
Abstract
We evaluated an electronic reminder device for detecting non-adherence in elderly patients with complex medication regimens. Randomly selected, home-living elderly patients were studied. The patients were aged over 65 years and were taking more than four drugs. Patients received an electronic reminder device which contained a GSM communications module. They were visited three times over a one-year period by a nurse who counted their medicine supply. We compared the adherence measured by the electronic device with the actual adherence measured by the pill count. Almost half of the 315 patients dropped out of the study for various reasons, so the calculations were performed on 168 patients. The adherence measured by the electronic reminder system was 79% and was 92% measured by pill count (P<0.0001). The limits of agreement estimated by a Bland-Altman analysis were −57 to +30. We also compared electronically measured adherence at morning/evening intake times with pill count adherence in the morning/evening only. For the pill count, there was almost no difference between morning and evening adherence rates (93%). For electronic measurement, adherence rates were lower in the evening (75%) than in the morning (81%). Electronic reminders were less reliable than the pill count in measuring adherence. However, the electronic system may be a useful supplement to other, more time consuming methods for measuring adherence.
Introduction
Interventions to improve non-adherence in patients undergoing long-term treatment for chronic diseases are not very effective 1 and the identification of non-adherence in medication regimens remains a challenge in health care research. Numerous methods for assessing non-adherence to medication regimens have been studied, but none of them measure non-adherence satisfactorily. 2 Hence, a reliable and low-cost method for detecting non-adherence in clinical settings is still required. Low-technology aids like pill boxes, dose dispensers or reminder clocks have been used for many years to enhance medication adherence, and more recently mobile phones have become popular as electronic pill-reminders. 3 In the past decade, electronic monitoring systems have become increasingly popular as a means for detecting non-adherence 4 and they are considered among the most promising methods for this purpose. 5–7 In most studies, these devices have been used to assess non-adherence in patients who were usually younger than 65 years and had a single ailment like HIV, asthma or hypertension. 8 However, the largest group of drug consumers is elderly patients undergoing long-term treatment. Only a few studies have compared adherence measured by electronic monitoring devices with adherence measured by pill count in elderly patients. 8,9
The aim of the present study was to evaluate an electronic reminder device for detection of non-adherence in elderly patients undergoing treatment with complex medication regimens.
Methods
Potential participants were identified from the National Health Insurance Population Register. From this register, samples of individuals were randomly drawn in the period February 2008 to March 2009. Duplicates were avoided by using the Danish personal identification number from the Civil Registration System. The people identified were contacted by letter followed by a telephone call. The inclusion criteria were: age 65 years or older, living at home, residence in the municipality of Aarhus, and an intake of more than four different drugs per day. Non-oral drugs were excluded.
We excluded people with the following characteristics: residence in a nursing home, hospitalization, terminal illness, cognitive disorders like dementia, and medication supervision by health care providers. A large proportion of the target group was not interested in participating in the study. Thus, 24% did not respond to the invitation and 43% of those contacted declined the invitation to participate. The study was approved by the appropriate ethics committee.
The patients received an electronic reminder system called Telesvar (TS)
10
(CIM Mobility, Struer, Denmark). The TS is portable and approximately the same size as a smartphone (Figure 1). It contains a GSM module for communication and so it was possible for patients to take the TS with them on vacation trips. Patients confirmed their medicine intake by pushing a button at self-stated intake-times. If a patient forgot to confirm their medicine intake, the TS sent a reminder signal. A reminder signal was sent at the stated intake time and if necessary again after 30 min.
Electronic reminder device. The patient was considered to be adherent when pushing the button at least one hour before or after the stated drug-intake time. The TS reminded the participant about their drug intake by an audio beep signal and red LED light in the button
The TS device works like a mobile phone and uses text messaging (SMS) to receive and send short messages to/from a server. The individual intake times of each patient are saved on the server. As soon as a patient forgets to confirm his or her medicine intake, the server sends a numerical code by a text message to the TS device and this activates the reminder signal. If the patient confirms the medicine intake by a push on the button within the stated intake time, the server receives a numerical text message and records the precise time the signal was sent to the server. In this case no activation signal is sent from the server to the TS device.
