
Abstract
The global epidemic of obesity continues to grow, with over 1.7 billion people worldwide classified as obese (body mass index; BMI ≥ 30 kg/m2). Of special concern is the population of older women, since women are more obese than men and gain weight early during menopause. Obesity with co-morbidities is the leading threat to women's health and longevity. Specific female co-morbidities, such as reproductive failure, urinary stress incontinence and disproportionate prevalence of serious diseases such as diabetes, cardiovascular disease and cardiopulmonary failure in addition to breast cancer and gynaecologic malignancies, reduce the fitness benefits grandmothers provide to the species by ensuring reproductive success of their children and health and survival of grandchildren. In fact, female life-expectancy is decreasing in industrialized nations. Non-surgical treatment for obesity itself is ineffective; currently there is not enough evidence to recommend weight loss medications for routine use in the elderly and calorie-burning exercise is problematic. Conversely, antiobesity surgery has been shown to be both effective and safe in the older adult population in studies that predominantly enrol women. Although the risks and benefits of antiobesity surgery performed in high-volume dedicated centres must be carefully weighed for each individual patient, the strong evidence for its safety and efficacy in reducing obesity-related co-morbidities and improving quality of life, with the potential to increase healthy life-expectancy, makes antiobesity surgery a viable treatment option for older obese women.
Introduction
Definition and prevalence
Obesity, from the Latin noun, obesitas, meaning fat or plump, is derived from Latin ob (over) and esus (past participle of edere, to eat). It is a symptom of overnutrition and is associated with numerous and serious chronic and fatal diseases. When exposed to overnutrition, humans are genetically susceptible to developing obesity, diabetes, hypertension, cardiopulmonary failure, hepatic and renal insufficiency, immune compromise and various malignant neoplasms, all of which contribute to a diminished lifespan. 1–3
Body mass index (BMI), expressed as weight in kilograms divided by height in metres-squared (kg/m2), is used to define ‘obesity’ as a BMI level of 30 and greater, whereas ‘overweight’ is BMI between 25 and 30. Earlier definitions of obesity were based on actuarial data demonstrating relationships between weight levels stratified for height and mortality in large general population samples. The nadir of the curvilinear relationship was termed ‘ideal’ or ‘desirable’ weight for height, indicating the lowest death rates. Greater weight or ‘excess weight’ was expressed as a percentage of ideal body weight. Surgeons treating severe (or ‘morbid’) obesity express their results as percent excess weight loss (%EWL), based on the faulty premise that weight standards for the never-obese are relevant for individuals who have been seriously overweight for several years. Optimal or healthy weight loss is not equal to 100% empirically, but this level is so rarely achieved, even by surgery, that meaningful actuarial statistics are not available.
By 2010 it is estimated that 12 million adults and one million children in the UK will be obese. 4 Currently, more than 30% of the US population is obese and in 2003–2006 approximately 16% of US children and adolescents aged 2–19 years were at or above the 97th percentile of the 2000 BMI-for-age growth charts. 5 The global distribution of obesity is presented in Figure 1. 6 There is an increased prevalence of obesity in older women; 39% aged 65–74 years in the US are obese. 7 It has been projected that by 2025 one-half of the US population will be obese. Women are more overweight and obese than men and gain weight as they age, especially after menopause. 8
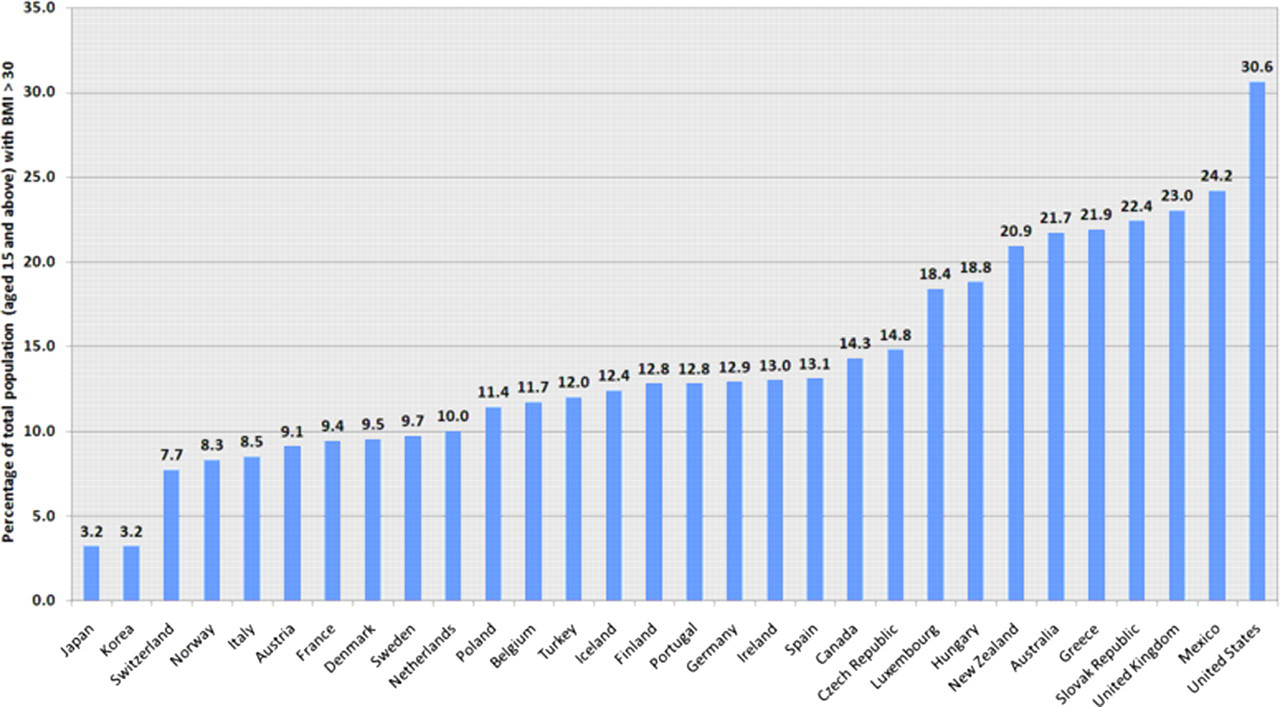
Percentage of obese adults (body mass index [BMI ≥ 30]) worldwide6
Consequences of obesity
Obese women enter menopause later than lean women, yet are at increased risk of metabolic complications of menopause compared with normal weight women and lean women. 9 The increase in prevalence of obesity in older women not only increases the number and severity of co-morbid conditions, elevating mortality and increasing the economic burden, 10,11 but also seriously decreases health-related and general quality of life, translating into a diminution of quality-adjusted life-years (QALYs). Although the BMI level associated with lowest all-cause mortality is slightly higher in older adults, the number and severity of obesity co-morbidities (e.g. metabolic syndrome, urinary stress incontinence, osteoarthritis, sleep apnea, cardiovascular disease, cancer and depression) 12 increase with age, as do the number of medications used to treat them. The time-course of weight gain and onset of obesity in women is important. In a group of adults with a mean age of 77 years, the risk of coronary heart disease (CHD) was assessed along with individual subjects’ weight histories. 13 Those with BMI greater than 27 in middle life had an increased risk of CHD later in life, but those who reached a BMI of 27 in old age had no such increased risk.
