
Abstract
The menopause is an isolated event in a much wider process that was probably an evolutionary adaptation essential for survival in the Pliocene. As a reproductive strategy, it is largely vestigial in the 21st century, part of an era that has seen a doubling of the average human longevity compared with that of the past. This process commences as an accelerated decline in female fertility, usually from the fourth decade of life, culminating in a total cessation of reproductive capacity for those surviving. The 20th and 21st century sees a huge increase in the numbers surviving and the duration of that postreproductive life phase extending for decades. This extended period of what is essentially a hormone deficiency state is a recent phenomenon and by no means part of the natural history of the human individual. It is therefore not surprising to see a postmenopausal increase in the incidence of so many disorders above that expected by age alone. Recent reproductive patterns have seen increases in the birth rate and requests for fertility treatments among women in their late 30s and 40s. Many try for pregnancy but are unsuccessful. The genes that permit later reproduction and hence later menopause are therefore being preferentially selected. Slowly over generations we will expect to see the fertility of future 40 year olds increase and the age of menopause to extend much later into our, now, longer lives.
Keywords
Menopause
The menopause is the occurrence of a woman's last menstrual bleed prior to a phase in her life, the postmenopause, which results from a primary ovarian failure. This ‘menopausal event’ can occur at any time, but is usually regarded as premature if it is prior to the 40th birthday 1 and may occur well after the 50th or even 60th birthday, with the average being 51 years. 2 This average age does not seem to vary significantly between ethnic groups and has been largely unchanged since recorded history. 3
This ‘menopausal event’ is the outward manifestation of a process that starts in the mid-30s. Reproductive capacity of women, as in men, peaks in late teens and early 20s with a slow decline through late 20s and early 30s. In fact, many of our functions peak between mid-20s and mid-30s, as is reflected by the peak age of performances among athletes. There is some variation from activity to activity (sprinters compared with rowers) but this age range reflects the peak in the life we would have expected in our longer past as humans living a ‘traditional’ prefarming lifestyle.
In men the slow decline in reproductive capacity parallels the other aging processes through the late 30s and 40s. The term ‘reproductive capacity’ reflects the multiple functions required to achieve reproduction. In men, the figures for both erectile dysfunction 4,5 and sperm quality illustrate this. Interestingly, the decline is seen in semen volume, sperm motility and sperm morphology but not in sperm concentration. 6 These male reproductive functions fit with our ‘traditional’ lifestyle life-expectancy.
Traditional populations, whose hunter–gatherer lifestyle continues, are diminishing with exposure to the industrialized outside world. The very study of them is difficult without contaminating their society with modern influences. Nevertheless, studies have been undertaken; three such groups have been studied extensively. 7–9 These are the Ache of South America and the !Kung and the Hadza, each from different parts of Africa. At the time of the cited studies, they still lived close to their traditional ways. With regard to longevity, a high infant mortality depresses the average life-expectancy at birth to only 38 years for Ache, 31 years for the !Kung and 33 years for the Hadza. Nevertheless, on reaching maturity, the probability of surviving past 45 years is 0.79 for the Ache, 0.66 for the !Kung and 0.71 for the Hadza. Survival to 60 years occurs but is unusual. It is interesting to note that the proportion of adult females over 45 years is 36% in the Ache, 31% in the !Kung and 29% in the Hadza. Unlike our Western society, men have a greater longevity than women. Human biological functions fit with this sort of life-span. There is a gradual alteration in the contribution that individuals in their mid to late 40s make to the community; less than a quarter of the population survives much past 50 years.
We know, of course, that the natural history of a woman's fertility is different from a man's. The mid-30s see a rapidly increasing decline in women's fertility. The mechanisms of this are primarily to do with the oöcyte. Ovarian responsiveness to gonadotrophins declines with age but this is clearly not the only mechanism. 10 There is growing evidence that apoptosis rates are involved 11 rather than the, rather facile, ‘limited quantity of eggs running out’ view, which was never very convincing. However, the mechanism has other facets. Our patients know well about increasing chances of Down's syndrome with age, but they might not know that chromosome 21 is not the only chromosome to be subject to non-disjunction. Aneuploid embryos are less likely to implant and produce a pregnancy in the first place but if they do they are more likely to miscarry. Embryo aneuploidy rates rapidly increase through a woman's late 30s and 40s and so seem to be part of this accelerated process of decline. The zona pellucida gets ‘harder’ with age, 12 which may have an impact both on fertilization but also on embryo hatching. The zona pellucida surrounds mammalian oöcytes. It is involved in sperm binding and acts as a species-specific sperm barrier. After fertilization, the zona reaction (‘hardening’) prevents polyspermic fertilization and provides protection of the preimplantation embryo as it passes through the Fallopian tube. A combination of lysins produced by the cleaving embryo or the uterus and physical expansion then reduces the zona thickness again in preparation for hatching. This process may also be induced by in vivo ageing, which correlates with implantation rates that are inversely related to advancing female age. Hence, failure of the embryonic zona pellucida to rupture following blastocyst expansion has been put forward as a possible contributing factor in implantation failure. 13,14
It is evident that the oöcyte-based mechanism of the process is complex, as is so often the case with evolutionary adaptations. All these oöcyte factors contribute to the accelerated decline in women's fertility.