The pill count was performed by four nurses for all patients at three home visits (at baseline, 6 months and 12 months). During the home visit, each drug was noted with its name, the daily dosage and pill-taking time. The pills were photographed on a black metal tray and counted on the print in the laboratory. The main purpose of the pill count visit after 6 months was to ascertain if any changes in doses had been made. The daily consumption of pills was recorded as the Patients’ Daily Dosage (PDD). The quantity of each drug counted at the first visit was added to the total quantity of the drug bought during the study period, and the quantity of the drug at the last visit was subtracted from the total. This was then divided by the calculated quantity of the drug expected to be consumed during the study period. The procedure for the pill count has been described in detail previously. 11
Adherence
The adherence for each drug was calculated as the number of pills actually consumed (measured by the pill count) divided by the total number of pills expected to be consumed in the study period. Since all participants were undergoing treatment with multiple drugs and each drug had its own adherence, the participants’ overall adherence was calculated as the mean of all the drugs the participant used.
Drug adherence measured by TS was expressed as a percentage, i.e. the number of responses at the correct time divided by the total number of expected responses. A response was considered to be given correctly when the participant sent a confirmation of intake by pushing the button of the TS within one hour before or after the stated intake time. Non-adherence was recorded when the participant did not confirm the intake within this time window. For both methods, an adherence level of at least 80% was defined as acceptable.
Statistical analysis
