
Abstract
We examined the effect of knowledge and task specific training provided to an allied health assistant (AHA), prior to her involvement in facilitating assessments of dysphagia (swallowing disorders) via telerehabilitation. The AHA received four hours of training, which included basic theoretical information regarding dysphagia as well as hands-on training with simulated patients. A written test examining swallowing function and its evaluation was completed pre- and then immediately post-training, and then again after the 15th and 30th of 31 consecutive patient assessments. In addition, after each set of 5 clinical dysphagia assessments completed with patients following the training, two speech pathologists rated the AHA's competence in relation to performing the tasks and activities required of her during the telerehabilitation swallowing assessment. The AHA also self-rated the perceived level of confidence at these times. Before training, the assistant's knowledge of dysphagia theory was at 40%. Following training, all tests were above the 80% level. The AHA's performance was rated as competent on each evaluation post-training. The AHA also expressed overall satisfaction with the initial training provided and reported feeling confident after the initial sessions with patients. Thus for an AHA with previous clinical experience, competence and perceived comfort in providing assistance in the sessions was achieved with only a few hours of task specific training.
Introduction
Telerehabilitation, i.e. the delivery of rehabilitation services via telehealth, is an area where the involvement of general assistants as well as trained health care assistants has been found to be particularly beneficial. 1–6 Some aspects of clinical speech pathology (e.g. dysphagia management) involve hands-on interaction between the patient and the clinician. In telerehabilitation, where the clinician is located at a distance from the patients and unable to conduct such hands-on activities, another health professional, such as an Allied Health Assistant (AHA) 7 may be used to assist the patient and facilitate tasks at the patients' end under the direction of the online clinician.
There has been little discussion in the literature regarding the training, preparation or skills of AHAs assisting with speech pathology in telerehabilitation. Lalor et al. 3 used an assistant in a telehealth assessment of the speech, language and swallowing deficits of a single aphasic patient. In that study, the assistant was described as an allied health team member who facilitated aspects of the session for the online clinician and assisted with feeling and describing the movement of the patient's larynx during the swallowing assessment. Little information was provided regarding training for the assistant beyond stating that they were shown how to feel the larynx and describe the movement, nor was there any discussion of whether this training was adequate. The objective of the present study was to explore the effect of dysphagia-specific training on the knowledge, competence and perceived comfort of an experienced AHA who served as the assistant during a series of telerehabilitation assessments of dysphagia.
Methods
The study participants were one telerehabilitation assistant (the AHA), and two speech pathologists (SPs). The performance of the AHA was examined by the two SPs over the course of 31 telerehabilitation assessments of dysphagic patients. Details of the patients can be found elsewhere. 8 The study was approved by the appropriate ethics committees.
Telerehabilitation assistant
The AHA who served as the assistant in the present study was a woman who held a Technical and Further Education (TAFE) Certificate IV in Allied Health Assistance, (HLT424507) completed in 2009. She had had one year of experience working in the physiotherapy department of a large tertiary hospital in Queensland. In the health service (Queensland Health) in which this research was set, an AHA is required to hold a TAFE Certificate III or IV. The AHA in this study however, had had no formal training in dysphagia or its management.
The equipment and assessment process as well as the assistant's role in the telerehabilitation assessment of dysphagia has been described in detail previously 8 and is based on the model used in the pilot research by Sharma et al. 9 In summary, patients underwent a clinical assessment of dysphagia via telerehabilitation which was led by the online SP via videoconference. The system also allowed the online clinician to record the session and review it at a later time to confirm decisions. A Clinical Swallowing Examination proforma 8 was used to structure the session and the variables assessed for each participant. The second SP simultaneously assessed the patient via the conventional face-to-face method using the same proforma. The assistant was present for all assessments and was located in the room with the patient. The assistant's role was to help with equipment set up, facilitate appropriate positioning of the patient and assist the patient to complete assessment tasks (e.g. certain oromotor tasks; food and fluid trials) under direction from the online SP.
Assessors
The two SPs served as the assessors. Both clinicians were able to observe the AHA's ability to complete tasks during the sessions and each made an independent assessment of her performance. Neither assessor was blinded to the intent of the study. Both assessors were highly skilled in dysphagia management and had extensive experience in conducting clinical observations and assessing personnel conducting clinical tasks.
Procedure
Prior to undergoing training, a baseline test of the AHA's knowledge of dysphagia and its clinical assessment was conducted. After training, the AHA underwent periodic re-assessment of both knowledge (after every 15 patients) and practical skills (after every 5 patients) over the course of 31 successive telerehabilitation assessments, see Figure 1.

The procedure used in training the AHA for the assistant's role
The training, which involved both content learning and clinical observations, took four hours to complete. The information was supplemented with printed material about normal swallowing and the structures involved, simplified diagrams of the mechanisms of swallowing, descriptions of the disorders of swallowing and the possible causes, signs and symptoms of dysphagia, and the available treatment options for individuals with dysphagia. A video component was used to consolidate the written information. Short videos summarised positioning the patient, correct feeding techniques and tasks.
