
Abstract
Summary
Buprenorphine is a potent analgesic commonly used clinically in humans and rodents experiencing severe pain. However, effects of therapeutic doses on locomotor activity and the cardiovascular system have not been studied in conscious animals. The effects of buprenorphine were therefore evaluated in this study using telemetric monitoring in conscious animals. Telemetry transmitters were implanted in the peritoneal cavity of Wistar rats with a pressure catheter in the aorta and electrodes for electrocardiogram (ECG) recording subcutaneously. After a single subcutaneous administration of saline, each rat was administered single subcutaneous doses of 0.006, 0.03 or 0.15 mg/kg body weight (bw) of buprenorphine. During a 10 h period after administration, buprenorphine induced a varying dose-dependent increase in body temperature, heart rate, dP/dt and systolic–diastolic blood pressure, as well as a corresponding decrease in QT time. At high dose, however, QT time was still decreased 24 h post-administration, but no arrhythmias or visual changes were observed in the ECG complex. Body temperature and heart rate increased at the high dose of buprenorphine, even at 20–24 h after administration. Moreover, the high dose of buprenorphine induced a biphasic response in diastolic blood pressure, with an early and pronounced increase that, at 14 h after administration, reversed to a decrease, failing to normalize within 24 h post-dosage. The results indicate that buprenorphine induces long-lasting effects (such as body temperature and cardiovascular effects) in the rat after a single subcutaneous dose at 0.15 mg/kg bw.
Buprenorphine is an opioid analgesic that, after parenteral administration of low doses, has approximately 24–40 times the analgesic potency of morphine in humans (Jasinski et al. 1978) and rodents (Cowan et al. 1977). It has therefore been used extensively for nearly two decades as a potent analgesic in animals experiencing severe pain, including post-surgical pain in clinical studies (Roughan & Flecknell 2002). Acute myocardial infarction (Boachie-Ansah et al. 1989) and neoplastic disease (Brema et al. 1996) are usually associated with severe pain, and it is common practice among emergency physicians to administer narcotic analgesics such as buprenorphine. Thus, physicians use buprenorphine as a current medication for a variety of patients. Moreover, the Food and Drug Administration has recently approved the use of buprenorphine for detoxification and office-based therapy for opiate addiction, particularly in individuals who are at high risk of developing acquired immunodeficiency syndrome (AIDS), hepatitis B and C and tuberculosis (Koch et al. 2006).
Buprenorphine is used in laboratory animal and human medicine because it has a long duration of action (Downing et al. 1977) and fewer cardiovascular and respiratory effects than do most other opioid analgesics for pain management (Taylor & Houlton 1984). Potential acute adverse effects of buprenorphine in humans are diffuse mild mental status changes, mild to minimal respiratory depression, small pupils and relatively normal vital signs (Sporer 2004). Moreover, it is compared with other opioids associated with a lower degree of sedation and respiratory depression (Mello et al. 1993). Studies in vitro have shown buprenorphine to have cardiac electrophysiological and antiarrhythmic effects (Boachie-Ansah et al. 1989). Buprenorphine has been shown to cause a decrease in heart rate, systolic and diastolic blood pressure, and stroke volume in anaesthetized dogs (Martinez et al. 1997). The effects of therapeutic doses of buprenorphine on the cardiovascular system have not been studied in conscious animals, however.
Because absorption of buprenorphine from the gastrointestinal tract is low, parenteral routes of administration are preferable. The recommended postoperative subcutaneous dose of buprenorphine is 0.05 mg/kg body weight (bw) (Thompson et al. 2004). A single oral dose of 0.5 mg/kg bw in rats produces analgesic effects for 6–8 h (Gades et al. 2000), but the obtained analgesic efficacy is more robust when 0.05 mg/kg bw is administered subcutaneously (Thompson et al. 2004). Absorbed buprenorphine is readily distributed in different body compartments, with a peak plasma concentration at approximately 90 min and a half-life of 4–5 h (Sporer 2004).
Telemetric monitoring of conscious laboratory animals has proven useful in the acquisition of reliable physiological data (Eisermann 1988, Brackee et al. 1995) and has many advantages over conventional data acquisition techniques in risk assessment of drugs and food constituents (Ilbäck et al. 2002a,b, 2007).
The aims of this study are to use telemetric monitoring in the evaluation of spontaneous locomotor activity, body temperature and cardiovascular effects that are caused by different doses of buprenorphine and to study whether the observed effects were dose-dependent.
Materials and methods
Animals and housing
Wistar Hannover GALASTM (HanTac:WH) female rats (aged 7 weeks) obtained from Taconic M&B, Ry, Denmark, were used. A microbiological health status was obtained from the supplier showing no infections to be declared according to FELASA (2002). During the experiment, clinical examination was performed daily and individual body weight was determined weekly. Rats were 13 weeks old at the time of surgery and 18 weeks old when the experiment was initiated. The body weight of the rats was approximately 300 g on the day the experiment began. The animals were housed in a barrier building and identified by an individual unique tattoo on the tail.
Animal room controls for temperature and relative humidity were set at 21 ± 1°C and 55 ± 5%, respectively. The light was controlled to provide 12 h of light (06:00 h to 18:00 h) and 12 h of darkness per 24 h.
The rats were kept in individual cages (Eurostandard Type III, Technoplast, Buguggiate, Italy). The cages, cage trays, food hoppers and water bottles were sanitized twice weekly. All animals were given free access to both food (RM1 [E] SQC Ltd, UK, vendor Scanbur A/S, Karlslunde, Denmark) and tap water. There was no indication that any (non-nutrient) substance was present in the diet or in the drinking water that influenced the effects of the test compound.
