
Abstract
Objective
The objective of this study is to use the internet to survey the effect of menopause on women's experience of libido.
Study design
A questionnaire incorporating the Brief Profile of Female Sexual Function (B-PFSF) on a UK menopause website.
Main outcome measure
Questions on reduced libido, distress, level of help sought and treatment.
Results
Eighty-four percent of women (n = 2112/2527) felt that an active sex life was important. One thousand and fifty-one perimenopausal and 560 postmenopausal women reported reduced libido causing distress with 23% and 35% discussing this with health professionals. Eighteen percent perimenopausal and 30% postmenopausal women had tried non-testosterone hormone replacement therapy with 34% and 37%, respectively, finding it helpful. Testosterone was deemed useful in some perimenopausal (n = 6/17) and postmenopausal (n = 23/50) women. Twenty-seven percent premenopausal, 38% perimenopausal and 56% postmenopausal women reported vaginal dryness with 78% peri- and 87% postmenopausal women believing it a factor causing reduced libido. Twenty-two percent premenopausal, 28% perimenopausal and 46% postmenopausal women had discussed this with health professionals and 17%, 36% and 55%, respectively, were on treatment. Women in all reproductive epochs completed the B-PFSF (a validated tool for postmenopausal women only).
Conclusions
An active sex life was deemed to be important but many women were not seeking help for menopause-related reduced libido causing distress. For many, vaginal changes contributed to their symptoms. In those seeking advice, treatment was commonly not prescribed. Health professionals must ask appropriate direct questions to all women, especially as part of menopausal assessment. A need for the B-PFSF to be validated in non-postmenopausal women was also indicated.
Introduction
The website
A previous web-based survey reported that an active sex life is important to women in all reproductive epochs. It highlighted the fact that many women are not seeking help for vaginal discomfort despite the fact that prescribed treatment has good efficacy and that, for many, their confidence had been adversely affected and that excuses were being made to avoid intercourse. 5 Health professionals and women themselves have so far been reluctant to initiate these discussions and there is a growing body of literature highlighting the need to rectify this with examples of consultations. 6,7
Sexual health is a state of physical, emotional, mental and social wellbeing; it is not merely the absence of disease, dysfunction or infirmity. 8 The hormonal changes related to the menopause can adversely affect the lower genital tract, leading to problems such as vaginal dryness and irritation, which can reduce sexual satisfaction and desire. 9 Reduced sexual desire leads to distress and a negative domino effect on wider aspects of psychological wellbeing, relationships in general and marital/relationship satisfaction in particular. 10 An important sequelae of these physiological changes is hypoactive sexual desire disorder (HSDD) defined as ‘the persistent or recurrent deficiency and/or absence of sexual thoughts/fantasies and/or desire for or receptivity to sexual activity which causes distress or interpersonal difficulty’. 11,12
In this paper we report the results of an online questionnaire that included a validated screening tool for HSDD, 13 which allowed us to examine the effect of menopause on libido, the degree of distress a reduction in libido caused, level of help sought and treatment used among a group of computer-literate women accessing a menopause website.
Methods
A voluntary, online, convenience open survey, devised by independent clinicians with a special interest in the menopause to survey the effect of menopause on women's experience of libido, was offered on the patient-tailored menopause website
The data were collected in plain text in a password-protected database and exported as a‘.csv’ (comma-separated value) file into Statistical Package for the Social Sciences (SPSS v.14; SPSS Inc., Chicago, IL, USA) for statistical analysis. The chi-squared test was used to examine differences in two proportions, while the Mann-Whitney test examined differences in median B-PFSF scores between two independent groups (since the distribution of B-PFSF scores was skewed). No consent was obtained because no personal information was collected or stored and ethical approval was thus not required. Log file analysis was performed to prevent multiple entries being included. A session cookie and page redirection prevented a return to the questionnaire unless the user had closed down their browser and reopened it in a new session. IP (internet-provider) addresses were checked for duplicates and none were found. Table 1 provides further data, in keeping with the Checklist for Reporting Results of Internet E-surveys (CHERRIES). 14
Checklist for data completion
Results
A total of 3395 responses were obtained over the 38 weeks that the questionnaire was online. Of those responses, 2953 respondents completed self-classification of ‘menopause status’ and, of those, 2547 (86%) self-classified themselves as being either peri- or postmenopausal, the remainder being premenopausal.
