
Abstract
Seven long-running telemedicine networks were surveyed. The networks provided humanitarian services (clinical and educational) in developing countries, and had been in operation for periods of 5–15 years. The number of experts serving each network ranged from 15 to 513. The smallest network had a total of 10 requesters and the largest one had more than 500 requesters. The networks operated in nearly 60 countries. The seven networks managed a total of 1857 cases in 2011, i.e. an average of 265 cases per year per network. There was a significant growth in total activity, amounting to 100.3 cases per year during the 15 year study period. In 2011, network activity was 50–700 teleconsultations per network. There were clear differences in the patterns of activity, with some networks managing an increasing caseload, and others managing a slowly reducing caseload. The seven networks had published a total of 44 papers listed in Medline which summarized the evidence resulting from the delivery of services by telemedicine. There was a dearth of information about clinical and cost-effectiveness. Nevertheless, the services were widely appreciated by referring doctors, considered to be clinically useful, and there were indications that clinical outcomes for telemedicine patients were often improved. Despite a lack of formal evidence, the present study suggests that telemedicine can provide clinically useful services in developing countries.
Introduction
Recent reviews of e-health applications have concluded that evidence in relation to improved patient outcomes, and evidence for cost-effectiveness, is rather thin on the ground. 1,2 Applications which facilitate care at a distance, i.e. telemedicine, can have particular value in low- and middle-income countries, and telemedicine has been used for many years to support doctors in the developing world. 3 Several networks exist, which provide services in different settings and in different ways. However, there is little published evidence about the effectiveness of such networks, and – assuming that it would be desirable to do so – there is no way of deciding what the best method of expanding their activities would be.
Performance measures (from Wootton et al. 4 )
The present work forms part of a wider study in which the framework for performance evaluation was applied to a larger number of networks. Details of the study design and additional information about the experience of the networks, including governance, medical liability, patient confidentiality, sustainability factors, challenges and future plans have been published elsewhere. 5 The aim of the present report was to summarize the performance of the networks, to draw conclusions about the effectiveness of the services provided, and to make suggestions about how these might be evolved in the future.
Methods
The telemedicine networks included in the study were identified according to the following criteria:
they delivered clinical and/or educational services through telemedicine they were long-running networks, defined as those which had been in operation for five years or more they delivered humanitarian services, defined as those designed to save life and alleviate suffering, and which are delivered without condition (e.g. pro bono).
Long-running telemedicine networks delivering humanitarian services were identified by the authors based on their personal knowledge of the field. Telemedicine networks were excluded from the analysis in the case of no reply to initial enquiry.
5
Data collection
Information for the study was collected by questionnaires (in English) sent to a contact person at each telemedicine network. The first questionnaire was sent in September 2011, to collect general information about the networks, including purpose, duration of operation, activities provided, model of operation, and numbers of requesters, experts and coordinators. A second questionnaire was sent in October 2011. This was designed to collect specific data about network performance, together with other more detailed characteristics of the networks. Each questionnaire contained 20 questions. Additional short questionnaires were sent in early 2012 to obtain information about the total number of cases managed during 2011, and further information about network operation.
Effectiveness
The information provided by the networks in response to the questionnaires included the total number of scientific papers published and details of the scientific papers published in Medline. Since the best quality evidence comes from papers published in the peer-reviewed literature, the latter information was assessed for evidence of clinical- and cost-effectiveness.
Only papers listed in Medline and dealing with telemedicine services were included in the analysis. To summarize their contents, one author extracted information from each published paper on the following topics: (i) study design; (ii) clinical effectiveness; (iii) cost-effectiveness. Study design was assessed using the nine-point scale traditionally employed to measure the strength of the evidence. 6 The other topics were graded subjectively and assigned a quality score based on the amount of information provided about them. Finally, the results were reviewed by all authors and changed by consensus where necessary. Hence, the papers from each network were reviewed by researchers from all the other networks, which increased the consistency of the results.