The animal experiments described in this paper took into account all ethical aspects of the welfare of the animals and were performed following the recommendations in the Guide for the Care and Use of Laboratory Animals of the Swedish National Board for Laboratory Animals (CFN). The experiment was approved (No. M255-03) by the Research Ethics Committee at the University of Lund (Malmö/Lund, Sweden).
Compound
Commercially available Temgesic stock solution in vials containing buprenorphine hydrochloride (0.3 mg/mL) was obtained from Schering-Plough, Stockholm, Sweden. The stock solution was diluted in physiological saline (NaCl) with a pH of 7.0. Dilutions of the test formulations (0.006, 0.03 and 0.15 mg/mL) were performed by the Department of Pharmacy, Active Biotech AB, Lund, Sweden. The placebo was saline (NaCl solution) with a pH of 7.0. The placebo solution and the test formulations were administered subcutaneously to achieve the three dose levels (i.e. 0.006, 0.03 and 0.15 mg/kg bw).
Experimental procedure
Anaesthesia
The rats (n = 4) were anaesthetized by inhalation with a mixture of isoflurane (Baxter Medical, Kista, Sweden), O2 and N2O using a Penlone PPVS Sigma vaporizer (AgnTho's, Lidingö, Sweden). The anaesthesia was induced by placing the rat in a gas chamber filled with 4% isoflurane. When anaesthesia was established, the rat was removed from the chamber and the vaporizer was connected to a mask covering the rat's head. The concentration of isoflurane was adjusted (approximately 1.5–3.0%) to ensure an adequate depth of anaesthesia.
Surgical preparations
Each rat was placed on a heated bed (Kanthal, AB Ninolab, Upplands Väsby, Sweden) during surgical preparation. Under aseptic conditions, an abdominal incision of about 5–6 cm was made to the right of the midline; at this time, the intestines were retracted and the abdominal aorta exposed. The catheter of the transmitter was inserted into the vessel and sealed in place with tissue adhesive. The intestines were gently put back in place and the flap of the transmitter was secured to the abdominal wall. After the telemetry transmitters had been implanted in the peritoneal cavity with the pressure catheter in the aorta, electrodes for electrocardiogram (ECG) monitoring were placed subcutaneously on the right side of the thorax and near the left hindlimb.
After surgery, the rats were subcutaneously treated with the recommended postoperative dose (0.05 mg/kg bw) of buprenorphine (Thompson et al. 2004) and kept under continuous observation in the postoperative unit until they had regained full consciousness, at which time the animals were transferred back to their cages. Approximately four weeks after surgery, the rats entered the study. When treatment and all registrations according to the protocol were finished, the rats were administered a lethal dose of pentobarbital.
Treatment and experimental design
The rationale for selection of the dose levels (i.e. 0.006, 0.03 and 0.15 mg/kg bw) was based on the combination of clinical use and earlier studies in rats with single doses of buprenorphine (Hayes & Flecknell 1999, Sharp et al. 2003). Each rat was administered with a single subcutaneous dose; for each dose, responses in four rats were investigated. The time point for administration of buprenorphine is marked with an arrow in the figures. The rats (n = 4) were administered with the placebo saline (NaCl) solution subcutaneously to register the individual baseline for 24 h. After this period, the different buprenorphine doses were administered at increasing dose levels with at least a seven-day washout period between the doses. By this experimental design, each rat served as its own control.
Test procedure and recordings
TL11 M2-C50-PXT transmitters (Datasciences Inc, St Paul, MN, USA) were used. The transmitters were turned on one day before implantation in order to stabilize the signal and to check the zero offset value. The signals from the transmitters were received by two RLA 2000 receivers and transmitted via a Data Exchange Matrix to a Dataquest PCI card CQ 2240 in the computer. The data were interpreted by the Dataquest program ART version 2.2 Gold Version.
Program set-up and checks
Registration was made with the Dataquest acquisition program version 2.2 and run with the operative system Windows NT 4.0. The configuration file was set as follows: for blood pressure, the sampling rate was 500 Hz with a filter cut-off set at 100 Hz and full scale at 500 mmHg. The sampling rate for ECG was 1000 Hz with no filter cut-off and full scale at 10 mV.
Sampling of ECG, blood pressure, body temperature and locomotor activity
The data were stored on a hard disk in accordance with the parameters entered in the configuration files. Refractory for diastolic and systolic blood pressure and heart rate was 0.2. Sampling duration for ECG, heart rate, and systolic and diastolic blood pressure was set to 10 s. Data were sampled once per minute. Locomotor activity was registered through horizontal movement of the transmitter, i.e. each movement results in a count.
Data evaluation and statistical procedures
Values of systolic and diastolic blood pressure, heart rate, body temperature and locomotor activity were imported to Microsoft Excel, and from these data diurnal mean values and correlation were calculated. Statistical evaluation of the effects of buprenorphine on body temperature, heart rate, systolic and diastolic blood pressure and QT time were performed between 11:00 h and 15:00 h and between 05:00 h and 08:00 h. All ECG recordings were investigated visually for signs of arrhythmia or changes in the shape of the ECG complexes. For the dP/dt values after the first, second and third buprenorphine doses, significances were calculated using the Neuman-Keuls test and the confidence limits (95%) of the ratio of the mean values (Tallarida & Murray 1987). The dP/dt means the rate of change of the ventricular pressure with respect to time (cardiac contractility). Because of the enormous amount of data collected over 24 h, results have to be presented in a pattern of changes in which dose effects can be compared in general.
Results
Our observations indicated that the rats did not develop any visual signs of adverse effects during or after treatment with the presently used single doses (0.006, 0.03 or 0.15 mg/kg bw) of buprenorphine administered subcutaneously. The data points shown in Figures 1–7 are mean values of 10 registrations, whereas in Figures 8 and 9 all data points are shown.