The pattern and timing of weight gain, along with the absolute weight and number of years spent being overweight or obese, affects the health risks, the co-morbidities and their reversibility through weight loss. This is of note specifically for multiparous women who gain weight during their child-bearing years and become obese as they fail to lose post- or interpartum weight. 14,15 Elevated postpartum weight becomes the baseline for addition of fat mass and redistribution to metabolically disadvantageous central adiposity as women enter menopause years later. 16
Taken together, the co-morbidities of obesity in older women are a serious threat to health and wellbeing. Less frequently addressed are the psychological consequences of obesity and its effects on quality of life. Depression, low self-esteem and negative body image are more common in women than men. In this context, obese women are more likely to delay critical health-screening tests, such as breast examinations, PAP smears and pelvic exams. 17 This avoidance of health monitoring can result in a vicious cycle of decline and late-stage disease in obese women already at high risk of metabolic and gynaecologic conditions. Higher BMI was associated with an increased incident risk of 10 out of 17 cancers studied in the UK Million Women Study, 18 and in a cohort of US women from the Iowa Women's Health Study, cancer of any type was 20% more common in subjects with the highest BMI compared with those with the lowest. 19
In addition to the increased prevalence of co-morbidities, mobility-related disability and cognitive decline, 20 there is evidence that obesity decreases life-expectancy, 21 an effect that decreases with older age owing to attrition of the most ill. Obese elderly women suffer from double jeopardy: both obesity and ageing have been seriously neglected by the medical profession leading to a dearth of evidence for developing safe, effective and timely treatment plans in this growing segment of the population. This review describes the state-of-the-art of antiobesity surgery and its relevance to female ageing.
Non-surgical treatment of obesity in ageing women
It is remarkably easy to lose weight: all methods work, from acupuncture and hypnosis to concoctions, drugs, electrostimulators, magnets and even diets. The problem is maintenance of weight loss. Although recent reviews of non-surgical treatment in respected journals present data on modest weight loss, 22,23 they affirm that long-term maintenance is ‘difficult’, stopping short of concluding that there is very little evidence for sustained weight reduction. Most published studies of diet, lifestyle changes or drugs describe periods less than 12 months, and it is exceedingly rare for patients to maintain medically significant loss beyond one year. 24,25
Many elderly people are unable to achieve even minimal physical mobility, let alone ‘exercise’ as a consequence of obesity, functional impairment or disability. Recommending hypocaloric diets to the elderly is controversial, especially for postmenopausal women in whom adequate consumption of vitamins and minerals, as well as protein, is of critical importance for musculoskeletal, neurological and cardiac health. The cognitive restraint associated with dieting and restricted food intake may induce psychological and translated physiological stress, as evidenced by elevated levels of urinary cortisol in pre- and postmenopausal women with high levels of dietary restraint. 26,27 This is of special concern for postmenopausal women, since elevated cortisol is associated with increased bone loss, decreased bone mass, calcium malabsorption and risk of fracture in older adults. 28,29
There are very few drugs approved for weight loss alone, and those that are approved pose problems for ageing obese women owing to the high prevalence and numbers of co-morbidities appearing with overweight (BMI 25–30), as well as side-effects and interactions. 30
Indications for antiobesity surgery
In contrast to the minimal and largely unsustained weight loss of medical management, antiobesity surgery has been shown to durably and effectively reduce excess body weight, obesity-related co-morbidities and mortality over the long term. 31–33 Commonly accepted indications for antiobesity surgery are based on the 1991 United States National Institute of Health guidelines, which specify that patients must have a BMI ≥ 40 kg/m2 or BMI ≥ 35 kg/m2 with one or more serious co-morbid conditions. 34 Although there are no age criteria, antiobesity surgery for older adults and adolescents is increasing along with the acceptability owing to increased safety from the availability of laparoscopic and other minimally invasive approaches, which are particularly beneficial for obese and elderly patients. The weight criteria are also broadening to include lower BMI limits due to the prevalence of co-morbidities at BMI 30–35 kg/m2 and the evidence that surgical intervention is safe and effective. 35,36
Risk–benefit analyses such as those routinely performed by physicians when they advise obese patients and their families are individualized and do not necessarily conform to personal or societal material cost–benefit analyses. Unless all parties recognize the seriousness of obesity and the relative safety of bariatric surgery, this modality will continue to be grossly underutilized. One of the difficulties in recruiting patients to prospective randomized trials comparing surgery with (combinations of) other modalities is the instinctive fear of surgery, and the perception of obesity as a cosmetic embarrassment rather than a serious disease. Beyond its serious co-morbidities, obesity compounds the difficulties of the menopause transition, partly through its intrinsic challenge of self-identity, partly through aggravating age-related disease, together resulting in an overall deterioration in general as well as health-related quality of life (HRQOL). It is distressing to read, as recently as 2006, in a review in a frontline obstetric and gynaecologic journal the recommendation: ‘Avoid operating on the obese woman if at all possible’. 37 Quality-of-life improvement is the primary objective of most women requesting antiobesity surgery. Antiobesity surgery can change the rate of unavoidable decline of vigour during senescence, a most powerful indication for its use.
