
Abstract
We evaluated a commercially-available monitoring system for older people with dementia living at home. The system was designed to detect problems before they require crisis intervention. Fourteen clients from two healthcare organisations in the Netherlands used the system over a 9-month period. The formal and informal caregivers were interviewed, project group meetings were observed, nurse diaries were analysed and a cost analysis performed. Clients and informal caregivers reported enhanced feelings of safety and security as a result of having the system installed in the home. The system appeared to reduce the burden of care on the informal caregiver and had the potential to allow people to live at home for longer. There were financial savings for clients staying at home with the technology compared with the costs of staying in a nursing home: for 10 clients living at home for 2 months, the savings were 23,665 euro. The study showed that the monitoring system represents a potentially useful early warning system to detect a situation before it requires emergency intervention.
Introduction
In 2010 there were more than 35 million people worldwide living with dementia. 1 New approaches are required to meet the demands on formal and informal care systems 2 and to promote the independence and well-being of an ageing population. Assistive technologies have potential, but little is known about their effectiveness for people with dementia.3,4
The assistive system AD Life is designed to detect problems before they require emergency intervention, such as admission to hospital or institutional care. The system uses equipment installed in the home, comprising a gateway with an alarm button, and a number of sensors which register the pattern of a person's behaviour within the home. The gateway sends this information to a server through a conventional telephone line which can be accessed remotely by a formal caregiver to assist in clinical decision-making. The caregiver can contact the person with dementia or an informal caregiver (such as a friend or family member) if changes in activity occur which might indicate the need for intervention. 5
To our knowledge, there have been no previous evaluations of the ADLife system. We conducted an evaluation to address the following questions:
How was the system installed and introduced into the homes of clients and through the participating healthcare organization?
How did the formal caregivers use the system in their everyday working practices?
How did the users rate its usability?
What was the effect of the system in terms of interventions, well being and cost savings?
Methods
The evaluation focused on (1) technology uptake: usage behaviour and usability, and (2) the technology impact: improved interventions, client well-being, effect on informal caregivers and cost savings. A summative evaluation of the technology implementation and subsequent operation and maintenance was conducted as these issues can have an effect on subsequent usability and acceptability by users. 6 A mixed methods approach was used which involved interviews with informal and formal caregivers, analysis of project group meetings and diaries from two nurses who worked with the system, and a cost analysis.
A field trial was conducted in the homes of 14 elderly people with dementia from April to December 2010. The same suite of sensors was installed in each home, at similar locations in the home, although the room layouts differed. Participants were recruited from two homecare organizations in the Netherlands. One of these organisations was involved in interpreting the ADLife client data.
Study participants
Clients were included if they were receiving homecare (housekeeping, nursing, personal guidance), but were not all personally known to the formal caregiver who interpreted the data. The formal caregivers selected clients diagnosed with dementia who were expected to live at home for at least 9 months. The professional caregivers were interviewed once, at the 9 month stage, and prior to the end of the evaluation. They participated in the project group and reports of their meetings were used as data to determine their opinions of ADLife. Two nurses who worked daily with the ADLife system were interviewed and asked to keep a diary. All formal caregivers, except the technician, had no previous experience of working with sensor technologies.
Fourteen informal caregivers were interviewed at the start, after 3 and after 9 months of using the technology. These included four partners of ADLife clients (three living in the same house as the client).
Use of the system
The formal caregivers monitored the sensor data for six weeks to establish the daily activity patterns of their clients. They received training in how to read and interpret the data, which was then monitored for a duration of nine months. The formal caregiver was required to contact the client or a nominated contact person if changes in the client's activities suggested the need for intervention. An example of daily data for specific sensors is shown in Figure 1. Figure 2 and Figure 3 show examples of activity data from a single sensor.