The administration procedure, as shown after the administration of the saline solution, rapidly induced an increase in heart rate, body temperature, locomotor activity and systolic blood pressure, all of which lasted for approximately 1–2 h (Figures 1–9). Buprenorphine was found to affect, to various degrees, body temperature, spontaneous locomotor activity, heart rate, dP/dt, systolic and diastolic blood pressure and QT time (Figures 1–9). Thus, depending on the dose, the responses varied in quality, quantity and duration. Body temperature, spontaneous locomotor activity and heart rate were found to correlate (r > 0.8) during the 24 h after saline administration, but not after administration of the medium and high doses of buprenorphine.
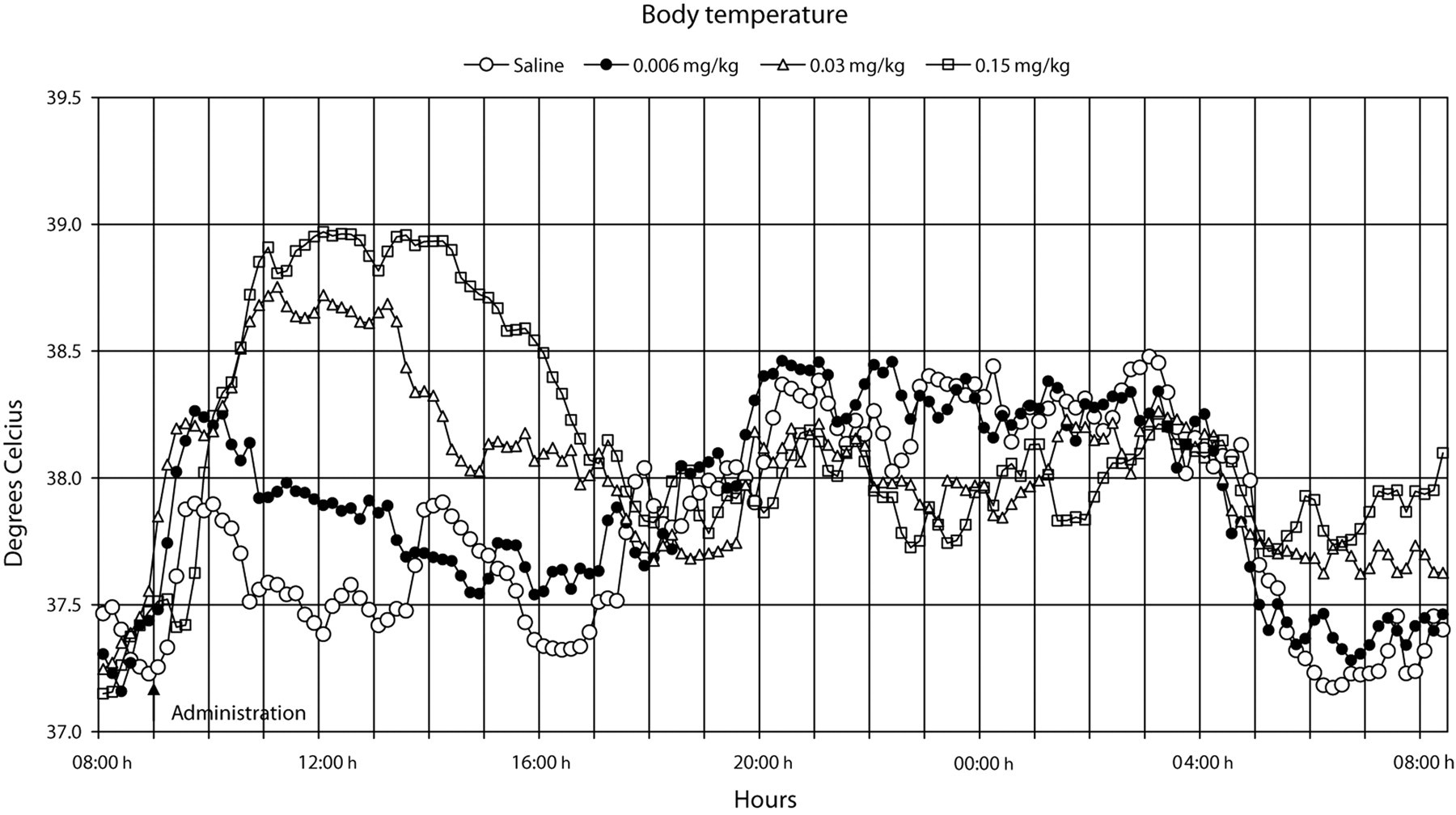
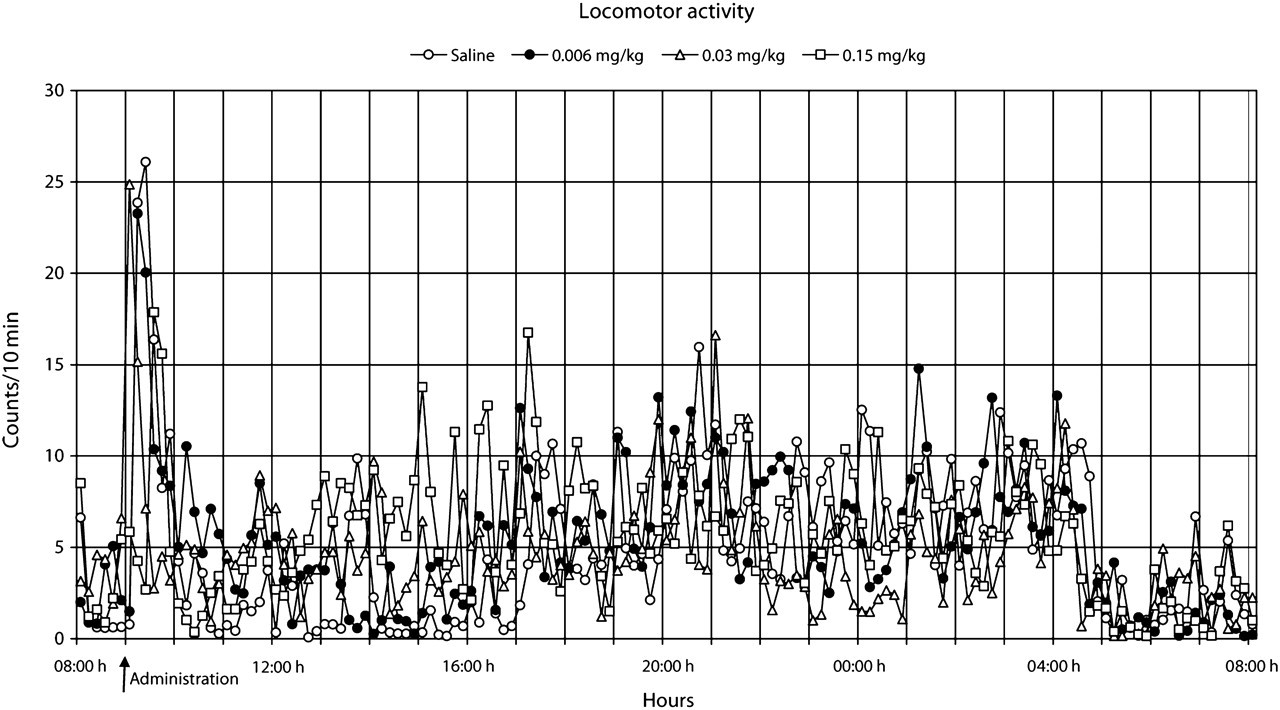
All doses of buprenorphine, when compared with saline, induced a dose-dependent increase in body temperature, both early and late periods after administration (P < 0.05, medium and high dose) (Figure 1). At the low dose of buprenorphine, the increase was minor, lasting for about 5 h, whereas at the medium and high doses, the increase in body temperature was dose-dependent and more pronounced, remaining at an increased