Current antiobesity operations
Most antiobesity operations (Box 1) are performed laparoscopically in high-volume dedicated centres by experienced ‘bariatric’ surgeons (from Greek baros, weight). Two main effects are achieved: gastric restriction and diversion of nutrient flow, sometimes acting in combination or sequentially. 38 The restrictive procedures decrease the size of the stomach by creating a small pouch using a laparoscopically placed circumgastric inflatable silastic band (laparoscopic adjustable gastric banding [LAGB]; Figure 2a), which limits the amount of solid food that can be ingested at one time. This is the simplest of the operations and has been used more widely in Europe and Australia than in the USA.
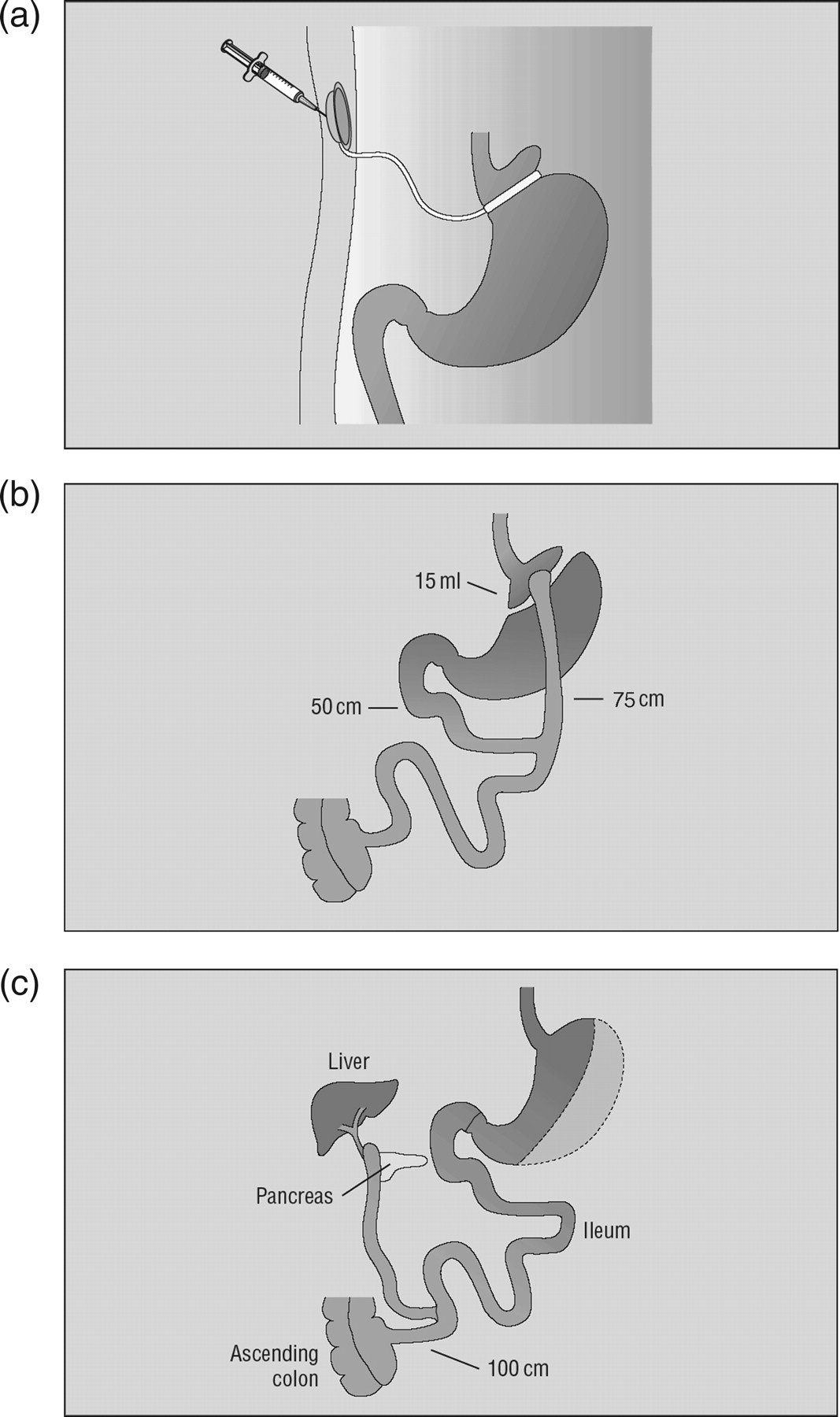
(a) Laparoscopic adjustable banding. Laparoscopic adjustable gastric banding creates a 15-mL gastric pouch causing delayed emptying of solid food through the narrowed passage. Adjustments are done by injecting or removing saline from the subcutaneous port. (b) Laparoscopic gastric bypass. Gastric bypass (Roux-en-Y gastric bypass) divides the stomach leaving a 15-mL pouch connected to a limb of jejunum varying in length. (c) Pylorus-preserving biliopancreatic diversion (Duodenal switch). Biliopancreatic bypass (BPD) consists of sleeve resection of one-third of the stomach and postpyloric diversion of the duodenum, creating a biliopancreatic duodenojejunal limb which empties into distal ileum. The proximal duodenoileal anastomosis creates an alimentary limb transporting food to the distal ileum where it encounters bile and digestive pancreatic enzymes.
Current laparo-endoscopic interventions for obesity
Restrictive operations
Adjustable gastric banding (AGB)
Vertical banded gastroplasty (VBG)*
Sleeve gastrectomy (SG)
Diversionary operations
Roux-en Y gastric bypass (RYGB)
Biliopancreatic bypass (BPD)*
BPD with ‘duodenal switch’ (BPD-DS)