Hands-on training was also provided by using standardized patients, i.e. actors who portrayed real patients. The two SPs acted as the standardised patients. The hands-on training involved practising positioning the standardized patient and setting up for the session, including starting the telerehabilitation system; placement of the marker tape across the patient's thyroid notch; and placement of the lapel microphone and pulse oximeter on the patient. There was also training for the AHA about how to assist a patient to perform tasks during the oromotor assessment and how to rate oral musculature strength (Figures 2 and 3). The AHA received training about the 5-point severity scale 8 (from 1 = normal function and task performance within normal limits to 5 = severe impairment) used to score patient function and practised relaying this information clearly to the online clinician for their consideration. The AHA was also shown demonstrations and allowed to practice feeding the patient under instruction of the telerehabilitation SP (Figure 4) as in the protocol previously described. 9

The assistant demonstrating the correct placement of the strip of white tape on the thyroid notch of the patient. The Figure also shows the assistant rating the patient's jaw strength to relay to the telerehabilitation speech pathologist

The assistant demonstrating the assessment of tongue strength in the oromotor and laryngeal function examination of the Clinical Swallowing Examination protocol as the patient pushes his tongue against his inner cheek

The assistant demonstrating the correct method of feeding the patient on instruction from the telerehabilitation speech pathologist
Test of knowledge
Specific knowledge of dysphagia was assessed using a 15-min written test comprising 35 items with multiple question types. The test assessed the assistant's prior knowledge of dysphagia. Section one of the test comprised five open-ended questions regarding the signs/symptoms and causes of dysphagia, the role of the SP in dysphagia assessment and management and how dysphagia is managed. Section two consisted of ten multiple choice questions regarding basic dysphagia knowledge. In section three, there were eight true/false questions regarding feeding and positioning the patient for the swallowing assessment. The final section required labelling of 12 anatomical structures that are associated with swallowing function. The assistant completed the written test immediately prior to training. The same test was then re-administered on three further occasions, i.e. immediately after the training and then after the 15th and 30th patients. A level of 80% accuracy was set as the minimum acceptable standard. To minimise a test learning effect, the assistant was not provided with a copy of the test to review the answers, nor was she given the exact results of the tests other than to know if the minimum 80% set pass mark had been reached.
Competency ratings
The two assessors carried out 20-30 min semi-structured interviews with the assistant after every five patients (total of six evaluations) to discuss the assistant's competence in performing tasks during the assessments and overall performance to that point. The discussions addressed problems, provided feedback on the assistant's performance and also provided the opportunity to express any concerns regarding patient management. Based on these discussions and the observed performance of the assistant over five clinical swallowing assessments, a rating was given by each SP that related to competence/skill in performing tasks and overall session performance. The ratings were dichotomous and indicated whether the assistant was perceived to be competent or not competent in performing tasks as required/instructed by the online clinician.
During these feedback sessions, the assistant also provided a self rating of her performance. The AHA was asked to reflect on her own perceived levels of comfort in carrying out the tasks during the telerehabilitation sessions and her interactions with the patients, and to provide a rating that reflected her overall perception of her performance over the last five assessments. This was rated by the AHA using a visual analogue scale (VAS) of 10 cm in length (from 0 = not comfortable performing the tasks during the assessment to 10 = very comfortable performing the tasks during the assessment).
Results
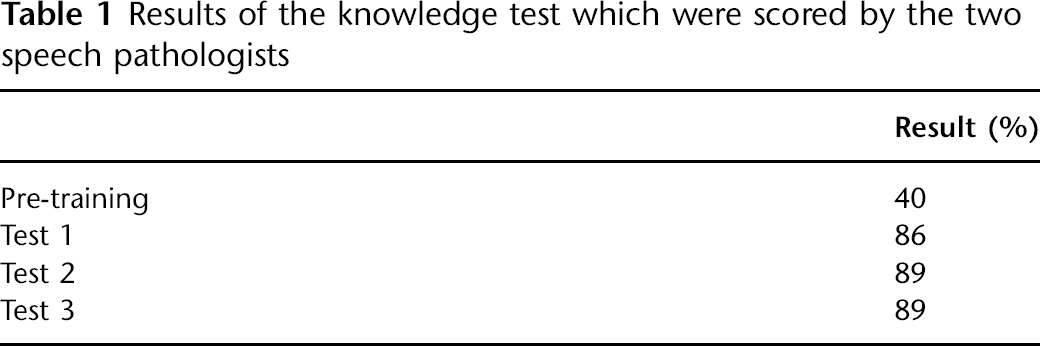
Before training, the assistant's knowledge of dysphagia was at 40% (14/35). However, following training all tests were above the minimum set level of 80% (Table 1). Items which continued to be marked incorrectly (Test point 2 and Test point 3) related to errors in labelling anatomical structures such as the oesophagus, trachea, pharynx, epiglottis and salivary gland.
Results of the knowledge test which were scored by the two speech pathologists
The assistant's competence and overall performance as judged by the assessors showed that she was competent in carrying out the specific tasks required of her position immediately following the first five patient trials. The assistant was rated by both SPs as being competent throughout the remaining five evaluations.