level for about 9 h. A decreased body temperature was observed with saline and low dose of buprenorphine 20 h after administration, probably because of the normal changes in diurnal rhythm and an associated decrease in spontaneous locomotor activity (Figure 2). However, at the medium and high doses of buprenorphine, this decrease in body temperature did not occur at 20–24 h post-administration. A tendency of increased spontaneous locomotor activity, observed between 3 and 9 h after administration, was noted with the high dose of buprenorphine (Figure 2).
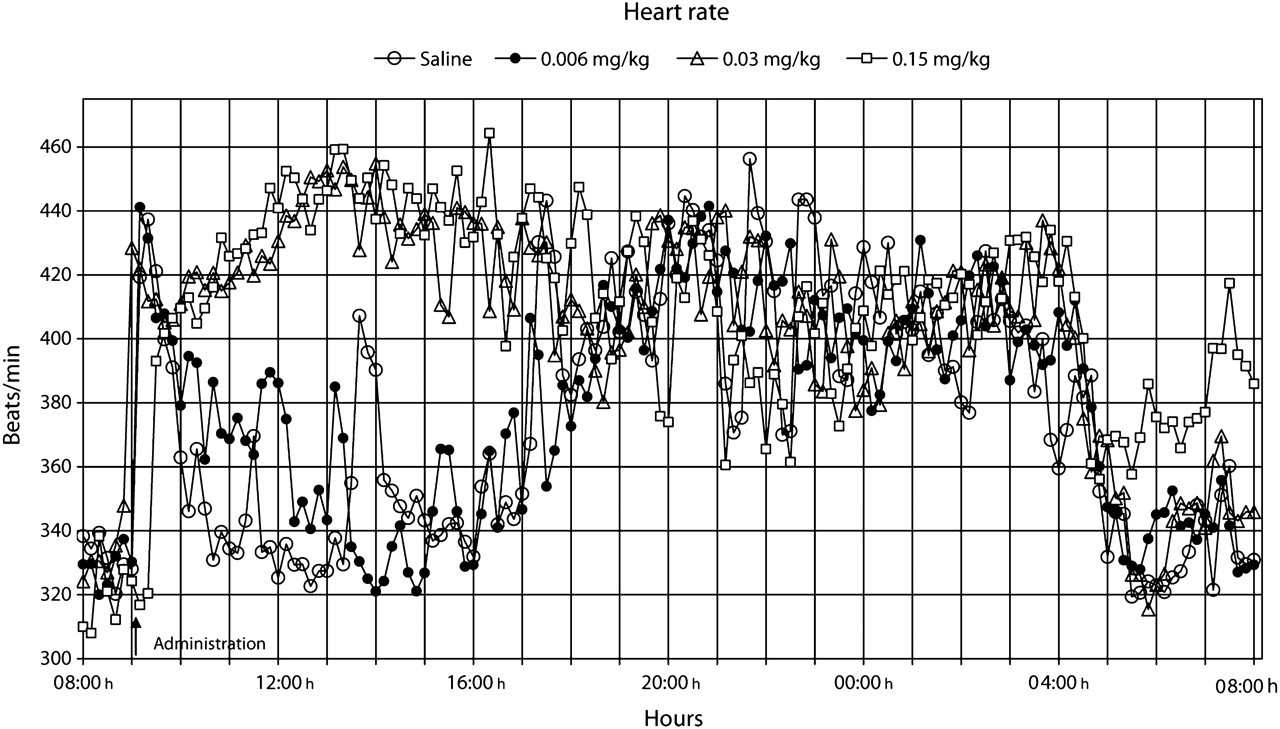
The heart rate normalized within 2 h after the administration of saline and the low dose of buprenorphine (Figure 3). However, a pronounced but similar increase (P < 0.05) in heart rate lasted approximately 9–10 h after administration of the medium and high doses of buprenorphine. At 10 h after administration, a normal heart rate frequency was also reached at these (i.e. medium and high) dose levels. However, 20 h after administration of saline or buprenorphine, the heart rate decreased at all dose levels, which was due to the normal diurnal rhythm, except for the high dose in which it did not normalize (P < 0.05) within 24 h post-dosage.
