
Abstract
Objectives
The objective of this study was to evaluate whether there is a relation between serum selenium levels and health-related quality of life (HRQoL) in overweight and obese postmenopausal women.
Study design
A cross-sectional study was carried out in 104 overweight and obese postmenopausal women attending a gynaecological clinic for their annual gynaecological examination.
Main outcome measures
Age, anthropometric parameters, educational level, smoking habits, serum glucose, insulin, lipid profile, C-reactive protein, folic acid, vitamin B12, homocysteine and selenium levels were determined, and the Cervantes Scale was used to evaluate HRQoL.
Results
Serum selenium mean value levels were similar in the different groups of HRQoL and there were no differences in the four domains of the Cervantes Scale. When women were classified according to serum selenium tertiles, higher levels of serum cholesterol, low-density lipoprotein cholesterol (LDLc) and triglycerides were found in women in the lowest serum selenium tertile.
Conclusions
In overweight and obese postmenopausal women, serum selenium level is not related to HRQoL but higher levels of cholesterol, LDLc and triglyceride values were detected in women in the lowest serum selenium tertile.
Introduction
Selenium is an essential trace element with a protective effect against some forms of cancer and cardiovascular disease; 1 furthermore, it regulates the inflammatory mediators and immune responses and is involved in the complex system of defence against oxidative stress through selenium-dependent glutathione peroxidases and other selenoproteins. 2 Oxidative stress of the brain is one leading cause of cognitive impairment associated with ageing, 3 and a relationship was found between serum selenium levels and cognitive functions. However, one study found that the highest declines in cognitive functions were associated with the lowest plasma selenium concentrations at baseline 4 and another more recent nine-year longitudinal study reported that cognitive decline was associated with decreases of plasma selenium over time. 5
Transition through menopause causes physiological and psychosocial changes, which could affect health-related quality of life (HRQoL). 6 The effect of the menopause on body fat distribution is unclear, but some studies suggest that it is associated with an accumulation of central fat and, in particular, intra-abdominal fat, 7 which is related to metabolic syndrome. 8 Obesity and metabolic syndrome could have a negative effect on HRQoL in postmenopausal women. 9 In a four-year prospective observational study, using the Medical Outcomes Study Short-Form 36 Health Status Survey to measure HRQoL, weight gain was associated with decreased physical function, decreased vitality and increased bodily pain. 10 Other cross-sectional studies found that obesity could have an influence on the psychical and sexual domains, 11 and an association between abdominal adiposity and hot flashes, particularly subcutaneous adiposity, was also reported. 12
Obesity and ageing have been associated with a fall in plasma selenium; 13 hence, several selenium-dependent functions could be affecting the HRQoL in obese postmenopausal women. At present not many studies exist on serum selenium levels and HRQoL during the menopause; hence the objective of the present study was to evaluate whether there is a relation between serum selenium levels and HRQoL in overweight and obese postmenopausal women.
Materials and methods
A cross-sectional study was carried out in 104 overweight and obese postmenopausal women attending a gynaecological clinic for their annual gynaecological examination. All these women had intact uterus and ovaries, were sexually active and were non-hormone therapy users. Menopause status was established one year after the last menstrual period and information on health status was obtained from medical history and physical examination. Trained personnel measured weight and height using calibrated scales and a wall-mounted stadiometer, respectively, with the subject in a standing position wearing light clothes and no shoes. Body mass index (BMI) was calculated as weight in kilograms divided by the square of height in metres, and categorized as less than 20 kg/m2 (underweight), 20–24.9 kg/m2 (normal weight), 25–29.9 kg/m2 (overweight) and 30 kg/m2 or higher (obese). Waist circumference was measured with an anthropometric tape placed directly on the narrowest point between the lower rib margin and the iliac crest on a plane perpendicular to the long axis of the body, while the subject stood balanced with both feet approximately 20 cm apart and both arms hanging freely. Hip circumference was measured at the widest circumference point around the buttocks and blood pressure was measured with a conventional sphygmomanometer following the recommendations of the British Hypertension Society.
Body composition was evaluated by bioelectrical impedance analysis using a multifrequency tetrapolar technique (QuadScan 4000; Bodystat, Douglas, UK). Percentage body fat was calculated using the manufacturer's software.