Overall, in those who self-classified themselves as being either peri- or postmenopausal and answered the relevant questions, 84% (n = 2112/2527) answered ‘yes’ to the question ‘is an active sex life important?’ and 79% (n = 1978/2513) admitted to their libido being affected by the menopause transition with 86% reporting this was for the worse (n = 1782/2084). Eighty-one percent (n = 1519/1886) of women who experienced a change in libido said they were distressed by this with only 27% (n = 411/1496) of those women admitting to discussing the problem with a health-care professional.
In those women who were sexually active and answered the relevant questions, 78% (n = 1458/1877) felt their libido had been affected by their menopause with 86% reporting this was for the worse (n = 1292/1509). Eighty-two percent (n = 1129/1377) said they were distressed by this with only 27% (n = 299/1111) of such women admitting to discussing the problem with a health-care professional. Table 2 shows further stratification by different cohorts.
Responses of questions on libido, whether it caused distress and whether or not help was sought stratified by cohort
Postmenopausal sexually active women were more likely to discuss their loss of libido causing distress with a health-care professional than perimenopausal women (P < 0.001) and women who were single and not sexually active (both perimenopausal and postmenopausal) were more likely to discuss this symptom with a health professional than perimenopausal sexually active women (P = 0.022).
In the perimenopausal and postmenopausal groups, 1051 and 560 women, respectively, were distressed by their symptoms, 23% (n = 225/968) and 35% (n = 186/528) had discussed them with a health professional and 18% (n = 41/222) and 30% (n = 56/186) had tried non-testosterone hormone replacement therapy (HRT) with 34% (n = 14/41) and 37% (n = 20/54) in the peri- and postmenopausal women, respectively, finding it helpful. Testosterone was found to be helpful in 35% (n = 6/17), in the perimenopausal cohort, and in 46% (n = 23/50) in the postmenopausal group.
Thirty-eight percent (n = 510/1328) of perimenopausal and 56% (n = 288/514) of postmenopausal women admitted to dyspareunia secondary to vaginal dryness with 78% (n = 382/488) in the perimenopausal group and 87% (n = 246/283) of postmenopausal women believing it to be a factor in their loss of libido. Twenty-eight percent (n = 105/207) of perimenopausal and 46% (n = 111/243) of postmenopausal women had discussed this with their health professional and 36% (n = 37/104) and 55% (n = 60/110), respectively, were on treatment (Figure 1).