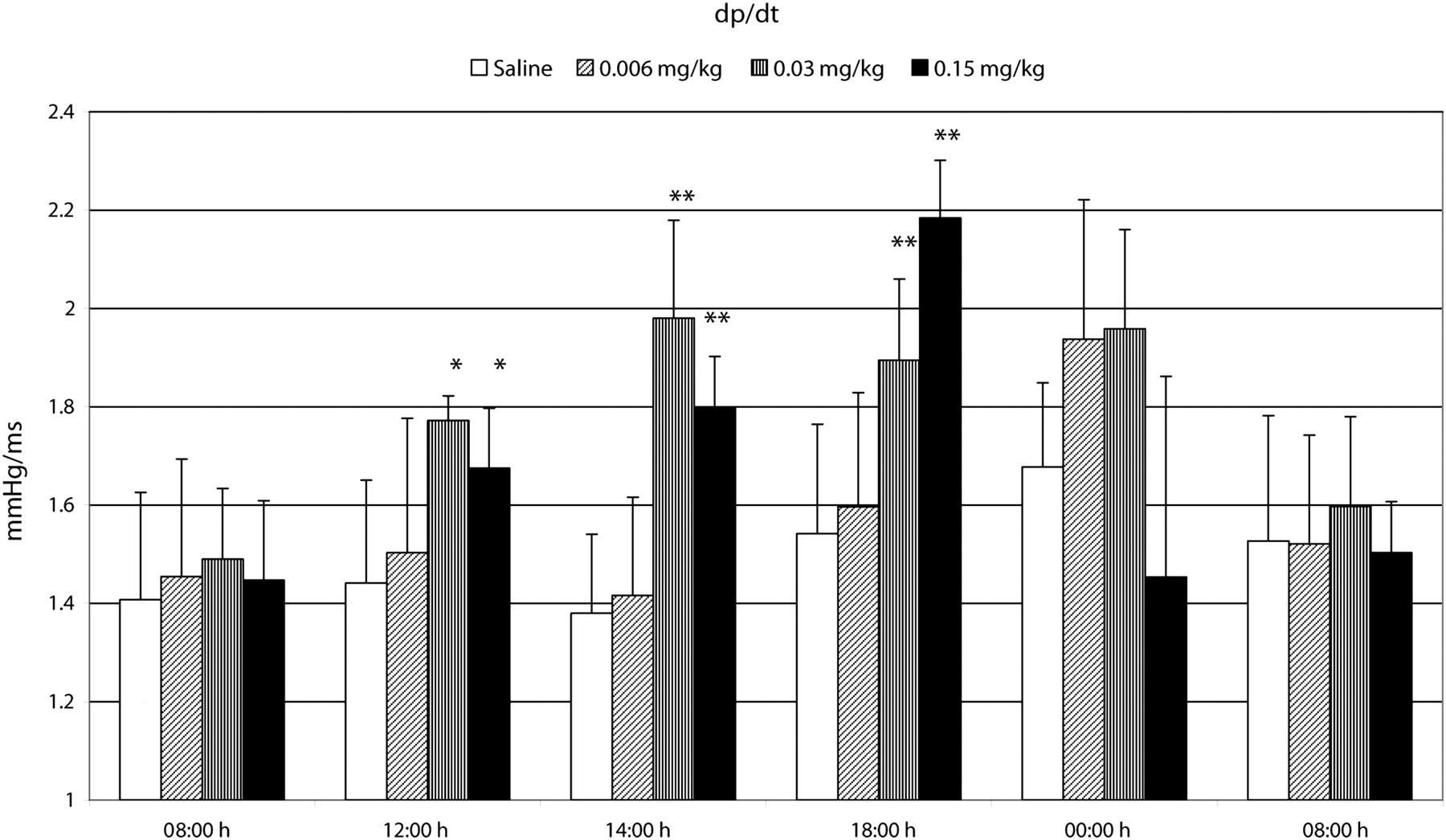
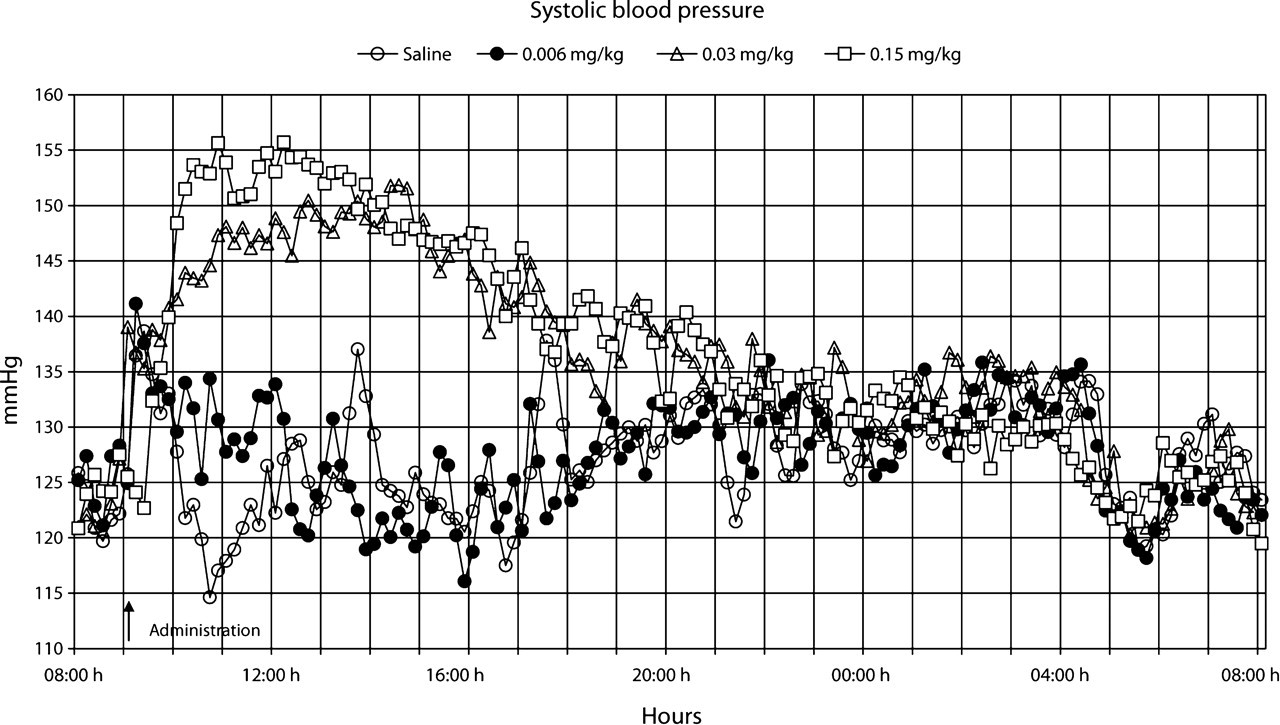
At the medium and high doses of buprenorphine, a substantial increase in dP/dt was observed 4–14 h after administration (Figure 4) and a concomitant increase in systolic (Figure 5) and diastolic (Figure 6) blood pressure (P < 0.05) 2–13 h after administration. This increase corresponded well to the period when changes in heart rate were observed (Figure 3). After administration of saline and the low dose of buprenorphine, systolic and diastolic blood pressure had normalized within 2 h. At the medium dose of buprenorphine, approximately 10 h were required until normal diastolic blood pressure was attained. Similarly, at the high dose, normal diastolic blood pressure was