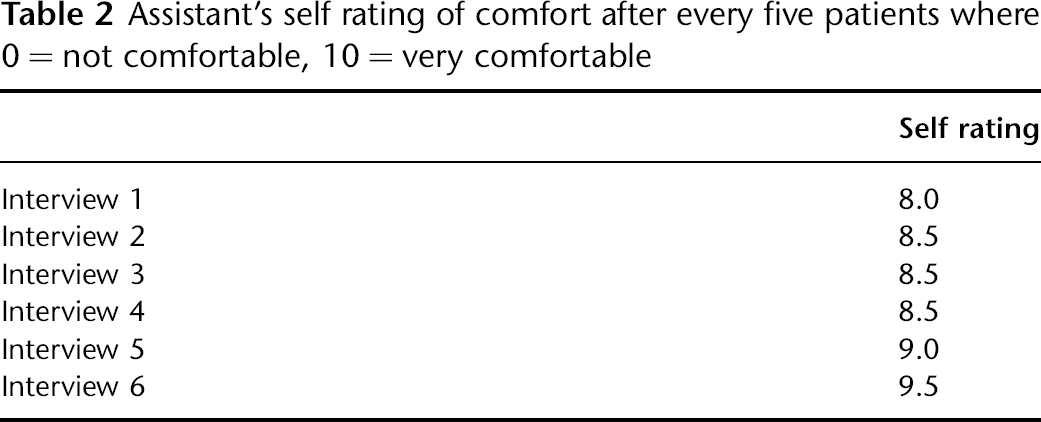
The assistant's self rating of comfort was found to be high (8/10) after completing the first five patients. This level of perceived comfort and ability to perform the session tasks continued to be high throughout the following five re-tests, with further increases in comfort levels noted at the 5th and 6th tests (Table 2).
Assistant's self rating of comfort after every five patients where 0 = not comfortable, 10 = very comfortable
Discussion
The present study indicates that the assistant's knowledge regarding dysphagia doubled after completion of the training session; she was rated as competent after the first five patients assessed, and her own perceived level of comfort in performing the session tasks and managing patients was high. This suggests that the four hours of didactic and hands-on training was sufficient for the successful completion of the clinical telerehabilitation trials. In no telerehabilitation assessment was any significant difficulty experienced, and all patients were successfully managed.
Because the assistant's background and work experience as an AHA was not in speech pathology, but in a related field, the low initial score on the knowledge test was not unexpected. However the marked improvement in the knowledge between the pre and post training tests indicated that training was successful in improving the AHA's awareness of specific knowledge relating to the tasks she was required to perform. It is recognised though, that the changes in knowledge scores observed may have been influenced in part by a test re-test bias. The knowledge component in the written test was repeated three times within a period of 25 weeks, and only contained a limited number of questions. However, as the test examined knowledge central to the job required of the AHA in the telerehabilitation assessment, any additional learning effect created by re-testing the same items was not necessarily a negative outcome. In the future, problems of test re-test bias could be minimised by having multiple versions of the same test, where each version examines similar content areas but the question wording, format and order of presentation are different.
Competence in carrying out the specific tasks during the clinical telerehabilitation assessment sessions was also achieved rapidly post training. Davies and van der Gaag 10 emphasized the importance of including both observations and video recordings of the clinical sessions for the training of assistants for specific skills. The multimodal nature of the present training programme, in which key theory training was supplemented with video and hands on practical skill training was potentially important in the positive outcomes achieved. However it is acknowledged that training alone does not ensure clinical competence. 11 In the present study, it was observed that both competence and comfort in performing the required tasks was high after only the first few patients. While this finding may be partly attributed to training, it is possible that the prior years of clinical experience, and the positive attitude of the AHA may have contributed to this result. The present training model assumed that the assistant had basic patient skills derived from her previous work experience as an AHA. Whether or not the same level of training would achieve the same positive outcomes for a novice AHA or individuals without any experience with healthcare cannot be determined from the present study. As the use of telerehabilitation in the assessment of dysphagia may be implemented in a range of clinical and home care settings in the future, further research is needed to examine the training needs of assistants who do not have prior health care experience, such as caregivers or family members.
Conclusion
The introduction of a new mode of delivery of healthcare, such as telerehabilitation, is undoubtedly complex and involves not only forming a new model of care but also the formation of new professional roles, such as that of the telerehabilitation assistant. Such new roles need careful consideration and adequate training in the breadth, depth and complexity of the skills needed to provide safe and competent practice. It is also critical that the role of the assistant is clearly defined to ensure that all required activities fall within the capabilities and permitted scope of practice of the person providing the assistance. The present study showed that for an AHA with previous clinical experience, competence and perceived comfort in providing assistance in the sessions was achieved with only a few hours of training. However further research is needed to explore the training needs of people with no prior experience working with patients. Future research is needed to determine the core knowledge and skills required to practise as a telerehabilitation assistant. Educational programmes are needed which incorporate theoretical and practical skills training to ensure the necessary competency levels are achieved.
Footnotes
Acknowledgements
We are grateful for funding from the Royal Brisbane and Women's Hospital Research Foundation.