Blood samples were drawn by venipuncture between 09:00 and 10:00 hours after an overnight fast and glucose, insulin, lipid profile, C-reactive protein, folic acid, vitamin B12, homocysteine and selenium were measured. Biochemical method by graphite furnace atomic absorption was used for serum selenium measurement, and metabolic syndrome was diagnosed according to the criteria of the International Diabetes Federation Consensus Group. 8
The Cervantes Scale was considered for the present study as a tool to evaluate HRQoL as it was developed and validated for Spanish women between the ages of 45 and 64 years, and attempts to deal adequately with the relative importance of menopausal symptoms, psychical and sexual problems and couple relationships in HRQoL. It is a 31-item, self-reporting questionnaire comprising four domains: ‘Menopause and Health’ with 15 items covering vasomotor symptoms, health and ageing; ‘Psychical Domain’ with nine items, ‘Sexuality’ with four items and ‘Couple Relationship’ with three items. It ponderates age and educational level and it is short and easy to complete (about 7 minutes). The minimum score is 0 and the maximum score is 155 (from better to worse HRQoL), and the scores can be compared with reference values in younger women and women of the same age. Values more than 2 standard deviations (SD) above the reference score in women of the same age and educational level were considered as ‘severe symptoms’. Values between 2 SD and 1 SD above were considered as ‘high-problem level’. Those between ±1 SD were considered as ‘low–medium level of HRQoL’ and values lower than 1 SD below were considered as ‘good level of HRQoL’. 14 A sample of 104 women provides a power of greater than 95% for variance analysis of a two-sided significance level of 0.05, assuming a mean global Cervantes Scale score of 50.73 (SD 23.89) and a difference change equal to one half of an SD.
Groups of patients sorted out by HRQoL levels were compared to determine whether there were any differences in age, BMI, waist circumference, waist–hip ratio, body composition, lipid profile, C-reactive protein, homocysteine, folic acid, vitamin B12, metabolic syndrome, smoking habits, physical activity or educational levels, and Cervantes Scale mean values, using a T-test or χ2 test and Likelihood ratio and a variance analysis. In order to consider potential confounding factors, a multivariate analysis was also performed. Serum selenium mean values were compared with independent-samples T-test according to Cervantes Scale global score and the same analysis for the four Cervantes Scale domains was performed. Finally, a linear regression analysis was used to find a relation between Cervantes Scale global score and serum selenium levels.
All analyses used SPSS statistical package (SPSS for Windows, 12.0; SPSS Inc., Chicago, Illinois, USA) and the significance level was set at P < 0.05. The study design was approved by the Asturias Ethical Committee and the eligible women signed an informed consent form before joining the study.
Results
Total sample mean values of serum selenium levels were 107.2 ng/mL (SD ± 17.047) and no correlations were found between serum selenium levels and age, BMI, waist circumference, waist–hip ratio, fat or lean mass, smoking habits, physical activity, educational level, glucose, C-reactive protein, homocysteine, folic acid or vitamin B12 or metabolic syndrome.
Women classified according to serum selenium tertiles showed no significant differences in most of the measures, but higher cholesterol, low-density lipoprotein cholesterol (LDLc) and tryglicerides mean values were detected in patients in the lowest serum selenium tertile (Table 1). Patients classified according to four groups of HRQoL did not show significant differences in serum selenium means values, although it was observed that there was a tendency towards a steady decrease in serum selenium levels in the severe symptoms group, even when data were adjusted by BMI, smoking habits, physical exercise or educational levels (Figure 1). This tendency was also found in the four domains evaluated by the Cervantes Scale (Table 2). According to these data, no differences were observed in Cervantes Scale domain when women were arranged according to serum selenium tertiles (Figure 2).