Combinations of restrictive and diversionary operations
Banded gastric bypass
Other operations (investigational)
Intestinal interposition (ileal transposition)
Abdominal truncal vagotomy
Devices and endoscopic techniques (investigational)
Intragastric balloon
Gastric wall electrostimulator
Vagus nerve stimulator (VBloc®)
Natural orifice transesophageal surgery (NOTES)
Transesophageal ultrasonic vagotomy (TEVx®)
Intra-duodenal sleeve
*Being phased out
The diversionary operations, such as Roux-en-Y gastric bypass, are more complex, involving both creation of an isolated gastric pouch and bypass of the remaining stomach and varying lengths of jejunum (Figure 2b). This causes maldigestion and altered macronutrient absorption in addition to the gastric restriction imposed by the small pouch. Owing to stretching of the pouch and gastrojejunostomy in gastric bypass operations, some surgeons have concomitantly used adjustable banding to maintain the restrictive mechanism.
The most complex of all operations is biliopancreatic bypass or diversion (BPD), which uniquely among other obesity operations includes an irreversible element, viz. resection of approximately one-third of the stomach. The end-result is a gastric-restrictive operation causing maldigestion and significant malabsorption, not surprisingly achieving the greatest amount of weight loss, sustained for the longest period of time and requiring the most assiduous supplementation of vitamins and minerals. 39 The most recent version of this operation uses a pylorus-saving sleeve resection of the greater curvature, excluding the duodenum (‘duodenal switch’ [DS]), connecting the distal pylorus to the ileum (Figure 2c). 40 This operation (BPD-DS) is one of the most technically demanding of all laparoscopic procedures. It can be performed in two stages in the heaviest, highest risk patients: (1) sleeve gastrectomy, leading to initial weight loss and (2) enabling performance of DS.
