
Abstract
Objective
To evaluate the impact of a patient decision aid (PDA) regarding the use of natural health products (NHPs) at menopause on decisional conflict, knowledge of NHPs, congruence between values and choice, persistence with an option, intention to disclose the use of NHPs to a physician or a pharmacist and intention to use decision support interventions in the future.
Study design
A randomized controlled trial in which 90 women, aged 45–64 years, facing a decision about using NHPs for menopausal symptoms, received a PDA (experimental group) or a general information brochure about menopause (control group).
Main outcome
Decisional conflict.
Measures
Women were evaluated at baseline and after a two-week period using the decisional conflict scale (DCS). Analysis of covariance was used to determine the differences between both groups on the DCS.
Results
Both groups experienced a statistically significant reduction on the DCS (−0.55 ± 0.59, P < 0.0001 versus −0.52 ± 0.73, P < 0.0001). However, there was no statistically significant difference between the groups (P = 0.32). Both groups experienced a statistically significant improvement in knowledge of NHPs (0.86 ± 1.77, P = 0.002 versus 0.51 ± 1.47, P = 0.031). However, there was no statistically significant difference between the groups (P = 0.162).
Conclusion
A PDA regarding the use of NHPs for menopausal symptoms impacted favourably on women's decisional conflict, but was not superior to a general information brochure on menopause.
Keywords
Introduction
Making decisions about natural health products (NHPs) for managing menopausal symptoms is difficult. 1,2 NHPs refer to a family of products that includes herbs, vitamins, minerals, essential fatty acids and homeopathics. They are derived from plants, animals or microorganisms, and may be used to prevent, diagnose or treat disease, restore or correct function, and maintain or promote health. 3 Sources of information about NHPs are perceived as unreliable by middle-aged women because their content is poorly conveyed, contradictory or biased. 1,4 Women also perceived physicians as being ignorant about NHPs and more likely to exert pressure for the use of hormone therapy for managing menopausal symptoms. 5 Consequently, it is no surprise that middle-aged women consider using NHPs without mentioning their intentions to their health-care providers. This is of concern because they might be at a risk for undesirable NHP–conventional medication interactions. 6
In order to respond to the needs of individuals facing difficult health-related decisions, patient decision aids (PDAs) have been proposed. 7 In a Cochrane systematic review of 55 randomized controlled trials (RCTs), PDAs were found to enhance decision quality for patients by reducing uncertainty and improving the decision process measures of feeling informed and being clear about values. 8 More recently, PDAs have been proposed as the standard of care for informed decision-making. To the best of our knowledge, at the time this study was conceived, there were no PDAs for middle-aged women who were considering NHPs for menopausal symptoms.
Consequently, our objective was to evaluate the impact of a PDA on decisional conflict of middle-aged women who were considering NHPs for menopausal symptoms. Our main research hypothesis was that women exposed to the PDA would experience a greater decrease in their decisional conflict than those in the control group.
Methods
Study design
An RCT was conducted in French in Québec City in May and June, 2006.
Participants and recruitment procedure
Inclusion criteria were: (1) women aged from 45 to 64 years; (2) suffering from symptoms of menopause; (3) considering NHPs for their menopausal symptoms; (4) able to read, understand and write French at grade-8 level and (5) capable of giving free, informed consent for their participation in the study. We excluded women who reported symptoms for which there was no precise diagnosis, owners and/or managers of natural health food stores, pharmaceutical companies or pharmacies and individuals with a close relationship with one of the investigators in this study. We did not exclude women who reported using NHPs because it was deemed possible that they may reconsider their choice. Publicity for this trial was placed in local newspapers and various locations, including pharmacies, community-based women's groups, family medicine clinics as well as gynaecology and obstetrics clinics.
Randomization
The randomization schema was carried out by a biostatistician using computer-generated unequal blocks. Sealed opaque envelopes containing one or the other documents (a PDA in the intervention group and a general information brochure in the control group) were prepared by another individual, external to the study. The investigators and research assistant involved in data collection and analysis were blinded to the participants' assignment.
Intervention group
This group received the paper-based PDA developed by our research team. 9 In-line with the recommendation of the International PDA Standards (IPDAS), 7 and based on the Ottawa Decision Support Framework, 10 it consisted of a six-stage process: (1) be clear about the decision to be made; (2) get the facts based on the best evidence available; (3) identify the available options; (4) clarify what is important; (5) select the role in making the decision; and (6) next steps. A copy is available on request from the authors.