The oöcyte, then, is the source of the climacteric, the menopause and the postmenopause. The role of the rest of the ovary, the hypothalamus, the bones, the lipids inter alia are all secondary.
Few of the Ache, !Kung or Hadza survive to reach menopause and fewer survive to suffer the longer term effects of estrogen deficiency.
The so-called anatomically modern humans are said to have evolved 120,000–150,000 years ago. 15 Between then and now we, Homo sapiens, have only recently had a different life experience. In light of this, two things need consideration. Most important is how we counsel our patients. The other is related to understanding why this defined inevitable postreproductive phase has evolved. An understanding of this can help us inform our patients.
Evolution
It is established, then, that a woman's reproductive ageing differs not only from a man's but also differs from the other biological functions by way of a rapid decline from the age of 35 to a state where the occurrence of pregnancy is effectively zero. This absolute and universal fact is unique to humans among primates. 16 While some might argue that individual macaques, marmosets and baboons and an occasional chimpanzee have been shown to reach a stage of primary ovarian failure, 17–19 a thorough reading of the literature makes it clear that these occurrences are not what is seen in humans. As explained the accelerated decline in reproductive function followed by a brief period of primary ovarian failure in a few survivors is the 150,000-year human experience and remains so for those living the traditional lifestyles. To take one of the above examples, the macaque, the observed ‘menopause’ occurs around the age of 27 years. Captive, protected primates, like humans in industrialized countries, live considerably longer than their natural lifespan. Only 10% of free macaque females survive to 13 years and none beyond 18. 20 So when medical anthropologists refer to the uniqueness of the human menopause, it is truly based on sound evidence (Figure 1). It is not surprising then that the reason for this has been sought. It is thought that this understanding can help with directions of research as well as counselling patients.
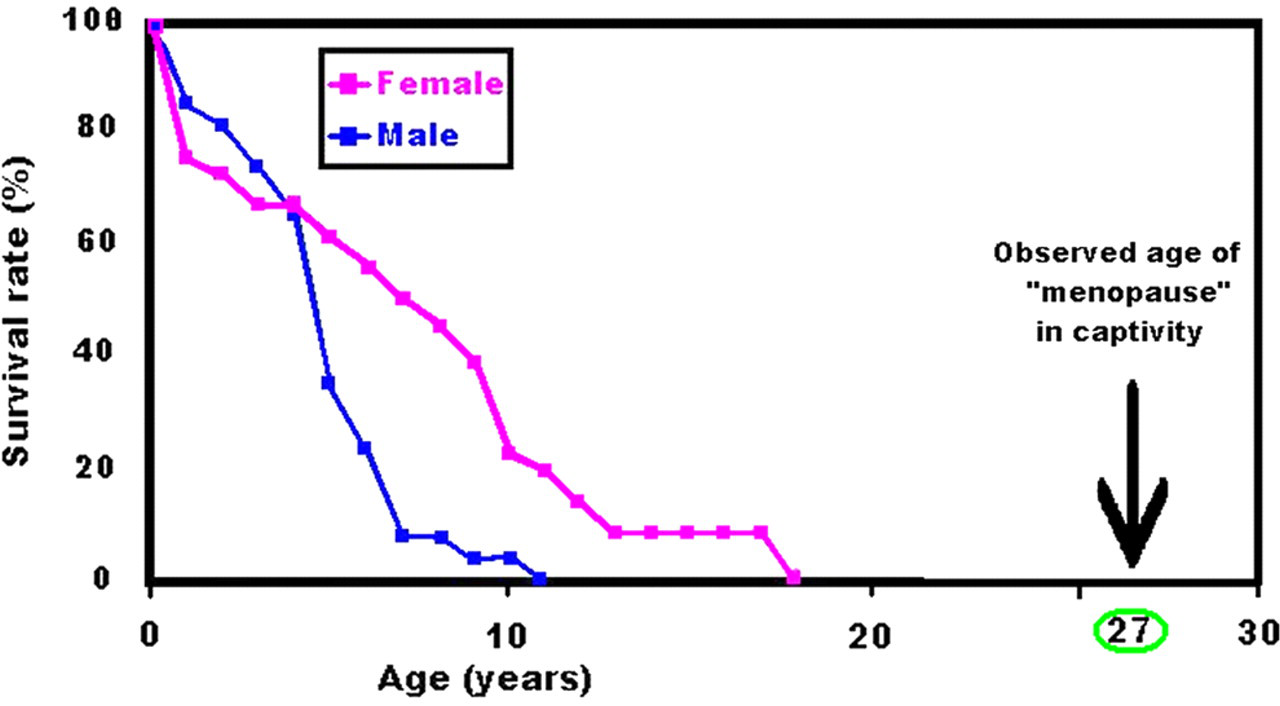
Survival of Rhesus macaques in the wild (Adapted from Takahata et al., 1998 20 )
When Kristen Hawkes 21 described what she calls the ‘Grandmother Hypothesis’, she described the result of many years work living with the Hadza, who live in Northern Tanzania near Lake Eyasi. The men hunt in small groups on the savannah with occasional success. As a result, the proportion of the diet provided by women's foraging is high and body weight is particularly sensitive to variations in those foraging habits.