Earlier, it was recognized that intestinal bypass operations cause weight loss through other mechanisms than simple malabsorption of calories. Indeed, decreased food intake contributed more to weight loss than dissipation of calories in the stool. These appetitive effects have been rediscovered after the isolation of several new gastrointestinal (GI) brain-gut peptides, foremost ghrelin, which is synthesized inter alia in the L-cells of the gastric mucosa, and is postulated to explain the greater weight loss achieved by diversionary operations. 41
Recent developments
The 50-year history of surgical treatment of obesity, perhaps more than any other field of surgery, is replete with controversy, failures and premature false claims by proponents of ‘gold standard’ operations of their making or choice. Given the multifactorial aetiology of this disease of chronic overnutrition, and its strong behavioural and even sociocultural underpinning, it is simplistic to believe that one procedure will suit all or even a majority of patients. Box 1, with its 15 interventions many of which have several versions with minor modifications, does not include the equally numerous abandoned procedures ranging from small bowel resection and jejunocolic bypass to gastric wrapping, oesophageal (sic!) banding and the ‘gastro-clip’ for partitioning the stomach.
Laparoendoscopic procedures have revolutionized the practice of surgery since the early 1990s through technological advances (although laparoscopy was first performed in women in 1910). The most recent addition uses a gastroscopic approach to achieve gastric restriction, and just as oophorectomy can be performed by entering the abdominal cavity via the GI tract, loops of intestine can be anastomosed to create diversionary operations. 42
It was early recognized that antiobesity operations have the potential to cure type 2 diabetes mellitus. 43–45 These findings were extended in large series of patients with gastric bypass followed for many years. 46 The rationale for widening indications for obesity surgery to younger patients 47,48 and to those in lower weight classes 35,36 was secondary prevention, which has been enabled by the significantly increased safety of antiobesity surgery. Most recently, the principles of diversionary operations have been expanded to treating diabetes in the absence of obesity 49,50 in analogy with the use of intestinal bypass to treat hypercholesterolaemia. 51 Owing to the long history of these operations, it is reasonable to assume that they will risk- and cost-effectively replace pharmacotherapy as they are incorporated into the standard of care for these serious chronic diseases.
Results of surgical treatment
Adverse outcomes
Safety/perioperative mortality
Current 30-day mortality rates for bariatric surgery in large series are 0.1–2.0% 52–54 depending upon the type of operation, experience of the hospital and surgeons, 55 and characteristics of the population being studied. Since minimally invasive laparoscopic procedures have only recently been disseminated, morbidity and mortality data are difficult to interpret, especially in governmental population registries that have failed to distinguish between open and laparoscopic approaches. Unfortunately, during the period of adoption of new, technically demanding operations, the ‘learning curve’ inflates the prevalence of adverse outcomes, whereas the results in institutions that developed techniques are not representative of standard practice. Common causes of early postoperative mortality included pulmonary embolism, anastomotic leak, myocardial infarction and bleeding or perforation. 56,57
Because the prevalence of chronic illness increases with age and both age and co-morbidity are linked with perioperative risk, one would expect operative mortality and morbidity to be increased in the elderly. 58,59 This was, indeed, the case during the era of open surgery, especially in population databases, 58,60 in contrast to personal series from centres of excellence. 61,62 No category of patients has benefitted more from laparoscopic approaches than the obese owing to the substantial reduction in operative trauma from large incisions. This benefit is magnified with increased age. In a comparison of severely obese patients in the US receiving Medicare who underwent antiobesity surgery, 30-day mortality in those ≥65 years of age was 1.55%, compared with 1.27% under 65, 63 although the older patients had an average of six co-morbidities compared with five among the younger ones.