Control group
This group received the paper-based general information brochure, produced and distributed by a community-based women's group. The brochure focused on the physiological aspects of menopausal symptoms and provided advice on a diverse range of ways to manage these. It did not focus on making a decision regarding the use of NHPs for menopausal symptoms, but mentioned a few aspects regarding a smaller number of NHPs than the PDA. It did not address risks and benefits regarding the NHPs that had been identified. It did not address the lack or presence of evidence regarding NHPs.
Outcome measures and data collection
At baseline (T1), women completed a self-administered questionnaire that included the following.
The decisional conflict scale (DCS) was used to assess for decisional conflict (primary outcome).
11
The DCS is a validated scale (Cronbach's α ranged from 0.78 to 0.92).
12
It comprised 16 items divided into five subscales: uncertainty, inadequate knowledge, unclear values, lack of support and ineffective choice. Each item is measured on a 5-point Likert scale (1 [strongly agree] to 5 [strongly disagree]). The DCS total score was obtained by summing up the 16-item scores and dividing by 16, resulting in a score that ranged from 1 (low-decisional conflict) to 5 (high-decisional conflict). Individuals with a cut-off value of 2.5/5 or more on the DCS, experience clinically significant decisional conflict that in turn is associated with lack of knowledge on the options, delaying a decision and decisional regret.
11
Knowledge of NHPs was assessed with a knowledge test based on needs assessment,
9
literature review and advice from clinicians on what a middle-aged woman would need to know to make an informed decision regarding the use of NHPs for menopausal symptoms. It comprised 10 items, each on a response scale of yes (correct answer), no and unsure (wrong answer). The knowledge score was obtained by summing up the 10 items (0 [no correct answers] to 10 [all correct answers]). Preference for an option was assessed by asking women if they intended to use NHPs on a scale of 1 [definitely not using NHPs] to 15 [definitely using NHPs];
13
Personal values regarding NHPs refer to the importance given to different aspects of NHPs.
10
It was assessed with an existing questionnaire that was modified according to a number of important aspects mentioned by the women who participated in focus groups during the needs assessment.
9
Sociodemographic characteristics were assessed and women completed the menopause rating scale (MRS).
14
Women received the specific brochure based on their random assignment and were given two weeks to use it. As a reminder, women received a phone call at the end of the first week. No questions were allowed during this call. The last data collection was performed at the end of the second week (T2), during a telephone interview conducted by a research assistant who was blinded to the intervention group. Women were assessed on the same measures as at baseline except for their sociodemographic characteristics and the MRS. The intention of women to disclose their use of NHPs to their doctor or pharmacist (three items; Cronbach's α = 0.82) and intention to use the document they had been assigned to in the future (three items; Cronbach's α = 0.80) were assessed.
15
All participants were advised not to share the document they had been assigned with others, in order to limit potential contamination between the groups.
Sample size and data analysis
A total of 35 women in each group would allow the observation of an average improvement of 0.4 (moderate effect size) with a power of 80% and a threshold error of 5%. 16 Taking into account possible dropouts (30%), we aimed at recruiting 100 women. Data were treated blindly by a biostatistician. Descriptive analysis was performed using mean with standard deviations. For ordinal and interval measures, a paired t-test was used to compare the results within each group. Intent-to-treat analysis was performed. Analysis of covariance (ANCOVA) was used to compare the results between each group while controlling for baseline scores. Categorical variables were analysed using a chi-square. To test the impact of the intervention on the congruence between personal values and choice, preference for an option (on a scale of 1 [definitely not taking NHPs] to 15 [definitely taking NHPs]) was entered as a dependent variable in a multiple regression model, with the items pertaining to personal values regarding different aspects of NHP as well as the intervention entered as covariates. Two regression models were created: one at baseline and one after the use of the brochure. To test the impact of the brochure on the persistence with an option, a posteriori, a new variable was created to identify three categories with preference for an option: scores of 5 or less were identified as ‘not taking NHPs;’ score of 6 to 10;’ uncertain;’ scores of 11 or more, ‘taking NHPs.’ The Statistical Analysis System version 9.1 (SAS Institute, Cary, NC, USA) facilitated data analysis.
