
Abstract
Background
Less advantaged social classes usually have unhealthier lifestyles and have more difficult access to health resources. In this work we study the possible association between poverty and the prevalence of obesity and oophorectomy in a population of postmenopausal women.
Design
Cross-sectional observational study.
Objective
To study in a population of postmenopausal women in poverty the possible differences in the prevalence of obesity and oophorectomy, and to compare some other gynaecological data: age at menarche, age at menopause, fertile years, number of pregnancies, breastfeeding and the use of hormonal replacement therapy (HRT).
Method
All patients were interviewed personally. A questionnaire was used to find out about their lifestyles and the medication they were taking. Their medical records were reviewed to confirm the existence of some diseases. A complete physical examination was performed with every patient. Weight and height were measured with the patient dressed in light clothes. Blood was obtained in a fasting state in order to carry out some analyses. Poverty was defined according to the Spanish National Institute of Statistics criteria.
Results
We enrolled 1225 postmenopausal women; 449 (36.6%) were under the threshold of poverty, defined by the Spanish National Institute of Statistics. Postmenopausal women in poverty had higher body mass index (29.2 ± 4.8 versus 27.0 ± 4.7 kg/m2 P < 0.001), and a higher prevalence of obesity than postmenopausal women not in poverty (44.2% versus 24.3%, P = 0.001). The prevalence of oophorectomy was also higher in women in poverty (32.7% versus 27.2%, P < 0.04). Women in poverty had had a greater number of pregnancies (3 versus 2, P = 0.001). They also showed a higher rate of breastfeeding than women in medium and high social classes (65% versus 59%, P = 0.037). There were no statistically significant differences between the groups in either the age of menopause or fertile years, nor in the use of HRT.
Conclusions
Postmenopausal women in poverty have higher levels of obesity, and also a greater prevalence of oophorectomy than women of medium and high social classes. They also presented a higher rate of breastfeeding and a greater number of pregnancies than those women not in poverty.
Introduction
Poverty has become a huge public health problem. 1 The recent increase in the number of women heading poor households has led to an increasing feminization of poverty, which is a change in the levels of poverty biased against women or female-headed households. More specifically, it is an increase in the difference in the levels of poverty among women and men or among female versus male and couple-headed households. 2,3
Against this backdrop, women in poverty also have reproductive health needs exacerbated by early marriage, lack of access to family planning, malnutrition, lack of prenatal care, failure to recognize obstetric emergencies and inaccessible health care. 4
Poor women tend to be more obese, to have more medical conditions, such as hypertension and diabetes, to be more likely to be stressed or depressed, and to smoke cigarettes and use illicit drugs. 5
Nevertheless, there are differences in these clinical patterns depending on factors such as their ethnicity or country of residence. In Spain, access to health services is equal and free for the whole population without consideration to the economic status of the patient. Medication is available at no cost to nearly all the population over 65 years old and hospital expenses are totally free for everyone. Because of this, we formed the hypothesis that there would be no differences in the gynaecological history of postmenopausal women living in poverty compared with postmenopausal women of medium and high economic classes. To test this hypothesis, we carried out the study described here in a population of postmenopausal women in poverty, living in the Canary Islands, in Spain, in Europe, in order to assess the characteristics of their gynaecological and obstetric history and to compare them with a group composed of women not living in poverty.
Methods
Subjects
Between January 2006 and January 2008, 1225 consecutive first-time outpatient postmenopausal Caucasian women were enrolled in some epidemiological studies and followed up in our unit. 6–8 They were all referred from their general practitioners and were aged between 45 and 85 years. Postmenopausal women were defined as those who had had their last menstrual period at least one year ago, in accordance with the clinical definition of the World Health Organization. 9 Those women receiving treatment for a malignancy, currently taking medication likely to influence skeletal metabolism or the interpretation of results (i.e. calcium supplements >500 mg daily, estrogens, progesterone, calcitonin, corticosteroids, anabolic steroids or bisphosphonates) and those with known malabsorption were excluded from the study. A flowchart of the enrolment of the patients is shown in Figure 1. It would appear that there might be potential for bias. All subjects were informed about the aims of the study and gave their written consent. The study was approved by the Ethics Committee of the Gran Canaria Insular University Hospital.