Complications/side-effects
Less serious postoperative complications and side-effects also occur with the same frequency in older and younger patients. Although specific complications vary by procedure type, the most common among bypass operations have included venous thromboembolism, wound infections, bleeding, stenosis, ulcers, incisional and internal hernias, peritonitis secondary to intra-abdominal leaks, small bowel obstruction and pulmonary complications. 38,64 Depending on the skill and dedication of the caregivers up to 50% of patients may experience some degree of GI side-effects, such as nausea, vomiting and dumping syndrome. 65 Specific LAGB complications include band slippage, erosion, ulcers and pouch enlargement, which necessitates reoperation or conversion to a diversionary procedure in approximately 15% of patients. 66–68
Deficiencies
Long-term adverse effects are mainly manifested as deficiencies of vitamins and minerals, and are more common following diversionary and malabsorptive procedures (Box 2). Of particular importance for older women is the potential of calcium and Vitamin D deficiencies, which increase risk for musculoskeletal disorders, such as osteoporosis and fracture. Gastric bypass and BPD-DS are associated with deficiencies of Vitamin B12, folate, calcium and Vitamin D from malabsorption, as well as fat-soluble vitamin and protein deficiencies from rapid GI transit. 69 Persistent vomiting, usually as a side-effect of gastric-restrictive operations, can lead to thiamine deficiency and encephalopathy. 70 Adjustable banding has significantly reduced the risk of persistent vomiting, once again emphasizing the importance of diligent follow-up care. Adequate supplementation and monitoring in the outpatient setting can prevent or correct the majority of these deficiencies, and are significantly easier to treat than obesity itself.
Deficiencies after antiobesity surgery
Vitamins
B12, folate
A, D
B6, B1 (thiamine)
Minerals
Iron, Calcium
Protein
In summary, the preponderance of evidence demonstrates that laparoscopic bariatric surgery performed in dedicated centres has similar rates of side-effects and complications and of mortality in older patients as in younger ones. Let us now look at the benefits.
Benefits of obesity surgery
There are three objective, interrelated outcomes that are relatively easy to measure: weight loss, co-morbidity reduction and mortality. Important as they might be, overall patient satisfaction, expressed as QALYs, is considered as subjective and as such is often neglected by the medical profession and by insurers. However, for the patient weight loss is by far the most important outcome and the main reason patients request surgical treatment.
Weight loss
The magnitude of weight loss is highly correlated with the durability and magnitude of improvements in co-morbidities and ultimately the quality and length of life. Data comparing older and younger groups of patients suggest that while older patients attain substantial weight loss postoperatively, it is often slightly less than the amount lost by younger patients. Sugerman and co-workers compared patients over and under 60 years of age who underwent mostly open (non-laparoscopic) gastric bypass surgery between 1980 and 2003. 61 The older cohort was 78% female, 85% white, with mean BMI 49 ± 7 kg/m2, characteristics similar to those in the younger cohort. At one year after surgery, the older patients had 57% EWL compared with 65% EWL in the younger group. The older group maintained 49% EWL at five-year follow-up, whereas the younger group had 59% EWL.
A study comparing outcomes of LAGB in patients ≥60 years of age to those under 60 demonstrated mean reduction in BMI from 44 to 36 in the older group and from 45 to 30 in the younger group after five years. 71 Similar patterns were reported for laparoscopic RYGB, after which patients ≥60 years old reduced their BMI by 12.6, whereas those <60 years old reduced their BMI by 15.5 U. 72 Although older patients tend to lose less weight than their younger counterparts, the loss is still impressive and clinically significant. Indeed, the greatest effects are usually not in the raw number of BMI units or % EWL, but in the reduction of associated co-morbid conditions and increased patient satisfaction, leading to improvements in both health-related and general quality of life.
Co-morbidity reduction/improvement
All co-morbidities improve after bariatric surgery. The magnitude of improvement is a function of the number of years of exposure and the amount of weight loss, which strongly speaks in favour of early intervention. It is true that smaller amounts of weight loss, in the order of 10% of body weight, are beneficial 73 but maintenance remains a problem. Severely obese patients over age 65 treated medically compared with those who underwent antiobesity surgery exhibited an increased prevalence of co-morbidity after one year, whereas the operated patients reduced their prevalence of diabetes, hypertension, dyslipidemia and CHD. 63 Similar results were attained in a two-year study of LAGB not stratified for age 74 and with the 10-year nationwide SOS (Swedish Obese Subjects) study. 31
Mortality reduction
Several recent studies have convincingly demonstrated reductions in mortality, factoring in operative deaths. 32,33,60,63 The population study in Quebec Province clearly showed reduced use of health care and three-fold lower mortality in operated patients compared with age- and sex-matched patients over a period of five years. 75 Not only is antiobesity surgery safe and effective in older obese adults, it normalizes survival in a group that would otherwise have increased mortality as a result of both obesity and obesity-related diseases. This outcome is of special value for older obese women who commonly express a desire to live for their children and grandchildren as a reason for considering antiobesity surgery.