Results
Participants
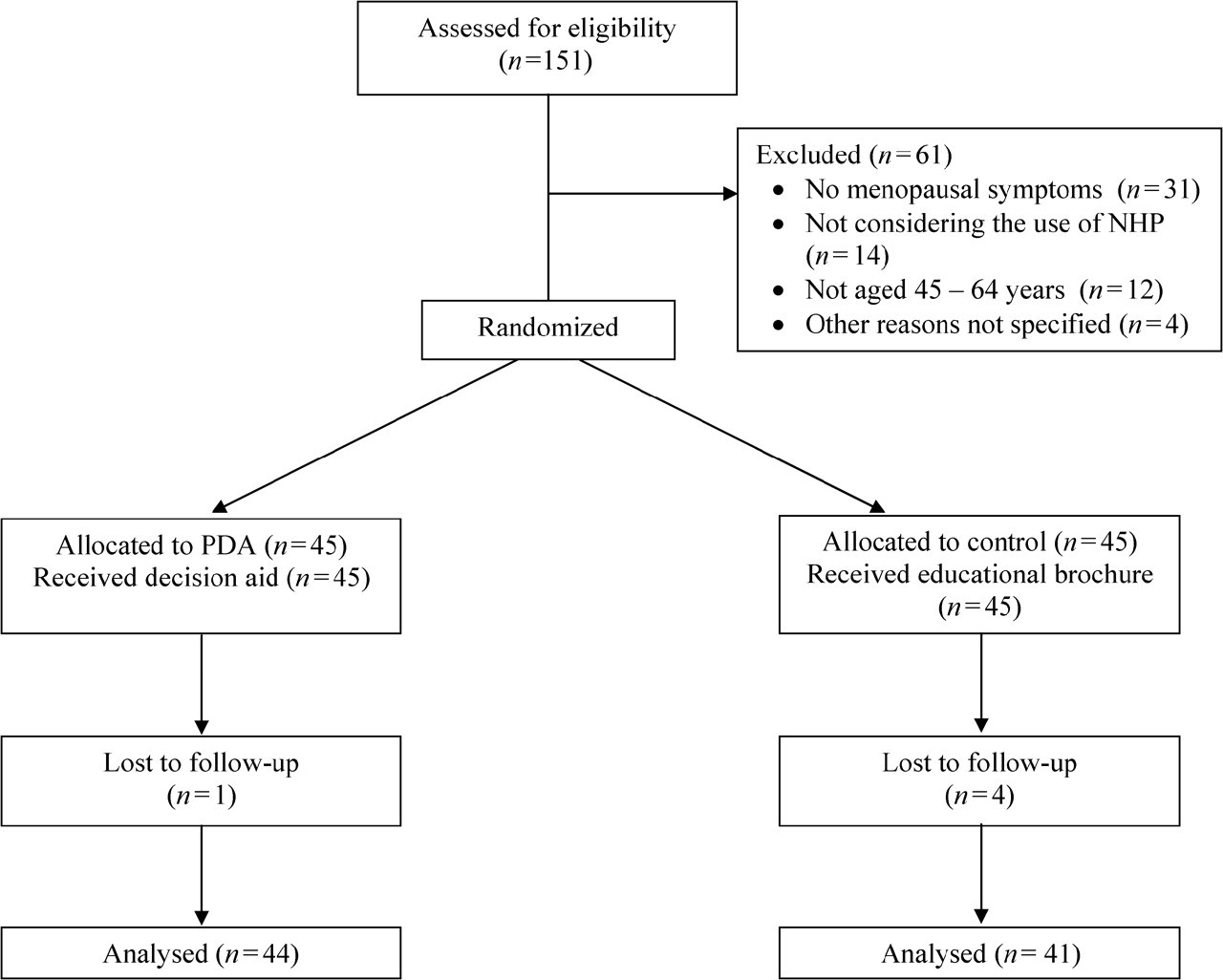
A total of 43 women in the PDA group and 41 in the control group completed the study (Figure 1). The only reason for loss to follow-up at the end of the two weeks (one intervention; four controls) was the impossibility of reaching the participants despite multiple phone calls. There was no statistically significant difference in women's characteristics between groups (Table 1). The typical participant was in her mid-50s, married, had completed secondary school and was employed full time with an income of > CAN$60,000. Most women were postmenopausal with few experiencing distressing symptoms.
Trial flow
Characteristics of participants
SD, standard deviation; NHP, natural health products; MRS, menopause rating scale.
Primary outcome: decisional conflict
At baseline, there was no difference between groups on decisional conflict (2.60 ± 0.84 controls versus 2.47 ± 0.69 decision aid, P = 0.77). At two weeks, women in both groups obtained a statistically significant decrease in decisional conflict (−0.55 ± 0.59, P < 0.0001 and −0.52 ± 0.73, P < 0.0001, respectively). ANCOVA showed no statistically significant difference between groups (P = 0.32). Table 2 shows detailed information for total DCS and each of the five subscales.