We examined the overall drug adherence estimated by the TS and compared it to the pill count. We also analysed adherence rates estimated by the TS and compared them with the pill count in subgroups according to age, gender and frequency of drug intake. In a second analysis, we compared adherence estimated by the TS at morning intake times with drug adherence estimated by the pill count for drugs taken only in the morning. The same procedure was applied to the evening regimen. Finally, we analysed the change in adherence measured by the TS during the study period. The time of delay was recorded in minutes before and after the intake time window and estimated for three month periods.
The adherence estimate measured by the TS was compared with the adherence estimate measured by the pill count using a Wilcoxon sign-rank test. Adherence with medicine intake was evaluated using contingency table analyses.
Statistical analyses were carried out using standard software (STATA/SE version 11.1).
Results
A total of 315 patients were included in the study, of whom 87 were excluded consecutively at the beginning of the project because of technical problems with the TS device. A total of 54 patients withdrew for various reasons: for four patients prescription-refill data for parts of the observation period were not available and two patients died during the study period. The calculations were performed on a total of 168 patients who completed the whole study period. There were no differences in demographic characteristics between patients who dropped out of the study and patients who completed it.
Total adherence
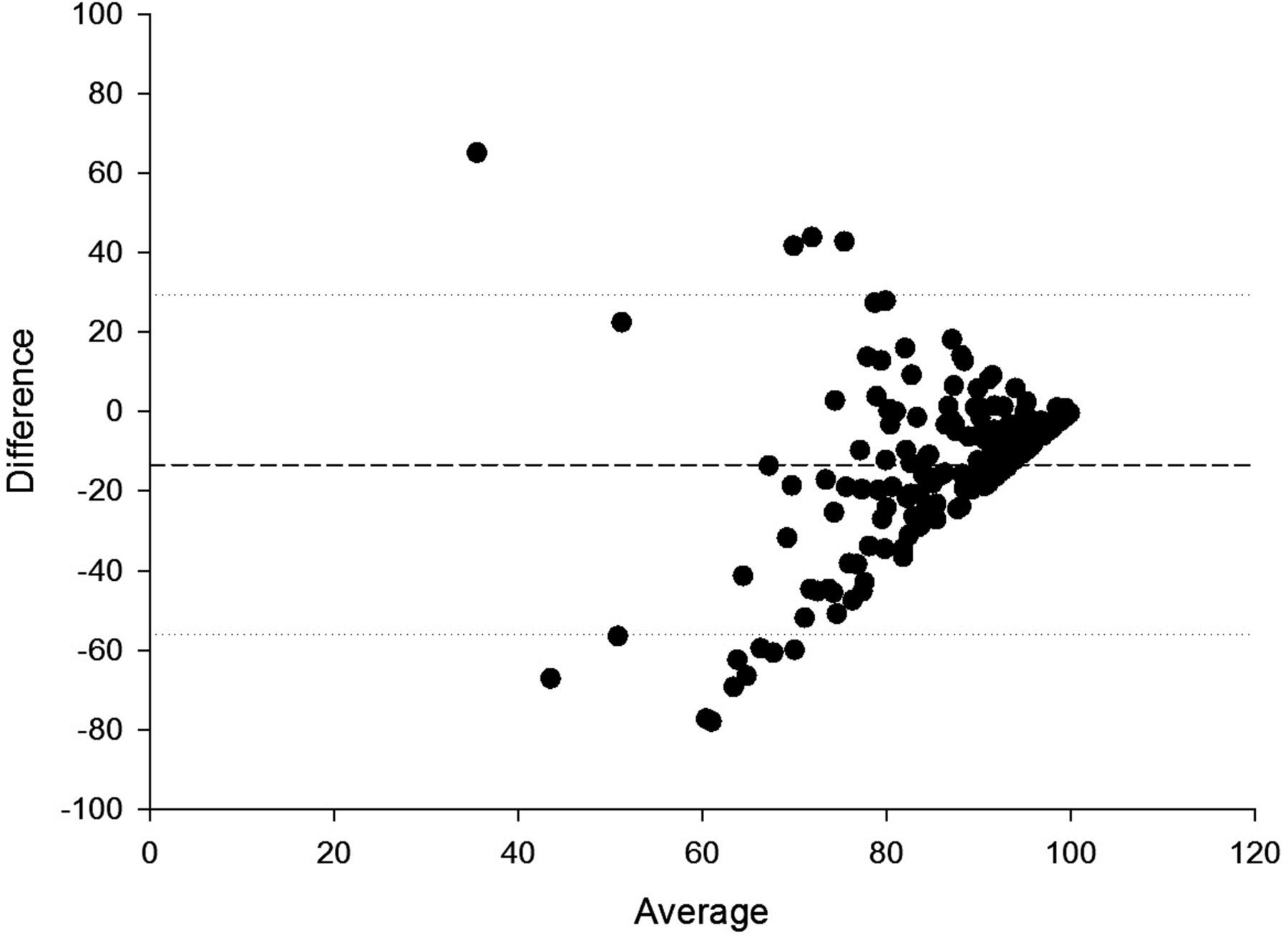
There was a significant difference in overall adherence between the two methods (TS 79%, pill count 92%; P<0.0001), see Figure 2. All subgroups tested showed the same significant differences in adherence between the two methods. The Pearson chi-square test revealed a significant association between the two measuring methods (P<0.0001). The Bland-Altman plot is shown in Figure 3 (mean difference −13.4; limits of agreement 30.2 to −57.0).