Hawkes' finding, in brief, was that a weaned toddler's weight is directly proportional to the time its mother spends foraging and that a woman's foraging time increases with her baby's age as he/she becomes less demanding. After the arrival of a new infant, there is a statistically significant reduction in the foraging times of the nursing mothers. She went on to look at the other relatives. She noted an association between the weaned children's weight and their grandmothers foraging time and that those times significantly increase when their daughters are nursing a new infant. There is, therefore, a statistically significant relationship between the grandmother's foraging effort and a positive effect on their grandchildren's weight. Moreover, she noted similar but declining relationships with more distant relatives such as aunts. The older women are shown to support their grandchildren by freeing their daughters to care for the subsequent baby. However, the adaptation is not the menopause, since the grandmother is not herself essential; she is part of a team, a cohort of available female helpers. The adaptation is the declining reproductive efficiency through the 40s, when their daughters are most fertile. The menopause is an endpoint, but it occurs because of the accelerated decline. Indeed, a protracted menopause has considerable disadvantages as we know.
The timing of this adaptation is also proposed as it is not seen in other primates. 22 In particular, it does not occur in our nearest relative, the chimpanzee, Pan Troglotytes (in particular the bonobo, Pan paniscus). Therefore, it seems likely that the evolutionary pressure that led to this occurred sometime after ‘we’ parted company from our common ancestor; that was around 6 million years ago (mya). Over this time, there were a number of adaptations, not least bipedalism. 23 However, the events between 3.8 and 2.8 mya, an era known as the Pliocene, seem the most likely. Australopithecus afarensis was the dominant hominin 3.8 mya. This ape's celebrity was feted in 1974 with the discovery of an almost complete skeleton by Don Johanson's team. They nicknamed her ‘Lucy’ after a Beatles song that was playing in their campsite on their return. 24 She was about 1.2 m tall and would have been a mainly frugivorous ape that, perhaps also, scavenged insects and remnants of carnivorous predators' kills living in what is now the Horn of Africa in dense rainforests. The fossil record of the million years in question shows a diversification of this hominin line (Figure 2), which suggests a severe survival pressure that required attempts at various adaptations.