established within 10 h after administration, but the diastolic blood pressure at 14 h after administration reversed to a decrease (P < 0.05) that did not normalize within 24 h post-dosage.

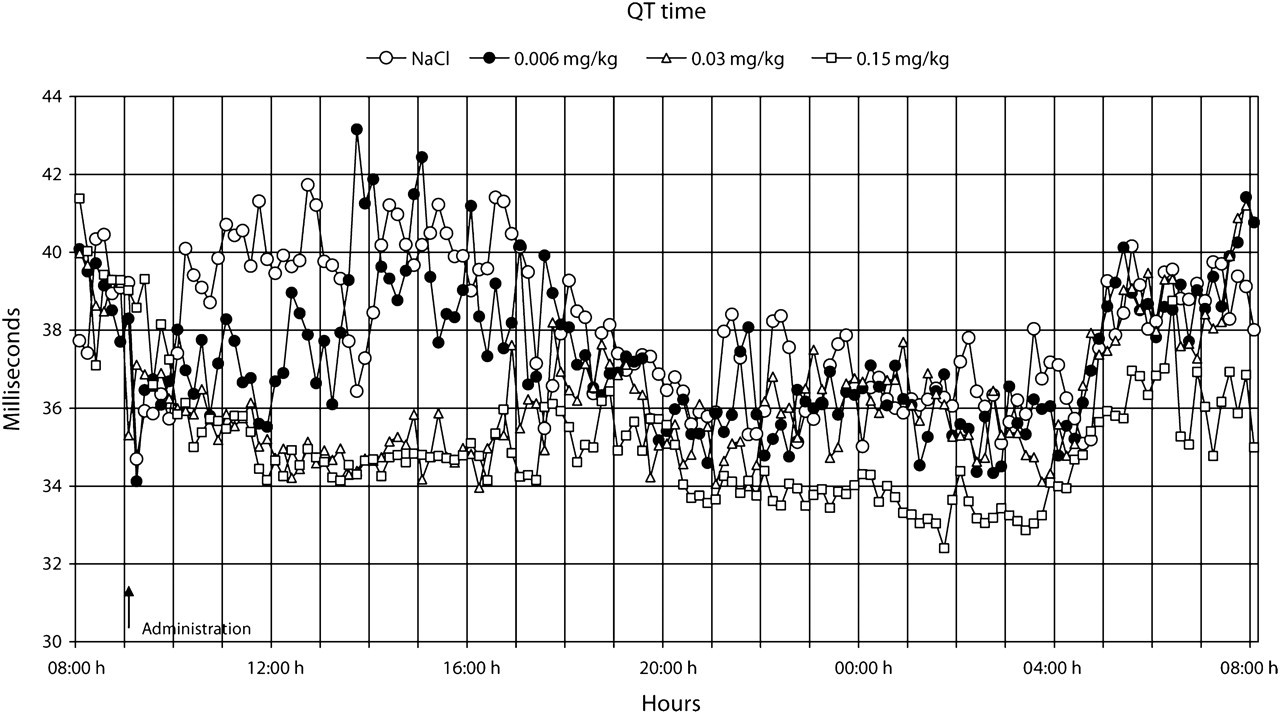
The QT time showed a dose-dependent decrease (P < 0.05, medium and high doses of buprenorphine) 2–10 h after administration (Figure 7), which corresponded to the period of increased heart rate (Figure 3). After this period, QT time was normalized at the low and medium doses, but not at the high dose, where QT time remained non-significantly decreased even 24 h after administration. The cardiovascular effects observed at the high dose of buprenorphine were not associated with any arrhythmias or changes in the ECG pattern.