Means scores of the decisional conflict scale (sub scales and total) according to study group (range from 1 [low-uncertainty] to 5 [high-uncertainty])
DCS, decisional conflict scale; SD, standard deviation.
aANCOVA (Controlled for Baseline DCS Score).
Secondary outcome analyses
Knowledge test
At two weeks, women in the PDA group showed greater improvement in their knowledge test than women in the control group (0.86 ± 1.77, P = 0.002 versus 0.51 ± 1.47, P = 0.031), but there was no statistically significant difference between groups (P = 0.162).
Congruence between personal values and preference for an option
When we tested the first regression model to assess the preference for an option at baseline explained by personal values (independent variables) and the intervention (covariate), it was not statistically significant (F = 1.13, P = 0.35). A second regression model assessed the preference for an option after exposure to the intervention, explained by the same personal values (independent variables), and the intervention (covariate) was statistically significant (F = 4.30, P = 0.0009). The personal value statement found to be positively associated with women's preference for an option was ‘what is the importance you give to the non-chemical aspect of NHPs?’ (ß = 0.71, P = 0.006). However, the variable ‘intervention’ was not statistically significant (P = 0.33). In other words, the intervention, namely the decision aid, was not associated with women's preference for an option.
Preference for an option
At two weeks, women in both groups showed a statistically significant change in their preference for an option (P = 0.0002 decision aid versus P = 0.01 controls) (Table 3). Although there was a reduction in the number of women who were uncertain after using the decision aid compared with controls (48–36% compared with 46–44%), these findings were not statistically significant (P = 0.61).
Preference for natural health products (NHP)
Intention to disclose use of NHPs and to use the intervention in future
At two weeks, the intention of women in the PDA group to disclose their use of NHPs to their physician or pharmacist was 1.63 ± 1.83 (on a scale of −3 [no intention to disclose use] to +3 [positive intention to disclose use]) compared with 1.21 ± 1.92 in the controls (P = 0.312). Women's intention to use the PDA in the future was 1.21 ± 1.70 compared with 0.88 ± 1.91 in the control group (P = 0.41).
Discussion
Our study results are important because, to the best of our knowledge, they are the first to explore the impact of a PDA concerning the use of NHPs for menopausal symptoms on women's decisional conflict. Overall, we observed a significant improvement in the decisional conflict of women within both groups. However, the results from our study did not support our main research hypothesis regarding the superiority of the PDA over the general information brochure. There are a few reasons that might explain these findings.
PDAs are interventions that have only been recently developed to help people make informed choice among many options by offering evidence-based information about the options and potential benefits and harms. 7 They are still the object of much research regarding which of their components are the most effective. 17 In our study, women in the control group were exposed to a general information brochure on menopause that had been produced by a community-based women's group. This brochure did not meet most of the IPDAS criteria and thus did not include a detailed section on evidence-based information about the risks and benefits associated with each available option. 7 Although our PDA included such a detailed section, women could read that there was very little evidence on most NHPs for menopausal symptoms. Therefore, future studies will need to address what PDA developers should do when there is little evidence about the options made available to patients and how this lack of evidence should be presented to patients.
Although a meta-analysis of PDAs has shown that overall, PDAs do reduce decisional conflict, a few RCTs of PDAs have also showed unexpectedly dubious, even negative, results on decisional conflict. 13,18–21 Few hypotheses have been proposed to explain these results. For example, in a study that tested a PDA for the surgical treatment of early breast cancer, although there was a lack of difference in decisional conflict between the PDA group and the control group, researchers observed that a subgroup of women who were initially leaning toward mastectomy or were unsure gained more from the PDA and had lower decisional conflict. It is possible that specific subgroups of middle-aged women may benefit more from our PDA than from the general information brochure. Therefore, there is a need for a larger trial that could evaluate the impact of the PDA on subgroups of women.
As no other RCT of a decision aid regarding the use of NHPs has been published, it is difficult to compare our study results with those of similar studies. However, in the field of menopausal women's health, a number of RCTs aimed at assessing the impact of decision aids on hormone replacement therapy (HRT) have been published. 20,22–25 Overall, when compared with other types of decision support interventions, they were usually shown to improve women's knowledge and perceived risks associated with HRT, enhance satisfaction with the decision, reduce decisional conflict and increase the congruence between subjects' personal values and their decision about using HRT. However, it is very important to emphasize that in contrast with our NHP decision aid, these other decision aids targeting menopausal women included published evidence on the probabilities of risks and benefits associated with potential outcomes of HRT. In our decision aid, probabilities were not provided because it was not possible to obtain published evidence for NHPs associated with ‘relieving’ menopausal symptoms. Therefore, our results support the need to provide more detailed evidence on outcomes of options to be able to improve women's knowledge and expectations of the benefits and harms of NHPs.