Diversification of hominin line in the Pliocene (Reprinted from
Palaeoclimate can be studied using marine dust and glacier samples. Oxygen isotopes on earth are largely 16 O with some 18 O. Water made up of 18 O is 11% heavier and so evaporates less easily and precipitates more easily than that made with 16 O. The ratio of oxygen trapped in glaciers and in benthic foramina shells (benthic foramina are protozoans with a tiny shell enclosing an ameboid body) can indicate the palaeoclimate. Such studies have clearly demonstrated that the earth as a whole was getting cooler and drier over the million years in question. Moreover, geological evidence in the Danakil Depression, one of only two ‘mid oceanic rifts’ to pass through land, suggests that this coincided also with geological activity that was elevating what we now call the Ethiopian Highlands. This elevation of the Horn of Africa was occurring at a time when Planet Earth, as a whole, was cooling, probably due to orbital periodicities round the sun. The rainforests with their plentiful food supply gradually gave way to what is now and has been for 2 million years, savannah. 25 Among the changes seen in hominins, generally, was an increase in body and brain size. The change in brain size was particularly marked over that million years. 26
The whole picture, then, is one of trade-off of marginal advantages with a price to pay (Figure 3). The altered environment demanded adaptation. Brain size increased to aid food acquisition. Childhood lengthened to enable training to add gearing to the intelligence. This demanded greater nutrition as well as lengthening the period of juvenile dependency and hence vulnerability. Of course, obstetric performance also suffered with the larger infant head, as there was a limit to the increase in pelvic girdle without adverse effect on mobility. The acquired benefit of long life and larger body enabled the flexible response of seasonal foraging, including digging and hunting in the face of not being able to outrun any quadruped prey. 27
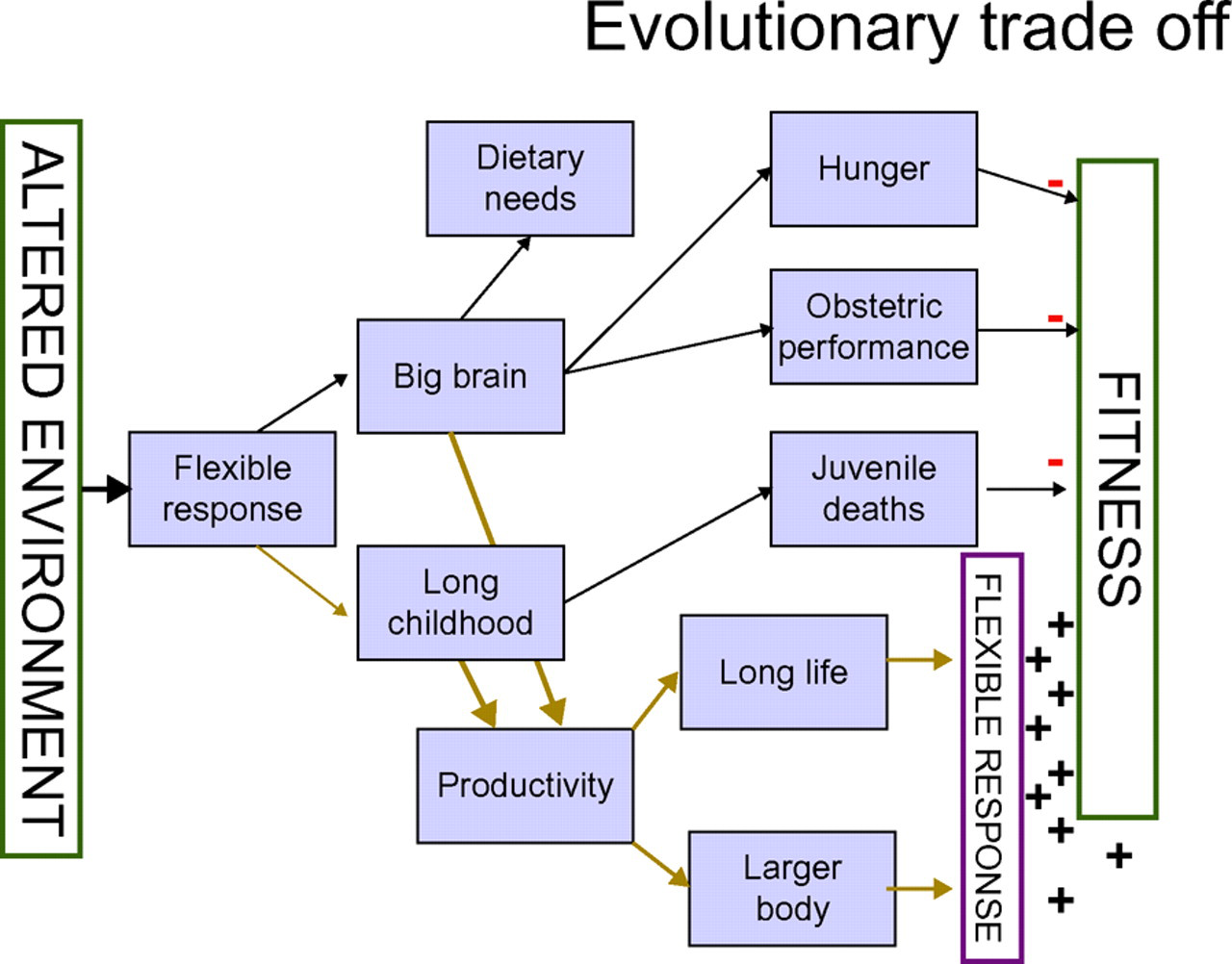
Part of the Pliocene evolutionary trade-offs
It is easy to see how the benefits of a cohort of older relatives with no recent children of their own would be of considerable survival advantage. Declining fertility through the fourth and fifth decades of life provides that cohort.