Results
General information regarding the telemedicine networks
*ITM, Institute of Tropical Medicine, Antwerp
**RAFT, Réseau en Afrique Francophone pour la Télémédecine
Organizational models
*For telemedicine networks with a clinical purpose, there are two fundamentally different modes of operation which correspond to the different ways in which an expert is chosen to reply to a query. In the "targeted" mode of operation, a query is directed to a specific expert for reply. In the " open" or "distributed" mode, a query is directed to a group of experts, of whom all, some or none may reply 4
Network performance
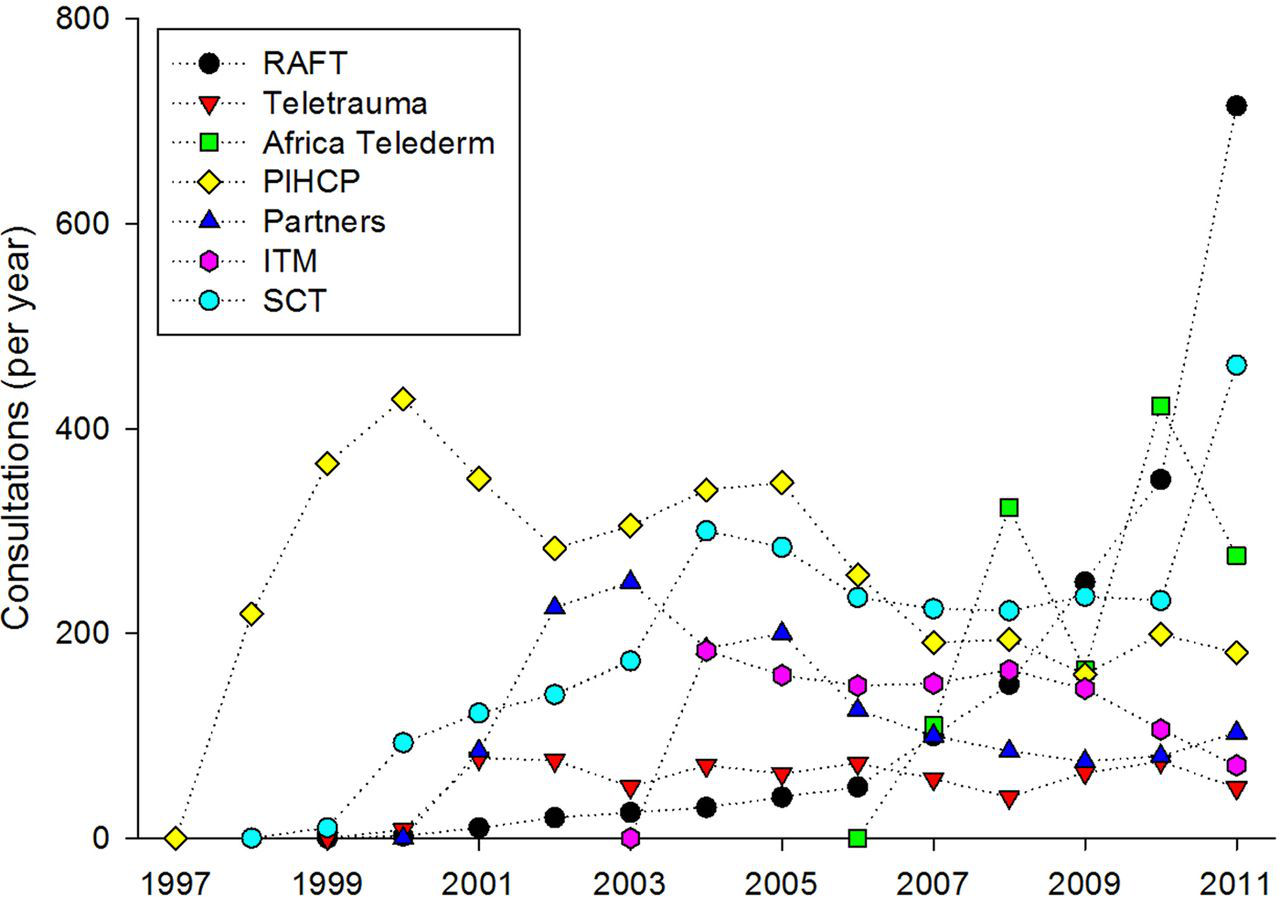
The seven networks managed a total of 1857 cases in 2011, i.e. an average of 265 cases per year per network. There was a significant growth in total activity, amounting to 100.3 cases per year during the 15 year study period (P<0.001), see Figure 1. In 2011, network activity in the individual networks ranged from about 50 to over 700 teleconsultations per year, see Figure 2. There were clear differences in the patterns of activity, with some networks managing an increasing caseload, and others managing a static or reducing caseload, see Table 4. The mean caseloads (averaged over five years) ranged from 57 to 313 cases/year.