Relation between pill count and TS. Satisfactory adherence was defined as being above 79%. (A) Adherent by both methods, (B) non-adherent by both methods, (C) adherent by pill count alone, (D) adherent by TS alone
8
Bland-Altman plot of the adherence (%) estimated by pill count and TS. The limits of agreement are shown (mean, dashed; 95% confidence interval dotted)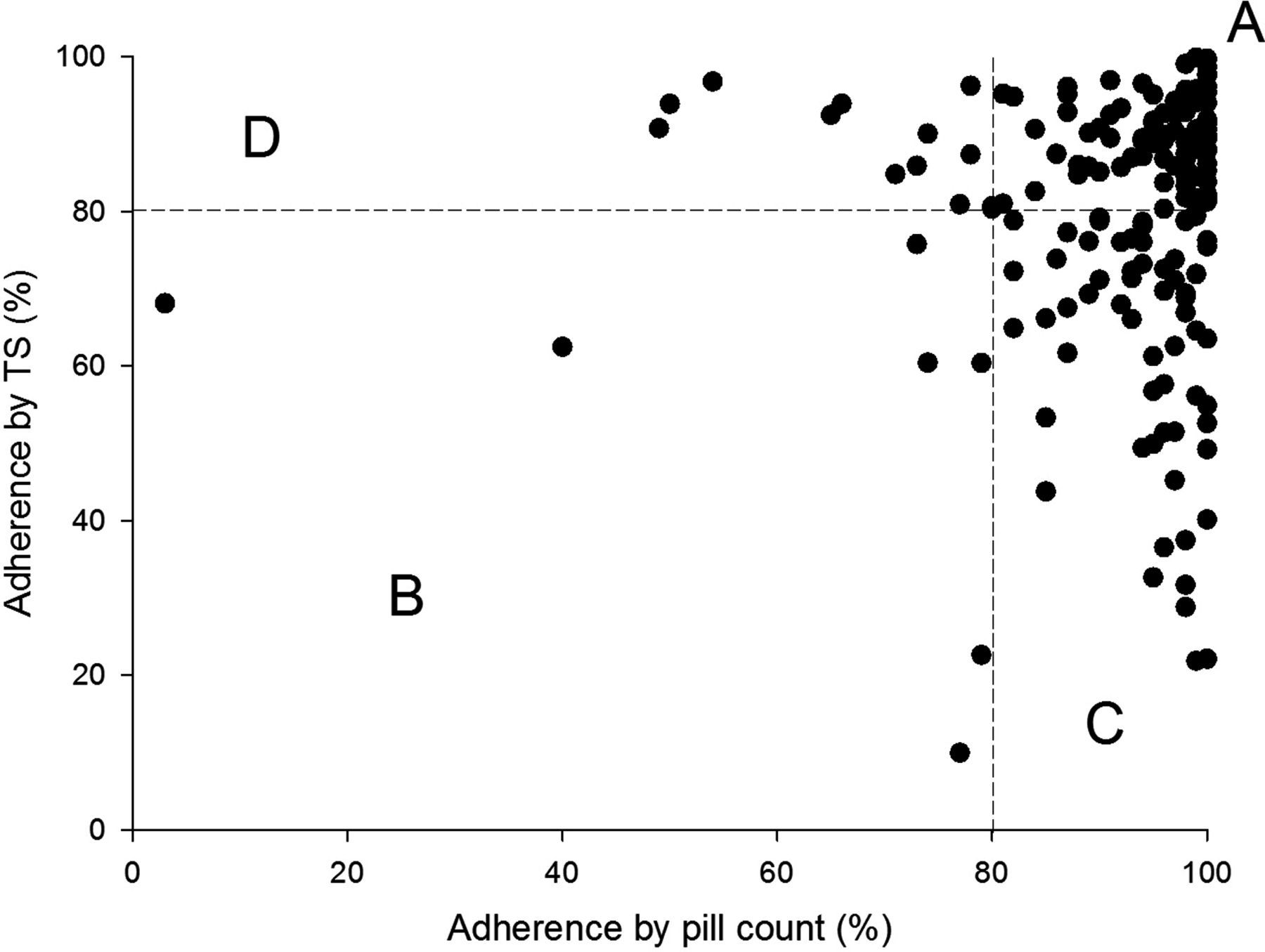
Adherence by pill count and by electronic monitoring
*P-value for the difference between pill count and electronic monitoring
Adherence at particular intake times
Adherence measured by pill count and by TS
Changes in adherence during the study
Percentage of patients (n = 168) responding before or after the self-stated intake time. Most of the patients confirmed drug intake close to the intake time, but usually after the TS had sent a reminder signal. In total, one-third of the patients confirmed drug intake before the self-stated intake time
Discussion
We found that a newly developed electronic reminder system over-estimated non-adherence, compared to the pill count. The limits of agreement estimated by a Bland-Altman analysis were 30.2 to -57.0, indicating substantial differences between the two methods. These observations are in accordance with other studies in which electronic monitoring devices consistently indicate poorer adherence. 7–9 Electronic devices are widely used for measuring adherence without taking into account that they assume, but do not confirm, that the medication intake has actually taken place. 4 The use of the device is an additional task that must be accomplished by the patient, which means that what is measured is the extent to which the device is used rather than the actual adherence to the medication regimen itself. This fact has been largely overlooked in previous studies. 5,7,8,12
In the present study, the TS was evaluated at both patient level and drug level. Patient level analysis showed that patients aged 76–99 years were more adherent (82%) in confirming their drug intake via the TS than patients aged 65–75 years (76%). Our results imply that electronic reminder systems like the TS may be beneficial in improving adherence in the oldest patients. Analysis of the number of drug intakes showed that the TS did not identify adherence properly when patients had to confirm their drug intake more than three times per day (72%). Further studies are needed to evaluate the influence of the number of daily drug intake times on the reliability of electronic non-adherence detection.
The morning/evening analyses were based on drug level, where morning (evening) response was compared with the corresponding scheduled morning (evening) drug consumption. The TS adherence for evening intake was low (75%) compared to morning intake (81%). The pill count identified almost no difference between morning and evening medication adherence (93%) suggesting that electronic reminders like the TS that involve the patients’ active confirmation are not suited for monitoring more complex medication regimens with evening medicine