Changing cultures
The menopause happens. It is an inevitable result of being a human female. However, there is nothing ‘natural’ about experiencing it for 30 or 40 years. What is natural is a rapidly declining female fertility through the fourth decade of life. The birth rate in England and Wales (Figure 4) is rising more rapidly among the 35–39 age group than any other. 28 The average age of women treated for fertility continues to increase and is now over 35 years. 29 So society clearly accepts that this ‘natural’ aspect of our life can be regarded as worthy of ‘treatment’, or, rather, correction to 21st century society's needs.

Live birth trends by mother's age (Adapted from Office for National Statistics, 2007) 28
With regard to the postmenopause it is transparent that the most ‘natural’ way to replace nature's missing estrogen must surely be with estrogen. However, is ‘natural’ really what is wanted? With antibiotics, clean food and drinking water inter alia, our lifespan and disease profiles are far from natural. The real questions are:
Just how dangerous is 30–40 years of estrogen deficiency? Is estrogen replacement for that time more, less or equally dangerous? Is there any alternative now or possibly in the future that is even safer?
There are no clear answers, but the columns of this and other journals explore them in every edition.
We know little of estrogen deficiency as an intervention. That women with long-term estrogen deficiency do have a reduced risk of breast cancer and of thrombosis seems not to be in doubt. 30,31 Neither in doubt is the associated increased risk of osteoporosis and heart disease (estrogen lowers lipids). 32 The risk of untreated menopause is considerable since heart disease and osteoporosis are far commoner than breast cancer. Consider, then, that the decline in bone density accelerates in the absence of estrogen at a faster rate than age alone would predict. Octogenarian women would be expected to have stronger bones if they had had estrogens than if they had not. Whether that reaches the threshold that has been set for the label ‘osteopaenia’ or ‘osteoporosis’ in any individual cannot be reliably predicted at 50. That individual will however be less likely to sustain a fracture had she had the estrogen.
Estrogen replacement will logically reverse this picture of breasts and clotting versus bones, heart inter alia. Therefore, it seems likely that there is an overall benefit to long-term estrogen replacement even before the benefit of both the reduction in bowel cancer 33,34 and the cognitive benefits 35 are considered.
When large studies such as the Women's Health Initiative produce counter intuitive results, the lay press over-react 36 and the medical world tears itself apart. 37–39 Hormone replacement therapy should be discussed with patients and decisions made on an individual's balance of risk and benefit and not algorithm and rigid protocol. Even if there was outstanding evidence supporting widespread use of estrogen replacement, it would still be a matter of personal informed choice taken by the patient with the guidance of her clinician. It seems that it is cost-effective 40 so National Health Service and health insurance provision should be justified, but it does remain a personal decision of the patient.
That personal decision is usually driven by the shorter term symptoms that are familiar to us and which respond so well to therapy. The matter that seems to concern patients is of course survival and those big studies that attract so much media attention have a reassuring message that is often ignored. The overall global survival in the long term seems to change very little between the treated and the non-treated groups, 34 so the decision to accept treatment is truly a lifestyle choice between a hormone profile compatible with 21st century living or retaining the vestigial hormone patterns of our past.
The coming centuries will see the biggest change in the evolutionary development of Homo sapiens since we took up farming over 10,000 years ago. As 21st century women delay reproduction to their late 30s and beyond, 28,29 there are many who cannot achieve pregnancy. Age of menopause and reproductive decline is genetically driven. 41,42 Those who succeed are clearly increasing the successive generation's gene pool of those with later onset of reproductive decline. It is likely therefore that the coming centuries will see successive generations of women for whom fertility decline occurs later and, as a result, age of menopause increases.
Our life experience is rapidly changing and menopause is only one aspect of this. The challenge for the academics is to arm clinicians with reliable data to enable sound advice for patients. This means proper analysis of counter intuitive results before publication. The challenge for the pharmaceutical industry is to find products that can give women the benefits of estrogen without the risks.
Competing interests: None declared.