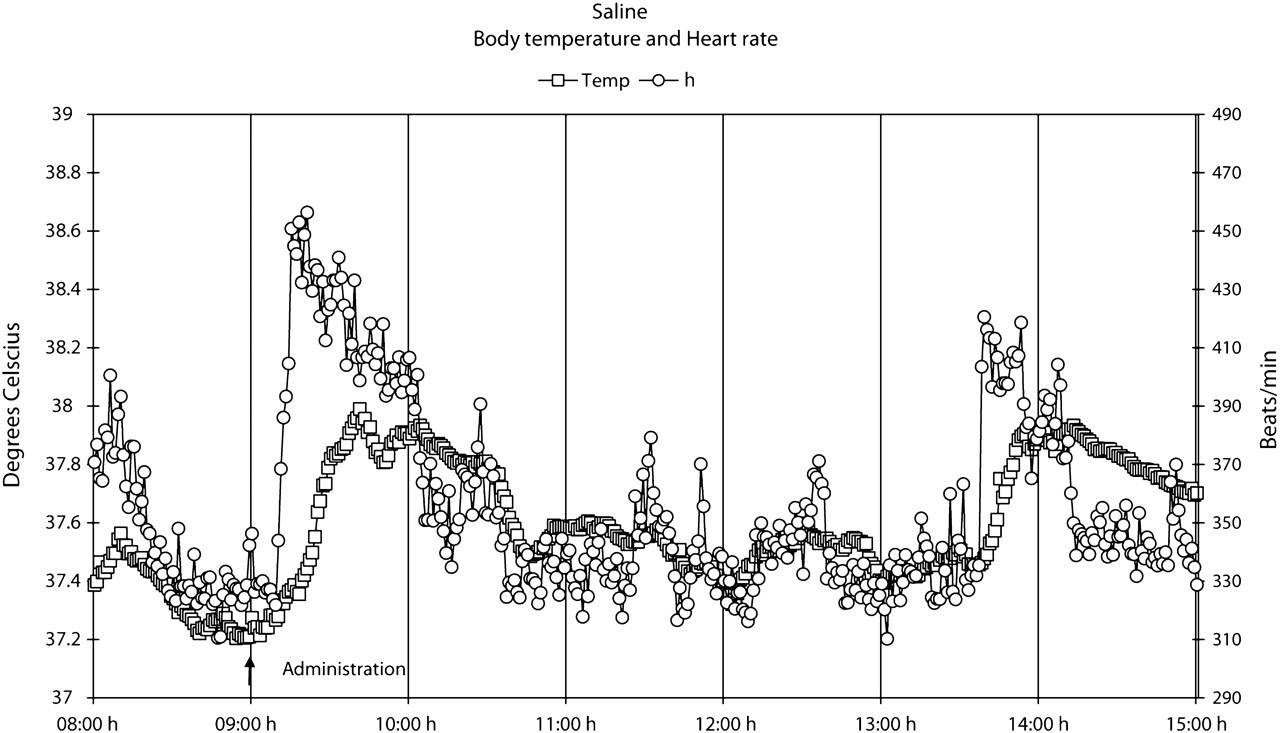
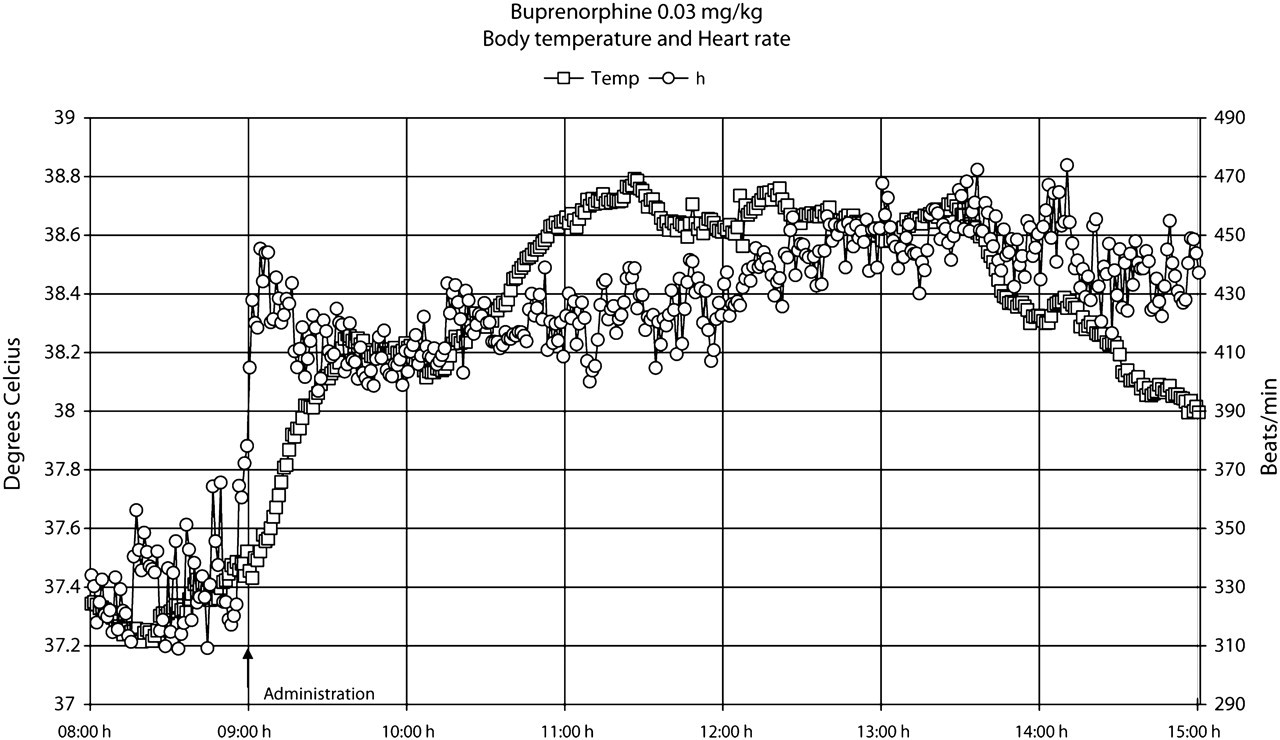
The results also showed that the increase in heart rate preceded the increase in body temperature, both after saline and buprenorphine administration (Figures 8 and 9). Moreover, during the 24 h following buprenorphine administration, increases and decreases in body temperature occurred even though no changes were observed in heart rate (Figure 9).