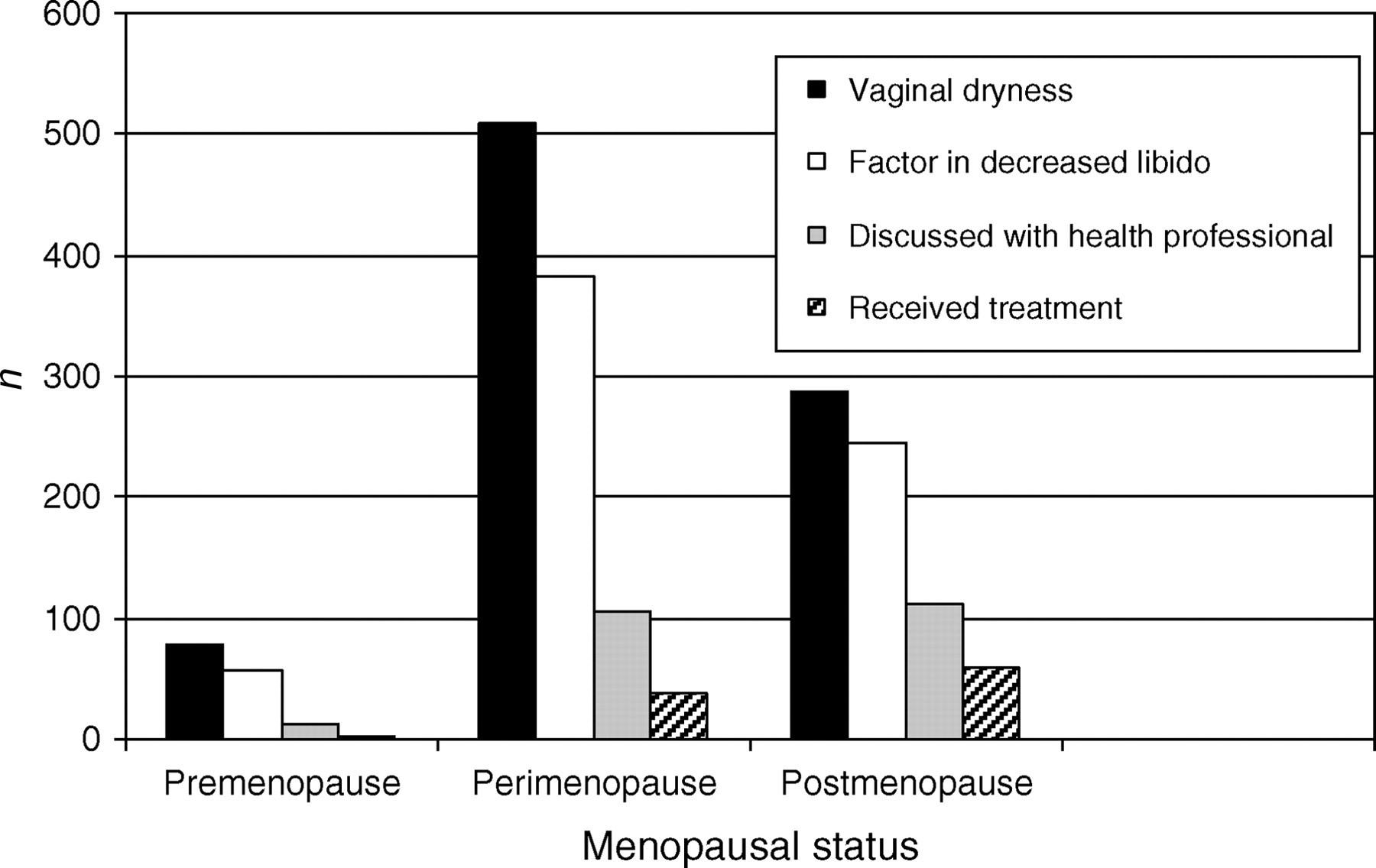
Number of women who experienced vaginal dryness, who thought it to be a factor in their decreased libido, who then discussed it with a health professional and finally received treatment
When stratified by age and menopause status, no perimenopausal woman <40 years old was on treatment for vaginal changes despite 78% (n = 18/23) of these women believing vaginal dryness to be a factor in their loss of libido.
In premenopausal women, 29% (n = 105/361) admitted to dyspareunia secondary to vaginal dryness with 63% (n = 82/130) believing it to be a factor in their loss of libido. Twenty-one percent (n = 17/80) had discussed this with a health professional and 17% (n = 2/12) were on treatment (Figure 1).
A total of 726 postmenopausal women completed all seven domains of the B-PFSF, of which 687 women self-classified themselves as having had either a natural or iatrogenic menopause. Women who had an iatrogenic menopause had significantly lower median B-PFSF scores compared with women undergoing a natural menopause (P = 0.003). Similarly, median B-PFSF scores in women who had an iatrogenic menopause and who were screened positive on the HSDD (score ≤ 20) were also significantly lower (P = 0.002) than women who had a naturally occurring menopause and screened positive (Table 3). Slightly more women screened positive in the iatrogenic menopause group compared with the naturally occurring menopausal women (P = 0.428).
Comparison of B-PFSF results in women self-classifying themselves as having either a natural or iatrogenic menopause
Of the 568 who were screened positive for HSDD, only 36% of the entire cohort (177/490) had discussed their lack of libido with a health professional. Of those prescribed treatment 37% (n = 29/79) of respondents had found non-testosterone HRT helpful and 43% (n = 16/37) had found testosterone preparations helpful. Over 90% (n = 322/356) felt vaginal dryness was a factor in their reduced libido and 40% (n = 173/430) had discussed dryness with a health-care professional with 51% (n = 87/170) being on treatment.
Despite the B-PFSF being validated as a screening tool for HSDD in postmenopausal women, women in all reproductive epochs completed the questionnaire (Table 4). There were significant differences in median scores across menopausal status categories with the postmenopausal women having significantly lower median scores (P < 0.001). Postmenopausal women were more likely to screen positive than both perimenopausal women (83% vs. 71%, respectively, P < 0.001) and premenopausal women (61%, P < 0.001).