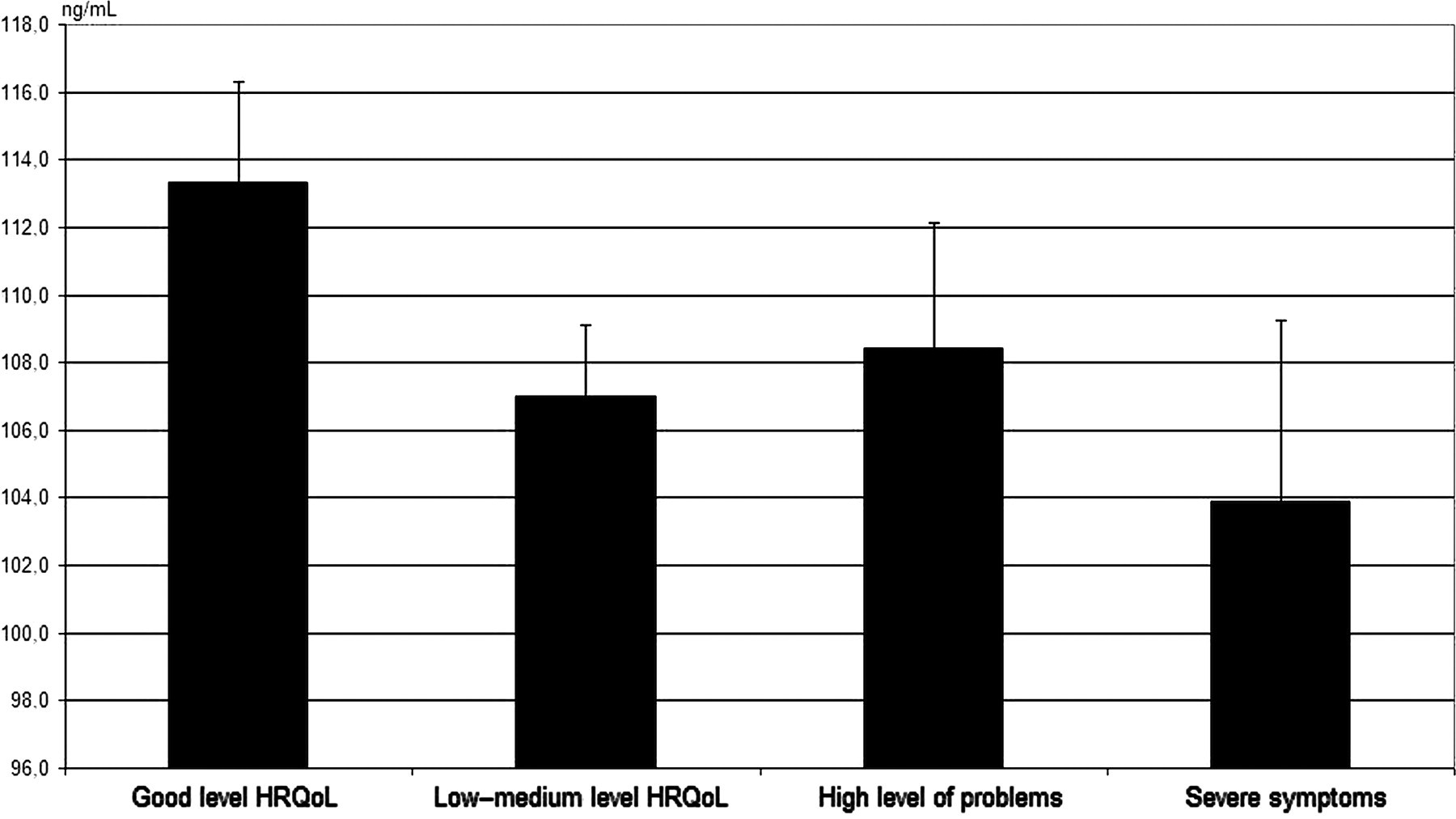
Mean serum selenium level found in women sorted out according to the health-related quality of life (HRQoL) Cervantes Scale categories
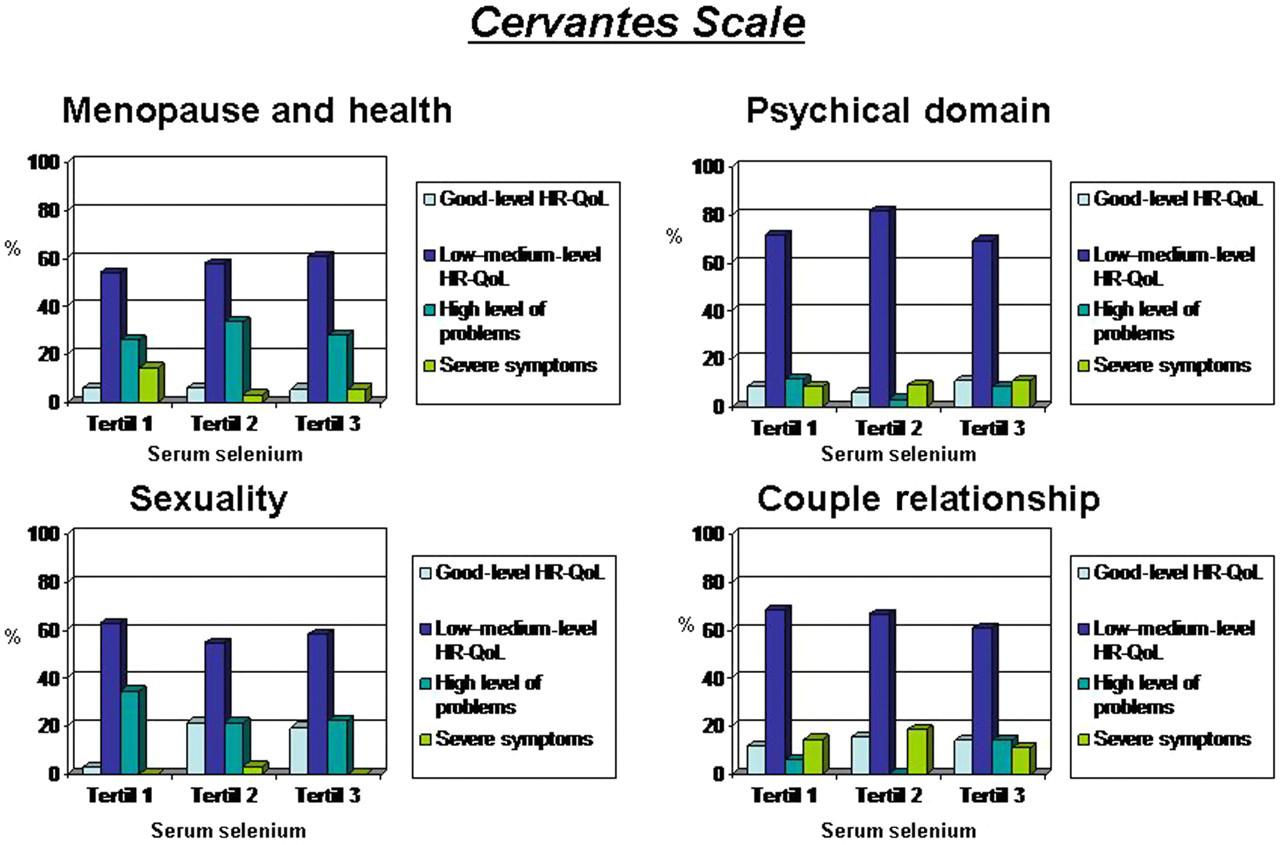
Percentage of women with good health-related quality of life (HRQoL), low–medium HRQoL, high level of problems and severe symptoms in the Cervantes Scale domains
Mean values and standard deviation (SD) for different parameters when women were classified according to serum selenium tertiles
*T1 versus T3, P = 0.049
†T1 versus T2, P = 0.029; T1 versus T3, P = 0.08
‡T1 versus T3 P = 0.021
LDLc = low-density lipoprotein cholesterol; HDLc = high-density lipoprotein cholesterol; NS = non-significant
Cervantes Scale mean serum selenium values and standard deviation (SD) for global score, menopause and health domain, psychical domain, sexuality domain and couple relationship domain according to their HRQoL level
HRQoL = health-related quality of life; NS = non-significant
Discussion
Some forms of cancer are the result of free radical oxidation that destroys or damages the part of DNA that regulates cell multiplication. Since selenium can protect from free radical oxidation, a possible role in the risk of developing these types of cancer has been reported. Several studies have shown that selenium could prevent from prostate cancer, colorectal cancers, cancer of the cervix, ovaries, bladder, oesophagus, pancreas, liver or lung malignancies. The anticarcinogenic effects of selenium compounds constitute intermediate mechanisms with several underlying chemical/biochemical mechanisms such as redox cycling, alteration of protein–thiol redox status and methionine mimicry. 15
Additionally, several studies have also suggested that dietary selenium deficiency may be associated with an increased risk of coronary heart disease and many studies suggest that selenium may reduce cardiovascular disease risk via several mechanisms. 16 For example selenium-related systems may decrease the oxidation of lipids and protect the vascular endothelium from damage due to oxidized LDLc particles. 17 Finally, selenium is essential for a healthy immune system. 18
Sex hormones and thyroid function could have some influence in selenium status in healthy young women. 19 However it is not clear if menopause hormonal changes have an effect on selenium levels. In a sample of healthy female workers, a lower level of selenium in erythrocytes in postmenopausal women was found, 20 but another cross-sectional study did not find significant difference in selenium level between healthy women of child-bearing age and healthy postmenopausal women. 21 In the present study most of the serum selenium levels were in the normal range and were not influenced by anthropometric parameters, metabolic syndrome, smoking habit, sedentary habits or educational level.