Discussion
During a 10 h period after administration of buprenorphine, the analgesic was found to cause, to various degrees, a dose-dependent increase in body temperature, heart rate, dP/dt, systolic and diastolic blood pressure and a corresponding decrease in QT time. At the high dose of buprenorphine, body temperature and heart rate were increased even 20–24 h after administration, whereas the increase in diastolic blood pressure reversed to a decrease, not normalizing within 24 h post-administration. Similarly, the medium dose caused a persistent increase in body temperature. Thus, the results at the medium and high doses exhibited some previously unknown long-lasting effects of buprenorphine. However, no signs of arrhythmia or changes in the ECG complex were observed.
The administered doses of buprenorphine in this study were well tolerated and toxic/pharmacological effects were minor in comparison with those effects reported to be associated with a high intake of buprenorphine in which severe adverse effects and response patterns develop, including respiratory depression and death (Gueye et al. 2001). It was intriguing to note how well spontaneous locomotor activity, body temperature, heart rate and blood pressure changes followed each other in the saline-treated rats.
Buprenorphine seems to be a valuable agent for pain relief in a wide range of animal species when used in an appropriate manner (Roughan & Flecknell 2002). After buprenorphine administration, plasma concentration peaks at approximately 90 min with a half-life of 4–5 h (Sporer 2004). A single high dose of 0.5 mg/kg administered subcutaneously to rats produces analgesic effects over a 6–8 h period (Gades et al. 2000). Symptoms of buprenorphine in clinically treated patients persist from 12 to 24 h (Pickworth et al. 1993, Sporer 2004). This pattern corresponded well to the duration (i.e. approximately 10 h) of the presently observed treatment-related effects.
A new finding in this study was that buprenorphine induced dose-dependent hyperthermia in the rats. This effect was probably not immune-mediated because buprenorphine has not been shown to affect immune system functions (Gomez-Flores & Weber 2000). In addition, buprenorphine has been shown to increase the general activity of rats in some studies (Gades et al. 2000, Roughan & Flecknell 2002) but not in others (Hansen et al. 2002). In the present study, there was only a tendency of minor increase in spontaneous locomotor activity. Thus, the reason for the concomitant increase in body temperature and heart rate could not be explained by increased spontaneous locomotor activity. It is evident that the increase in heart rate immediately after buprenorphine administration precedes the increase in body temperature. These early effects, however, are probably related to a stress effect associated with the administration procedure. It was noteworthy that in the 24 h following buprenorphine administration increases and decreases in body temperature occurred even though no changes were observed in heart rate. Moreover, the medium and high doses of buprenorphine induced a similar response in heart rate but a dose-dependent increase in body temperature. It is therefore tempting to suggest that buprenorphine, in addition to possible cardiovascular effects, directly influences regulatory mechanisms of body temperature.
It is apparent from the literature that buprenorphine can either directly or indirectly affect the respiratory and cardiovascular system (Boachie-Ansah et al. 1989, Gueye et al. 2001). Buprenorphine has been reported to cause a decrease in heart rate, systolic and diastolic blood pressure, and stroke volume in anaesthetized dogs (Martinez et al. 1997). However, the effects of therapeutic doses of buprenorphine on these parameters have not been studied in conscious animals. We found that buprenorphine caused an early and dose-dependent increase in heart rate, dP/dt and systolic and diastolic blood pressure. Thus, it is worthy to note the completely different cardiovascular responses in this study in conscious animals when compared with those reported in anaesthetized animals (Martinez et al. 1997). Moreover, at the high dose of buprenorphine (0.15 mg/kg bw), long-lasting and previously not reported drug-induced effects were observed, i.e. effects on diastolic blood pressure, QT time, body temperature and heart rate did not normalize within 24 h post-dosage. The mechanisms underlying these new findings that appeared late after the administration of buprenorphine, are not known and thus need to be studied.
Our study showed a clear dose-dependent increase in body temperature and associated heart rate responses. Although atrial fibrillation and ventricular tachycardia have been associated with prolongation of P-wave and QRS complex duration (Guidera & Steinberg, 1993, Lander et al. 1993), buprenorphine reduced the QT time in the present study. Moreover, no arrhythmias or effects on the ECG complex were observed at visual inspection.
Although only four animals per dose were used, the telemetry model in the conscious, unrestrained rat seems to be sensitive and demonstrate high predictive power in the evaluation of toxicological/pharmacological effects induced by buprenorphine. These results in the rat indicate that a single high dose of buprenorphine (0.15 mg/kg bw) may induce long-lasting effects, though this does not seem to involve changes in the ECG complex.
Footnotes
Acknowledgement
This study was supported by grants from the Faculty of Medicine, Uppsala University, Uppsala, Sweden.