Total caseload managed by the networks (the solid line is the linear regression). The number of networks operating each year is shown below Numbers of clinical consultations in each network Activity trend in each network for the years 2007–2011. The trend was calculated as the linear regression of each network's annual caseload on time
Little quantitative information was available for the educational activities provided by the telemedicine networks. Only the RAFT network collected data, see Figure 3. The ITM telemedicine network also offered online learning and web-based discussion forums, but the contact-hours could not be quantified.
Hours of tele-education provided by the RAFT network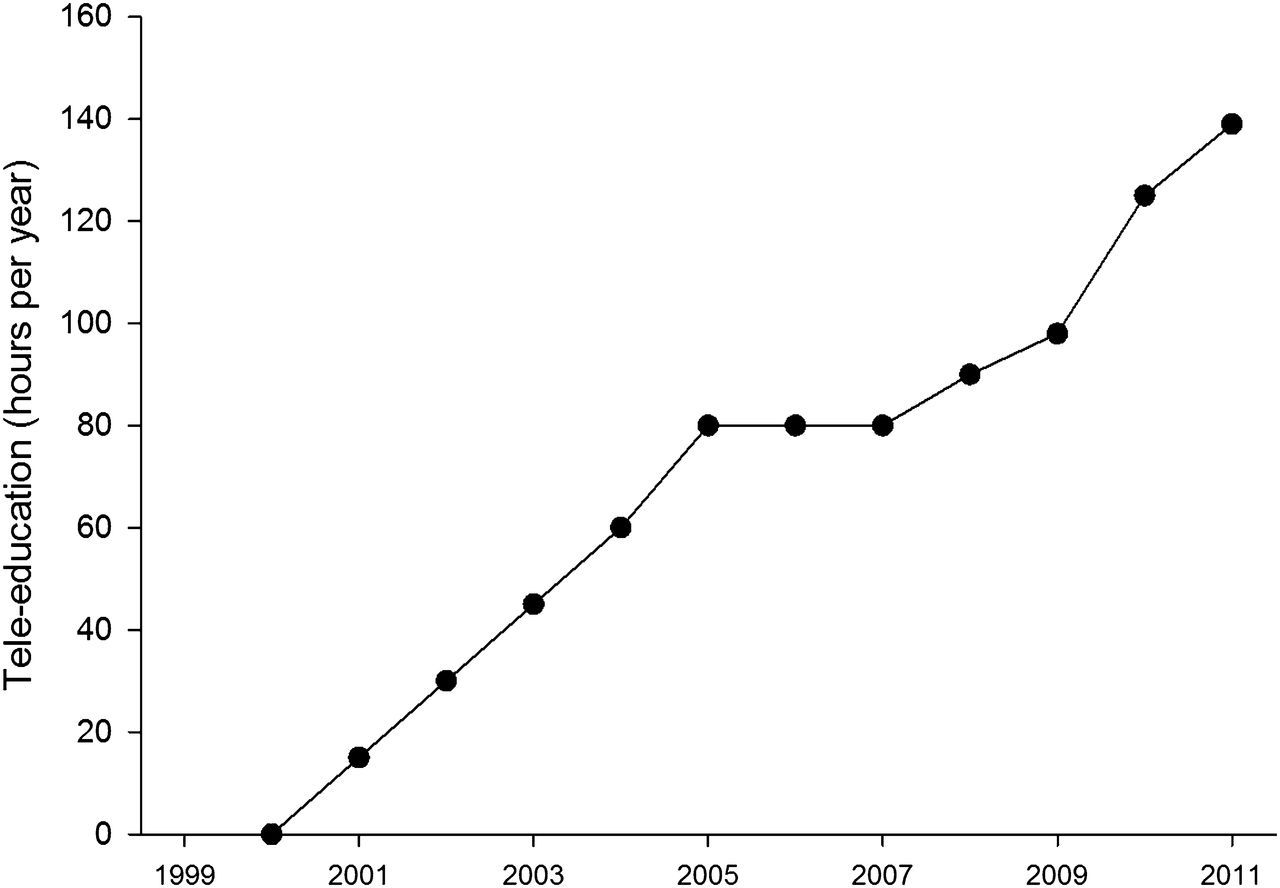
Performance of the telemedicine networks in 2010
*The possible responses to the multiple-choice question were: Never; Sometimes; Often; Always
The average time to first reply to the requests is an important performance measure which affects the value of the clinical teleconsultations to the referrer. In the previous 12 months of operation, most networks had an average time to first reply of about 24 hours (range 5.6–72 hours). Another performance measure regards the possibility, for the requesters, of conducting a dialogue with the experts. This facility was available in all seven telemedicine networks. On the other hand, the experts only sometimes had access to outcome data about individual patients. In particular, the number of times that feedback was provided on outcomes in 2010 ranged from all cases managed by the network to only a few of them.