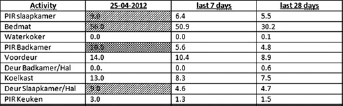
Screenshot. the red entries (identified by cross hatching) indicate a sudden deviation requiring intervention (as can be seen on 25 april 2012 for the movement sensor in the bathroom [pir badkamer]), yellow entries (identified by diagonal hatching) indicate a potentially emerging situation and green entries (identified by no hatching) denote the data being within limits

Screenshot showing daily activities at a specific time in the hallway
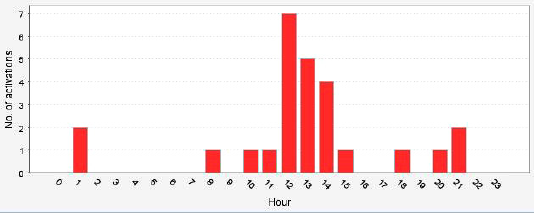
Screenshot showing the number of activities at specific times in the hallway
Interviews with informal caregivers
A total of 38 semi-structured interviews were conducted with informal caregivers; 13 were undertaken immediately prior to using the system, 11 follow-up interviews were conducted at or after the three months stage and 14 post-interviews were conducted. A semi-structured interview guide was employed which included the following topics: implementation of system, usability of the technology, effect on care intervention and effects on well being, as key dimensions defined in the CeHRes roadmap. 6 All interviews were tape recorded and transcribed for analysis purposes.
Interviews and diaries with formal caregivers
An interview at the end of the evaluation was conducted with the two nurses who worked with the ADLife system, using an adapted version of the informal caregivers interview guide that focused on the effect of technology on the working practices of caregivers. The nurses kept a diary of their usage of ADLife which was used in the evaluation and as a stimulus during the interviews to discuss specific cases.
Project group meetings
In total there were eight project meetings over a period of 14 months. In these meetings, the evaluation focused on recording information related to caregiver experiences whilst using the system. Key findings and action points from the meetings of the group were recorded by a researcher.
The interviews and project group notes were analysed thematically. 7 A second researcher coded the interviews to minimize single researcher bias.
Cost analysis
The costs of staying at home with the technology were compared with the costs of a nursing home admission from a societal perspective. The cost of living in a nursing home was the total government or health insurance expenses for someone living in a nursing home.
The cost of staying at home was:
The cost of purchase and installation of the ADLife system
The initial fee for activating the system and the monthly fee for using it
The average monthly cost for homecare paid by the state, e.g. for nurses coming to the home to help with washing and eating
The average monthly cost of the person who reads out the data from the system
The cost of the professional caregivers’ time for analysing the data.
These costs were calculated:
For 10 clients up to 150 clients
For 1 month up to 12 months of living at home or in a nursing home
For the use of ADLife at home with increasing costs of homecare.
Ethics
All participants were provided with an information sheet and signed a study consent form. For those clients who were unable to provide their consent due to dementia, their informal caregivers were asked to sign on their behalf. The study did not require ethics approval.
Results
The mean age of the clients was 78 years (range 58-87). Their MMSE scores (1 = severe dementia and 30 = no dementia) ranged from 13 to 29 with a mean of 23. The 14 participants consisted of six females and eight males. The formal caregivers were two nurses, an occupational therapist, nursing home doctor, project manager, technician and research assistant. There were eight females and six males whose ages ranged from 35-79 years. The total number of years spent caring ranged from less than 1 year to 12 years with a mean of 4.2 years.
Introduction of the system
The research findings suggested that the way in which ADLife was introduced to caregivers and users could be improved. Because the formal caregivers had no prior experience with the system, they had problems in clearly describing it during the recruitment process. Subsequently, informal caregivers had misconceptions about what the system was designed to achieve, which affected levels of acceptability. For example, two informal caregivers decided not to participate in the trial because they thought the movements of the older person were being captured through real time video images. Informal caregivers also reported problems relating to the presence of the equipment in the home environment. Some clients appeared unsettled by noises and flickering lights from the equipment, seeing these as indicators as a cause for alarm, raising levels of anxiety.
Formal caregivers commented that they felt isolated and alone when participating in the project, because other carers outside of the project group were not aware of the evaluation. Whilst it was the responsibility of the internal project manager to publicize the project internally, time constraints hindered her progress. This deprived formal caregivers of an outlet to share their experiences of being involved in the trial, resulting in the feeling that there was little organizational commitment to the project, which undermined levels of enthusiasm. Progress was also hampered by members of the project group who disengaged from the project due to sickness, retirement and lack of time, affecting the continuity of the evaluation as new participants needed to be orientated to the aims and objectives of the evaluation.
Further discussions with formal caregivers centred on the most appropriate time to install the technology in the clients’ homes. A number of the informal caregivers felt that ADLife was unnecessary, because the clients were only experiencing mild forms of dementia and did not require any intervention. However, some caregivers suggested that installing the system prior to the onset of more serious dementia was advantageous, since the client had the mental capacity to understand the purpose of the sensors and could gain proficiency in the workings of the system.