Karita et al. 20 in a sample of Japanese postmenopausal women reported a negative correlation between triglycerides and LDLc with levels of selenium in erythrocytes and that result is supported by our data. However, this result differs from data observed in a USA sample of men and women participating in the third National Health and Nutrition Examination survey, who found that elevated serum selenium was associated with elevated serum concentration of total cholesterol, LDLc, triacylglycerols, apo B and apo A-I. 22 At present, it is not possible to explain the reason or the potential mechanisms underlying these associations, but selenium may be one of the possible associated factors in lipid profile regulation after menopause.
One study had previously reported that C-reactive protein was inversely and significantly associated with concentrations of selenium and other micronutrients, 23 and other authors found that the level of total plasma homocysteine was inversely correlated to plasma selenium concentration in elderly people. 24 However, in our study these associations were not observed, but in Bekaert et al.'s research the design was different from the present study and the sample size was not calculated to evaluate differences in these parameters.
The term HRQoL is used to measure the effects of numerous disorders, short- and long-term disabilities and diseases in different populations and could be defined as the patients’ evaluation of the impact of a health condition and its treatment on daily life. Castelo-Branco et al. 25 in a sample of Spanish postmenopausal women reported a worse HRQoL when BMI was above 25 kg/m2, and pyknoid phenotype or androgenic fat distribution was present. We had also reported a higher level of problems on the HRQoL global score when metabolic syndrome was present in a sample of Spanish postmenopausal women with insulin resistance. 26 On the other hand, Gonzalez et al. 27 in a sample of elderly people residing in nursing homes reported that low serum concentrations of vitamins B6, B12 and selenium predict subsequent disability in daily living activities and serum selenium levels may affect the self-perception of health, although there is no evidence that selenium supplementation benefits mood or quality of life. 28 In this way, our data did not support the idea that low selenium levels were associated with worse HRQoL in postmenopausal women between the ages of 45 and 64 years.
We are conscious of the limitations of a cross-sectional study of HRQoL and the difficulties involved in the interpretation of our data due to the short age range in our sample limited by the Cervantes Scale design. Other possible implications for data evaluation are the fact that samples were taken from a gynaecological clinic, the women were healthy urban postmenopausal women, sexually active and that most of them had normal plasma selenium levels. Considering these limitations, our data suggest that serum selenium levels usually are in the normal range in overweight and obese postmenopausal Spanish women and they have no influence on HRQoL, although higher cholesterol, LDLc and triglyceride values were detected in patients in the lowest serum selenium tertile.
Additional research in this field will be necessary, especially with longitudinal design studies including a wider age range to ratify, as well as probe, the present data and to determine whether selenium supplements in diet or some specific antioxidant treatment could affect HRQoL.
Conclusion
Our study shows that obesity and excess weight do not appear to alter serum selenium levels in postmenopausal women, probably because the female population in our study group remained on a Mediterranean-style diet, with a higher antioxidant consumption. A Mediterranean-style diet is less common in North America & North Europe, and would tend to be high in saturated fat but low in total fat, fruit, vegetables and fibre leading to a low intake of antioxidants. Therefore, this may explain why a direct relationship between selenium plasma levels and HRQoL was not found in our study, but this should be studied in greater depth.
Footnotes
Acknowledgements
The present study was backed by a Health Investigation Grant funded by the Spanish Government (PI-O51616). The study design was approved by the Asturias Ethical Committee and the eligible women signed an informed consent form before joining the study.
Competing interests: None declared.