Clinical and cost-effectiveness
Clinical and cost-effectiveness of the telemedicine networks, based on their published papers
Discussion
The present study reports the characteristics of seven long-running networks which deliver humanitarian services by telemedicine. The networks were of different sizes, used different models of operation and provided different services (although all of them provided clinical teleconsultations). The reasons why the caseload of some networks was rising while that of other networks was falling are not yet fully understood. It may be a consequence of the use of small-scale organizational models, and it might be that improved collaboration between networks in future will improve the situation. Furthermore, there was no obvious relation between the model of organization employed by the networks and their performance, see Tables 3 and 4.
Despite the differences in their organization, there were similarities in the performance of the networks: all provided rapid responses to clinical requests, and all offered the possibility of further dialogue between requester and expert. Although there had been relatively few user surveys, those that had been conducted all showed high levels of user satisfaction. 9,40 Thus, it appears that there is no single common successful organizational model. That is, different models are associated with sustainability (since the telemedicine networks had all been in operation for 5 years or more) and lead to similar performance. In future, a comparison between long-running telemedicine networks (i.e. the ones included in the present paper) and other telemedicine networks which have ceased operation, might provide a better understanding of which are the most successful organizational models.
Although all networks were able to report some of the performance data suggested in the framework, few of them had been able to obtain outcomes data routinely, and the published work contained generally weak evidence for clinical effectiveness. None of the networks had published evidence of cost-effectiveness, as would be considered normal in other areas of health care, and there were no reports which complied with current guidelines on health economics studies. On the other hand, it is worth noting that an absence of evidence for cost-effectiveness does not prove that the operations are not cost-effective. Despite the weak evidence for effectiveness, an extensive corpus of published work provided evidence that the services were widely appreciated by referring doctors, considered to be clinically useful, and there were indications that clinical outcomes for telemedicine patients were often improved.
All of the networks held concerns about long-term funding (data reported elsewhere 5 ), despite their apparent sustainability to date. Published information on cost-effectiveness would make it easier to secure funding through conventional sources, which emphasizes the importance of collecting performance data of the kind suggested in the framework. 4 Other measures which might improve sustainability include better mechanisms for cooperation between networks. 51
Limitations
The present study had certain limitations. For example, there may be other long-running telemedicine networks around the world which also deliver humanitarian services. However, we believe that the ones studied include the main active networks. Other limitations concern the study design. For example, we examined only successful networks, and arguably, experience from unsuccessful networks may be equally informative. Also, the experience of the telemedicine networks was reviewed by the persons responding on behalf of the networks. This might represent a potential reporting bias.
Conclusion
Despite a lack of formal evidence, the present study suggests that telemedicine can provide clinically useful services in developing countries. Since the potential pool of patients is very large, we suggest the right strategy at present should be one of cautious expansion. That is:
continued support for current networks; introduction of new networks, based on similar models to those employed by the networks described here; a programme of research designed to secure formal evidence of clinical- and cost-effectiveness.
Future research should aim to obtain formal evidence of clinical effectiveness, which implies the need for patient follow-up. This is not easy in the settings in which the networks operate. Future research should also aim to obtain evidence of cost-effectiveness, which is likely to require controlled trials. Again, this is not likely to be easy to do in practice. However, if convincing evidence of cost-effectiveness can be obtained, then telemedicine in the developing world could take its place alongside measures of proven effectiveness, such as vaccination, and be funded for large-scale implementation.
Footnotes
Acknowledgements
We are grateful to our colleagues in the various networks for their willingness to share the data about network operation.