Usability
At the beginning of the evaluation, the formal caregivers experienced difficulties in reading and interpreting the client data. A technician provided extra training, which was judged positively by the nurses. However, there were also recommendations made by formal caregivers to improve the user interface, including re-designing graphs/bars for easier readability of the data and displaying long-term data to establish patterns and trends over time.
The email alerts provided to the caregivers were reported as being valuable. Given their other commitments, nurses were often only able to directly access the ADLife data twice per week, and the alerts provided an opportunity to fill the gaps between caregiver visits, allowing them to observe and monitor remotely. Formal caregivers thought it would be useful if clients informed them when fluctuations in the data could be expected, for example, leaving the house to visit friends for the day, to prevent unnecessary responses.
There were a number of operational problems which affected the reliability and accuracy of the data. The most common problem was data not being transferred, resulting in formal caregivers being unable to access information on the condition of the patient. The system sometimes generated false positives, for example, through over sensitive bed sensors or generated inaccurate readings, for example, through erroneous transmissions in the data. This created a feeling amongst formal carers that the information was unreliable, undermining their confidence in using the system as a decision-making tool.
Informal caregivers felt that the system would be more useful if it also monitored emergency situations, for example to identify a fall event, rather than simply acting as a preventative tool.
Effect of care interventions
Formal caregivers believed that the ADLife system could assist those living with dementia to remain at home for a longer period of time, as it provided the possibility for earlier, timely interventions. Two situations occurred where ADLife data prompted changes in service delivery to better support the older person. In the first situation, a person was identified from the sensor data as sleeping in his chair in front of the television instead of in his bed, prompting the informal caregivers to commence a bedtime service. In the second situation a person was identified as not using the salt dispenser, located in a closet with a door sensor, suggesting that the person was not preparing their own meals. This prompted the caregivers to implement a meal service for the client. In addition, formal caregivers mentioned that if a person could prepare their own meals and the sensors showed evidence of this, then it would be possible to discontinue the meal service.
However, the system was not failsafe. For example, there was a situation where the client did not consume any fluids for some time and became dehydrated. This developed into an emergency, but it was not recognized by the ADLife system.
Effect on well-being of the client
Informal caregivers reported that most clients became unaware of the sensors over time. They reported that the small size of the sensors ensured that they quickly became an acceptable feature of the home environment following installation. Even when awareness of the sensors was raised, the system afforded a sense of safety and security to clients, knowing that they were being monitored by the formal caregiver.
A particular concern expressed by clients and caregivers was that dementia is characterized by periods of forgetfulness which can compromise health and well-being. One of the clients often failed to remember to undertake important everyday tasks, for example taking medication or remembering to eat. Having a system which alerted caregivers to deteriorations provided the client with a perception that there was an additional security net which was continuously monitoring them. Ensuring that people are supported in their home was seen as integral to older people retaining a sense of personhood, providing a private domain to express their freedom and autonomy.
Effect on well-being of the informal caregiver
The informal caregivers reported that the ADLife system alleviated their anxieties and concerns when they were not able to undertake personal visits or make telephone calls. Caregivers reported that the system supported the tasks they carried out, freeing up their time to engage in activities and tasks that were restorative of their well-being, for example, freedom to visit friends or going for a vacation. However, it had no direct effect on supporting caregivers with the most onerous tasks, such as grocery shopping, contacting service providers and managing the clients’ finances. One of the caregivers reported that in some circumstances the system might increase the burden of care, if the sensors detected certain situations where additional care was required.
Some caregivers commented that they valued the information provided from the sensors, as it gave a better understanding of the behaviour and movements of the client. However, it also had the potential to create further interventions through the information it generated.
Other caregivers reported that the person they were caring for did not experience any situations which directly required an intervention. However, they felt that the system could be useful if the state of dementia was to deteriorate, requiring closer monitoring and more frequent intervention. For one client, the system highlighted deteriorations in health status and condition, including a disturbed sleep rhythm, which might provide a useful piece of information in determining the frequency of wandering and appropriateness for admission to a nursing home.