intakes. In contrast, the fact that the pill count identified almost no difference in morning and evening medication adherence (93%) may imply that the pill count is not suitable for detecting whether the daily regimen is being followed or not. The pill count would not detect compensation of drug intake in the morning for frequent forgetfulness in the evening. On the contrary the TS is better suited to differentiate between morning and evening intakes. In our study, it was not possible to confirm or refute this assumption.
Electronic devices may, however, improve our understanding of patients’ habits and routines and may provide information on daily intake and drug-taking behaviour. 13 In the present study, patients did not change their habits or routines of pushing the response button over a period of one year. Most of the patients confirmed their drug intake 0–15 min after the electronic device had reminded them by an audio beep and an LED light signal on drug intake (44%). One-third of the patients confirmed their drug intake within one hour before the stated intake time (Table 3). A possible explanation for the absence of any change in habits over time is that our study population already showed a high level of adherence before the study started and needed no electronic devices to support their drug intake.
The high level of adherence of the study population (92% measured by the gold standard, the pill count) weakened the power of the study and made comparisons difficult. The exclusion of 87 patients at the beginning of the study and the high number of non-responders at inclusion may have introduced a selection bias and contributed to the high level of adherence of the group. The Hawthorne effect is another possible explanation.
Electronic devices like the TS measure primarily the adherence to the device which is a proxy for, but not identical with, adherence to medicine intake times. In contrast, the pill count measures primarily the adherence to actually taking the medication and secondarily the adherence to intake times. However, adherence estimates from an electronic monitoring device can be useful as an adjunct to the pill count. 8,9
Conclusion
Electronic monitoring systems are less suitable for measuring patients’ adherence than the pill count. An electronic device primarily captures patients’ adherence to the device, which may or may not be a good estimate of the actual drug intake. Furthermore the signal sent by an electronic device does not always correspond to actual drug intake. In the present study, confirmation of evening intake differed from the drug intake estimated by pill count. Electronic monitoring devices may be useful to disclose the patterns of adherence behaviour. Electronic reminders may also be beneficial when the problem of non-adherence is caused by forgetfulness.
Footnotes
Acknowledgements
The study was supported by the Danish Ministry of Health [2007–13009–501], the Association of Danish Pharmacies [HPN/161/00011], the Toyota Foundation and the Health Insurance Foundation (Helsefonden) [2009B038].