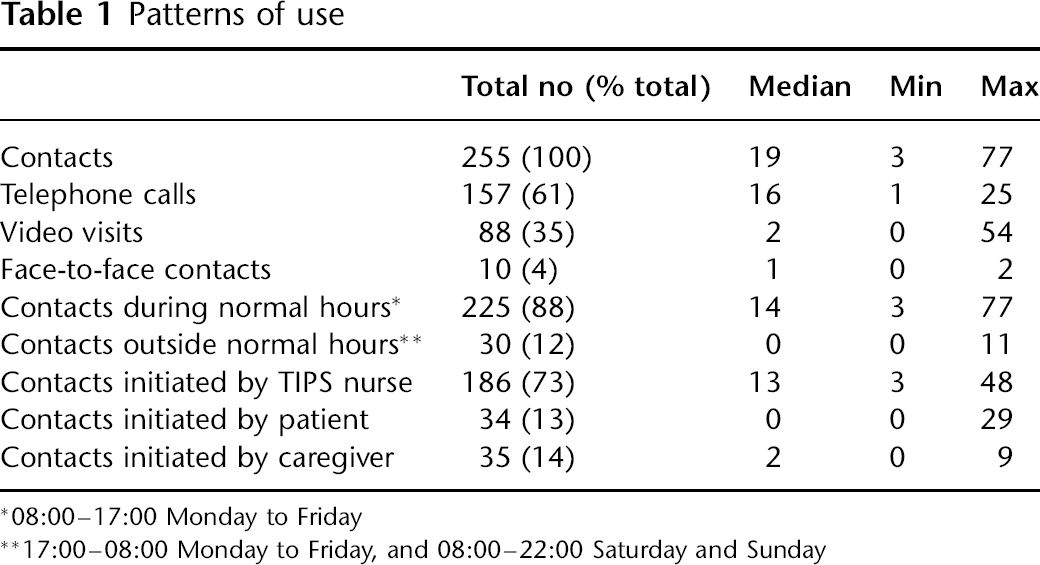
*08:00–17:00 Monday to Friday
**17:00–08:00 Monday to Friday, and 08:00–22:00 Saturday and Sunday
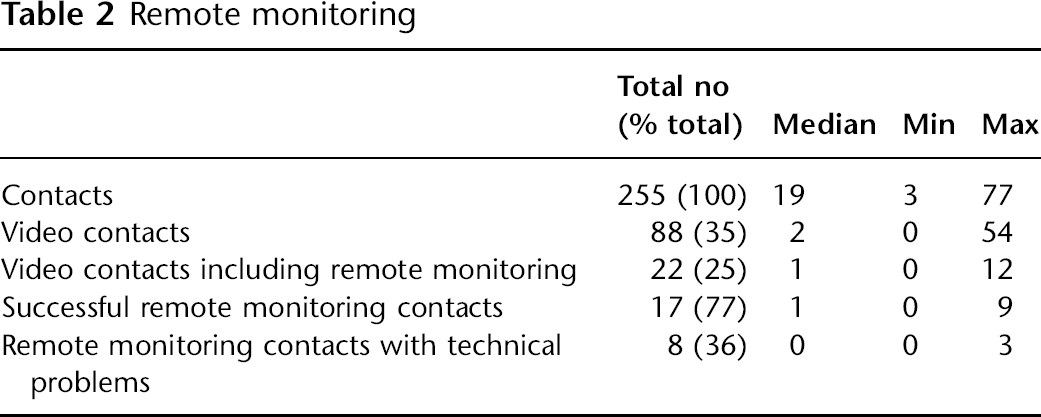
Remote monitoring was utilized in 22 (9%) of all contacts (Table 2). The views of patients and caregivers about remote monitoring varied. A few felt that remote monitoring of vital signs was very valuable. Data from the documentation indicated that four families never used, or were unsuccessful in using remote monitoring because of equipment failure.
Remote monitoring
Thematic analysis of the qualitative data showed that there were two major themes: enhanced access to care and usability of the home telehealth system.
Enhanced access to care
There were three sub-themes:
Ease of access to a health care professional
Many families stressed how important easy access to a health care
professional was. The enhanced access to a tele-nurse led to increased
reassurance felt by caregivers. Despite their appreciation of increased
access to care, it was seldom used outside normal working hours (i.e.
08:00–17:00 Monday to Friday), with only 30 (12%) visits occurring after
business hours. Data supported use by caregivers for patients whose
conditions were deteriorating, with all but one after-hours call pertaining
to pain and symptom management. Almost half of after-hours contacts were
initiated by families.
Reassurance with visual access to care
Even though there was relatively little video use, families reported that
they appreciated the visual link, explaining that it helped provide
reassurance and enhanced nursing assessment. Tele-nurses supported the value
of a video connection in providing reassurance to patients and caregivers in
particular situations. One family felt that the visual connection was not beneficial. This family
did not have a visiting community nurse involved. Furthermore, the wife did
not like her husband seeing “… the pretty girls on the screen…” This was a
source of tension for the couple concerned.
Enhanced access to pain and symptom management
Nursing notes indicated that the most common reason for tele-nursing contact
was related to pain (Table 3). It was addressed in 50 (57%) of the 88 video visits, 5 (50%)
of the 10 face-to-face visits and 62 (39%) of the 159 telephone visits. Each
contact typically addressed a number of problems.