B-PFSF results by menopausal status
Discussion
In their reviews of the Internet and the menopause consultation, Currie and Cumming highlighted the fact that the Internet lends itself not only as a medium for managing the menopause in the third millennium, 1 but also a medium for research and surveys outside of experimental settings with ‘real’ people. 15 The main advantages are that large volumes of data can be collected at low cost from a targeted population, where respondents are anonymous. The main disadvantage is selection bias (the volunteer effect), which limits generalizability. Our surveys potentially suffer from this bias and also, since they were anonymous, we cannot investigate the impact of sociodemographic factors on any of the issues. Another drawback is the problem of respondents not completing all the questions. We decided not to make all the questions compulsory as we thought it might be a disincentive to completing the questionnaire and respondents may abort the questionnaire, thus reducing response rates. To circumvent some of the criticism that can be levelled at web-based surveys, a checklist for reporting results of Internet e-surveys (CHERRIES) has been developed 14 and we have reported our results using these guidelines (Table 1).
There is no gold standard response rate for web surveys, although the current response rate (number of people filling in the questionnaire divided by those who viewed it) of 22% compares favourably with other online surveys where response rates were in the range of 20–40%. 16 One researcher 16 concluded that the relationship you have with your group of interest is the single most important factor in driving the response rate, not the administration method. The view rate (ratio of unique site visitors/unique survey visitors) for this survey was 6.8%. Our view rate is very acceptable especially as ‘it is not unusual to have view rates of <0.1% if the online survey is voluntary’. 14
In a computer-literate population of women accessing
However, loss of libido is multifactorial and comorbidities are not uncommon. Graziottin 18 cautions against the use of simple treatments ‘as a panacea for a complex condition with multiple contributing factors and comorbidities which need to be diagnosed and addressed in individual women’. The fact that non-testosterone HRT and testosterone replacement was helpful in some, but not all women, supports this conclusion that the management of this condition can be complex.
This survey would also confirm our previous conclusions from other surveys published in this journal 5 where we suggest that women may not be fully aware of the available treatments to alleviate their symptoms or that they may just be too embarrassed to seek help. Health professionals must therefore actively ask women about their sexual health.
The Women's International Sexuality and Health Survey suggested that HSDD is not uncommon particularly in menopausal women. 19 Dennerstein et al. showed that in a mail survey of women with sexual partners in France, Germany, Italy and the UK, the prevalence of HSDD was 7%, 9%, 12% and 16% in premenopausal women (20–49 years), natural menopausal women (50–70 years), surgical menopausal women (50–70 years) and surgical menopausal women (20–49 years), respectively. In this computer-literate population, we found a higher prevalence of women screening positive for HSDD using a validated screening instrument. These findings are to be expected and are accounted for in part by the self-selecting nature of the population. Nevertheless, these findings reflect a high unmet burden of not only pathology but also personal and social distress. Our survey showed that women who had an iatrogenic menopause had a higher percentage of women screening positive on the B-PFSF compared with naturally occurring menopausal women. This is in keeping with the literature, 19 although we did not observe a statistically significant difference.
Websites are being increasingly designed for interactive online assessments. The B-PFSF was designed for use in postmenopausal women. A potential problem of using questionnaires such as the B-PFSF online is that they are completed by people for whom they are not appropriate thus increasing the demand on already overstretched health services and potentially increasing unnecessary physician consultation. Scores in women who were not postmenopausal suggested a prevalence of pathology justifying validation of a screening tool in these groups to optimize physician consultation and patient quality of life.
Conclusion
An active sex life is important to women, and many women report libido being affected by their menopause, yet many women are not seeking help from health professionals for loss of libido sufficient to cause distress. In many women vaginal changes contributed to their loss of libido. Many do not seek help and in those that did, treatment was commonly not prescribed despite effective treatments being available. Health professionals must address libido issues by asking direct questions not only in the postmenopausal and perimenopausal groups, but also in premenopausal women. Loss of libido causing distress is multifactorial and single treatments must not be seen as panaceas. With increasing use of online questionnaires to aid self-help, it must be made clear to users who the questionnaires are designed for. There would appear to be a need for the B-PFSF to be validated in premenopausal and perimenopausal women.
Competing interests
The Menopause Matters website has been supported financially by several pharmaceutical companies. Procter & Gamble Pharmaceuticals Inc. have sponsored GC and HC to attend educational events.