Cost analysis
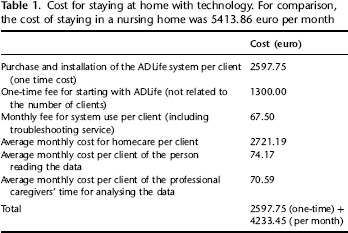
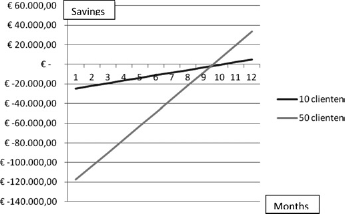
The cost analysis indicated that there were savings for clients remaining at home with technology compared with admission to a nursing home (Table 1). Compared to staying in a nursing home, for 10 clients living at home with ADLife for a duration of two months, the savings were 23,665 euro, while for 50 clients the savings were 124,122 euro (Figure 4). If the quantity of home care is to be increased (given an expected deterioration in condition as the person ages), there will eventually be a breakeven point at which a nursing home is less expensive than the private home. For example, if a client in the Netherlands receives 15 hours of homecare, four hours of housekeeping service, three hours of personal guidance and visits to a day-care centre (a total of 20 hours per week), this will result in a monthly care cost of approximately 5000 euro. Above this, a nursing home becomes cheaper. With this amount of homecare, the cost savings for 10 clients can only be reached after a duration of 10 months staying at home compared to living in a nursing home (as can be seen in Figure 5). If the homecare expenses increase above the 5000 euro per month it will be more cost effective for an older person to be admitted into a nursing home.
Cost for staying at home with technology. for comparison, the cost of staying in a nursing home was 541 3.86 euro per month

Savings associated with staying at home compared with staying at a nursing home
Saving for staying at home with homecare of 5000 euro per month compared with staying at a nursing home
Discussion
The present study showed that the ADLife system represents a potentially useful tool to help older people with dementia to remain at home for a longer period of time, by providing an early warning system to detect a situation before it requires emergency intervention. ADLife enables monitoring of the patient's condition, providing the potential to deliver more personalized care and savings compared to the cost of staying in a nursing home. However, there were a number of operational and design problems which need to be resolved before the system can be relied on as a decision-making tool. First, information needs to be presented in a way that can be easily interpreted by formal caregivers. Second, the role of the formal caregiver needs to be revised to establish the skills they need to act as an educator to the informal caregiver and client. Third, the information provided needs to be more closely aligned to the requirements of all caregivers.
The problems experienced in introducing the technology into the home highlighted the need to fully inform clients and informal caregivers of the aims and objectives of the technology prior to installation. Whilst a user manual would provide useful information, carers highlighted the need for a professional to translate this into the context of care delivery for the client. Although skilled technicians could deliver this information, it was felt that formal caregivers should assume this role. This requires training for formal caregivers.
While the results of the evaluation indicate the benefits of the system, the study had a number of limitations. First, it did not provide quantitative evidence that ADLife could assist older people to avoid nursing home admission, for which a new study would be required. Second, the cost analysis was limited to a simple comparison of costs between homecare and care delivered in a care facility. The study did not include mandatory personal contributions under the Dutch system, the costs of informal care provision for people who live at home, or implementation costs which vary between different jurisdictions. Third, the evaluation relied on the accounts of formal and informal caregivers, and future work should include the perspectives of clients, even when they have dementia. 8 Finally, it would have been beneficial to collect data on the ‘traffic light’ system (red-amber-green) used to denote alerts. This would help in establishing the extent to which clients have been maintained within the stable areas of green and yellow, as well as documenting the ability of ADLife to highlight crisis situations and the subsequent responses.
Informal caregivers reported that use of the system provided benefits to their mental well-being. However, further investigation is required to establish if the use of ADLife would reduce visits from friends and family members, and the effect that this would have an on the overall social and emotional well-being of the older person, given the importance of face-to-face social contact. The study showed that assistive technologies can be powerful decision-making tools in their own right, but also highlighted the potential dangers arising from decisions that were based solely on the output from the technology.
In summary, the present study showed that the ADLife system enhanced the feelings of safety and security as a result of having it installed in the home. The system also appeared to reduce the burden of care on the informal caregiver and provided the potential for supporting older people to live at home for longer.
Footnotes
Acknowledgements
We thank the healthcare organizations Bruggerbosch, de Posten and the company Focus Cura BV for their support.