Mode and content of visits. Values in parentheses represent the percentage of total contacts

*Includes visits relating to constipation, diarrhoea, nausea or vomiting
Usability of the home telehealth system
There were five sub-themes:
Lack of integration of nursing services
Analysis of the nursing documentation revealed that all patients, except
one, received visits from community nurses in addition to being enrolled in
the randomized trial. In some cases families had frequent visits by
community nurses and felt little need for home telehealth. One caregiver
noted confusion between the visiting and nursing services. Another caregiver
voiced similar confusion about the lack of service integration. One
tele-nurse also stressed the lack of integration of nursing services.
Inappropriate timing of the intervention
Five of 11 families felt they would have received the most benefit had home
telehealth been introduced earlier, or extended later into the patients'
disease trajectory. One caregiver said “I think it could have helped him if
we'd had [home telehealth] early on, and I think if we hadn't had access to
the other help that we had, then that would have been a real life line.”
Another caregiver also expressed frustration with the timing of the
videophone introduction stating “Although we didn't get the video telephone
until later…it wasn't operating exactly properly, but then that glitch was
figured out, but I think basically we got it, maybe too late in his
progression…?”
Lack of portability of the equipment
Lack of equipment portability was noted in many interviews, nursing notes
and during direct observation. Challenges with patients' mobility affecting
system use were echoed by a tele-nurse who observed “As patients declined,
getting up to the equipment, people were so overwhelmed. And irrespective of
how well you prepare somebody in palliative care as a caregiver, the
realities – they were a shock. So, for a lot of them to have to think of
that movement and moving the equipment or moving the person to the equipment
was just overwhelming…”
Technical challenges
Despite the general impression that the technology was relatively easy to
use, there were many examples where equipment problems occurred,
particularly with the remote monitoring devices. Problems were documented in
eight (36%) of 22 video visits using remote monitors, with 17 (77%) attempts
to transmit data eventually succeeding. Both tele-nurses commented that the
remote monitors were unreliable. One caregiver experienced problems with equipment because Digital Subscriber
Line (DSL) access was unavailable. They chose to trial a videophone
operating via the public telephone network (PSTN), but became frustrated
with the equipment and subsequently dropped out of the randomized trial.
Both tele-nurses reported experiencing technical problems with the PSTN
videophones used initially, but commented on greatly improved usability
after converting to DSL videophones.
Ease of use of the equipment
Despite technical problems with the remote monitoring, the majority of
patients, family caregivers and tele-nurses described the equipment as easy
to use overall. Direct observation supported this. All patients needed
assistance with blood pressure cuff application, but were able to operate
pulse oximeters and videophones independently.
Discussion
The case study confirmed the importance of timely and accessible care for a group of clinically vulnerable, dying cancer patients and their family caregivers. When interviewed, patients and family caregivers attested to their difficulty in obtaining care via the usual route in the community. One of the greatest advantages was the ready access they had to the tele-nurses. Appreciation of enhanced access to care via home telehealth, irrespective of its actual use, is consistent with other studies involving videophones. 15–18
Home telehealth was most heavily used during normal working hours, with nurses initiating most contacts. In the present study, only 12% of contacts occurred after hours, with families initiating almost 50% of them. All but one contact involved pain and symptom management. This may reflect the proactive approach of tele-nurses, whose easy access and reassurance may have reduced after hours contact by patients whose conditions were deteriorating.
The telephone was the primary mode of contact with tele-nurses for most families. Infrequent use of videophones as a means of contact appeared to be related to lack of equipment portability and technical challenges. It may also be that perceived benefits of videophone use were outweighed by their limitations. However, despite limited use by some families, most felt that the visual link provided reassurance. This is consistent with other research. 3,16,19
Contact related to pain management comprised 50 (57%) videophone contacts, compared with contact by telephone, in which pain management comprised 62 (39%) contacts, suggesting an important role for videophones in pain management. Videophone use primarily for pain and symptom management was also noted in a tele-hospice study using PSTN videophones in various palliative diagnoses, including cancer (61%). 4
Although nurses and families had the option of using remote monitoring devices, less than 10% of contacts included remote monitoring of blood pressure or blood oxygenation levels, and none involved the stethoscope. Lack of device use appeared to be related to technical problems, but may also have been due to the questionable role of remote monitoring of vital signs in palliative care.
Studies conducted on telephone support for family caregivers of seriously ill cancer patients, 20 patients with haemophilia and HIV/AIDS, 21 people with dementia, 22 and people with chronic illnesses receiving home care services, 23 all support telephone interventions. However, the value of commercial, dedicated videophones versus the ordinary telephone is not known. Internet videoconferencing applications, such as Skype, Google video and ooVoo, offer new possibilities.
Home telehealth was an additional community based nursing service for all but one family involved in the study, with no formal process of communication or information sharing between the tele-nurses and the visiting nurses. The lack of formal integration into standard visiting nursing services provided to community based patients was a limitation of the present study, and must be addressed in future research. 24
The lack of standardization of the home telehealth equipment, large variations between systems within which care is delivered, and differences in the populations studied make the generalization of the results in the literature difficult. 25 It is also difficult to determine the reasons for use of various home telehealth components. Considering the technical challenges experienced by families with remote monitoring equipment, and the questionable role these devices may play in palliative care, a study exploring home telehealth applications integrated into existing care delivery systems should be considered in the future, enabling a comprehensive, co-ordinated model of care delivery to support palliative patients and their caregivers in the community.