We acknowledge that women who enrolled in this study might not be representative of the larger population of middle-aged women. Despite the popularity of complementary and alternative medicine, researchers may face problems recruiting women for RCTs in this field. 26 More specifically, the decision to use these products may occur independent from the health-care system. Thus, it is possible that the impact of the decision aid that was tested could have been different in a more representative sample of middle-aged women considering NHPs. On the other hand, it has also been reported that women who use NHPs are more likely to use conventional therapies than non-users of NHPs. 27 Furthermore, the decision aid was designed to be used in preparation for discussing NHP decisions with health-care professionals, but this resource can also be relevant to those independently considering NHPs. Therefore, future studies testing the proposed decision aid in a more diverse population of women are worth considering.
We recognize that many factors may influence women's choices when considering the use of NHPs. Conflicting and/or lack of information, 4,28,29 lack of support or undue pressure from physicians, 1,28 costs of and access to NHPs, 1,29,30 personal experience, 30 menopausal health 30 and perceived effectiveness of NHPs for relieving symptoms 5 are among the identified factors that have been shown to influence women's choice. In this study, the decision aid that was tested had been developed after a carefully planned decisional needs assessment with the target population. 9 Therefore, we believe that the decision aid that was tested did address some of these factors.
Our study results also provide insight into the level of decisional conflict experienced by a group of middle-aged women facing the decision to use NHPs for menopausal symptoms. They showed that at baseline, a significant number of women experience clinically significant decisional conflict. This is important because a large proportion of participants (73% in both groups) reported currently using NHPs. This is not surprising, considering the definition of NHP encompasses a large number of products including vitamins. This suggests that although these women had made a choice, they were not entirely comfortable with it. Consequently, our study results suggest that there is a need to improve the current methods for supporting middle-aged women in deciding about NHPs for menopausal symptoms.
Finally, we observed interesting trends in some of the secondary outcomes. At two weeks, there were fewer uncertain women in the PDA group than in the control group (48–36% compared with 46–44%). This is congruent with the results from the meta-analysis of PDAs. 31 Interestingly, this also was associated with a greater increase in the number of women not wanting to use NHPs in the PDA group (9% pre versus 23% post) than in the control group (7% pre versus 15% post). We also observed that notwithstanding which group women belonged to, congruence between their preferred option and personal values was improved. This is important because a high-quality health decision is increasingly defined as being informed by the best available evidence and congruent with personal values. 7 Therefore, our results suggest that providing women with a PDA or a general brochure on menopause has the potential to improve the quality of their decision regarding the use of NHPs for menopausal symptoms.
In spite of its interesting findings, this study has a number of limitations. The majority of women taking part in the study were recruited in a clinical environment and a large proportion of those already had a strong predisposition towards an option at the start. Thus, it is possible that the results of this study do not translate to all middle-aged women. Also, although the superiority of the PDA over a general brochure was not supported, both brochures appear to help women increase their comfort with the decision that was made. However, it is important to note that the addition of a third group without any intervention (i.e. usual care) could have helped us to better determine the effectiveness of the PDA. 32
Nonetheless, the results of this study indicate that women in both groups experienced similar improvement in their decisional conflict after being exposed to educational interventions. Subsequent research is needed on how to implement any decision support intervention in routine clinical practice. 33 One barrier is acceptability of the intervention for practitioners. Given that compared with the general information brochure, the PDA was evidence-based, it is possible that physicians would be more receptive to such PDAs; but this hypothesis needs to be tested.
Footnotes
Acknowledgements
We would like to thank Monique Richer, who, at the time of this study, was Dean of the Faculty of Pharmacy, Université Laval, for facilitating the collaboration of pharmacy owners with this study, Claire Dubé of the Service d'information en contraception et sexualité de Québec who generously supplied the general information brochure, as well as all the women who agreed to participate in the study. This study was approved by the Medical Ethics Committee of the Centre Hospitalier Universitaire de Québec, Hôpital St-François d'Assise. Its trial registration identifier is NCT00325923 (
Competing interests
FL, DS, ST, AL and SD are involved in the development of PDAs in the area of women's health. However, they receive no financial gains.