Quality-of-life improvement
The combination of obesity and older age significantly decreases quality of life. 76 Bariatric surgery patients, if given the choice, would prefer to be deaf, dyslexic, diabetic, have heart disease or bad acne rather than be obese; 90% preferred amputation or blindness to obesity. 77 This is pertinent to the discussion of antiobesity surgery for older obese women, because while age and gender are not reversible, obesity is. Operated obese patients reported improvements in multiple domains of HRQOL, including overall physical functioning and mobility, mental health, work capacity, confidence, self-esteem, social interaction, sexual activity and general satisfaction with life. 78,79 In a study of LAGB patients over age 65, 70% reported increased self-esteem, 48% had improved sleep and 72% reported a better outlook on life. In terms of satisfaction with the surgical outcome, 82% were happy that they underwent LAGB and 91% would recommend it to other older people. 80
A 60-year-old woman in an industrialized nation has a life-expectancy of approximately 20 years. After adjusting for years of life lost due to obesity, 21 an obese woman, however, will likely live only for 12 years. With the increased life-expectancy of patients undergoing weight loss surgery 32,33 and the associated reduction in co-morbidities, the quality of the years remaining increases in both health-related and general quality-of-life measures, in aggregate entailing increased QALYs.
Intergenerational benefits
Although older obese women have already made their genetic and epigenetic contribution to their offspring, grandmothers have the power to abrogate the intergenerational transmission of obesity. 81 Obesity surgery, by prolonging grandmothers’ postreproductive lifespan, allows them to exert ‘grandmother effects’, improving the reproductive success and fitness of the next generation, if not the entire species. 82–84 Grandmothers contribute both knowledge and material help. One crucial area of potential influence for grandmothers is breastfeeding, especially since recent trends in decreased breastfeeding and early introduction of supplemental foods for babies is associated with the epidemic rise in obesity. 85 However, significant educational efforts targeting grandmothers are required to offset maladaptive cultural/traditional beliefs undermining healthy practices limiting the rates of gestational weight gain, 86 early-life catch-up growth 87 and infant feeding practices. 88,89
Patient selection
By design antiobesity surgery substantially and mechanistically alters eating, the most fundamental and, for most people, rewarding of activities. It is precisely for this reason surgical treatment is more effective than other modalities that rely on various degrees of volition. Given the strong relationship between the severity of the eating disorder and the magnitude of excess body weight, the choice of operation should be predicated on the level of obesity. However, efficacy and safety are discordant and patients and physicians alike vary in risk aversiveness, bringing into question the necessity of the greater weight loss from malabsorptive and diversionary operations for older patients.
Owing to the lack of reliable outcome predictors in obesity surgery, in the late 1980s Kral introduced the concept of a staged approach to antiobesity surgery analogous to step-care strategies in the treatment of other diseases. Since the purely restrictive operations rapidly produce correction of co-morbidities, e.g. normalizing glycaemia within days of operation, it is reasonable to use a staged approach in the elderly obese, with their relative increased anaesthetic and operative risks. There are insufficient data to determine whether the risk of weight regain is smaller in older patients or whether there is any sex difference. In case of insufficient weight loss or regain, rescue operations via the laparoscopic approach pose minimal risk, especially with the benefit of the weight loss of the first stage.
Keeping in mind the severity of obesity and its co-morbidities and the impairment of quality of life, bariatric surgery should be considered as early as possible even in ageing patients. Treatment must be individualized and the preoperative evaluation and patient education, the surgery and the after-care must be delivered by an experienced, compassionate and competent multidisciplinary team.
Competing interests
None declared.