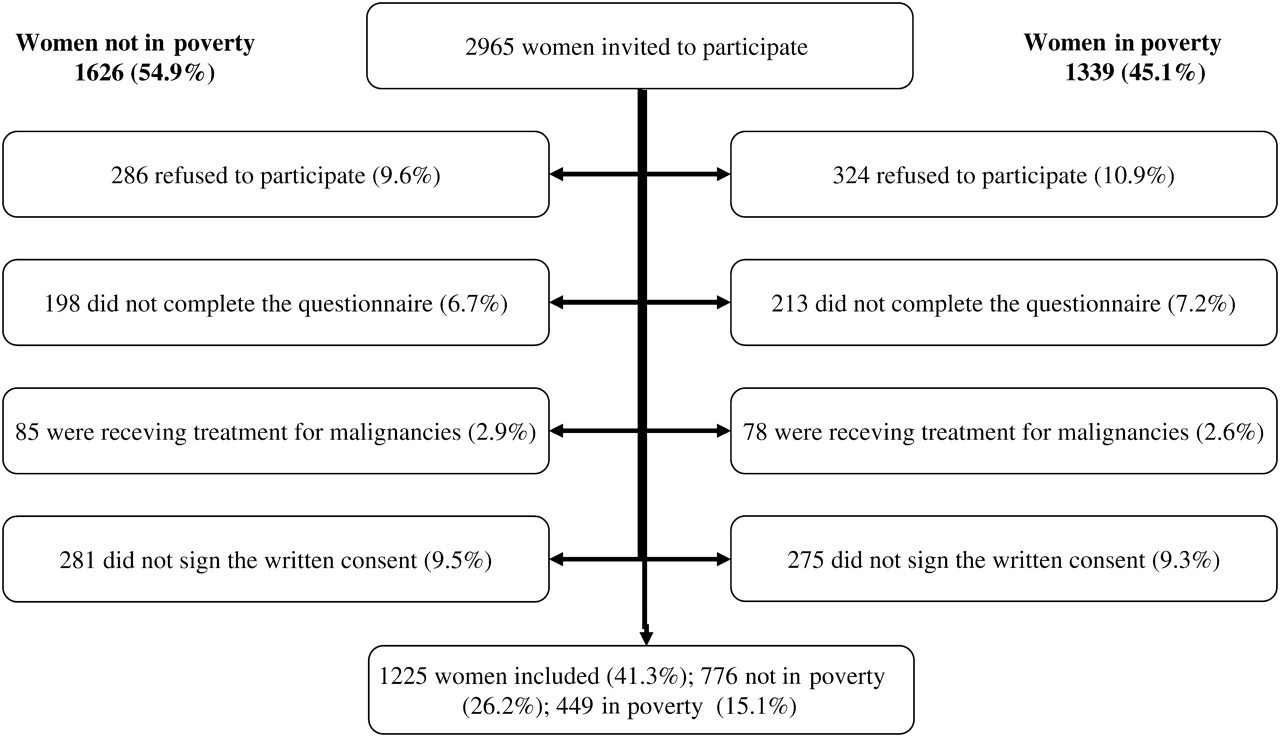
Flowchart of the women included in the study. Percentages are calculated from the total women invited to participate (2965)
A previously validated and detailed questionnaire concerning health, diet, drug use, lifestyle and reproductive history was obtained prior to examination. 10 A complete physical examination was performed. Height and weight were measured to obtain the body mass index (BMI) of each subject. Estimated calcium intake was assessed using the methods described previously. 11 The socioeconomic status (SES) of the participants was established after a personal interview, following the criteria of the Spanish National Institute of Statistics, which defines a one parent family with an annual income lower than 6346.8 Euros as living in poverty. 12
Statistical analysis
The categorical variables were summarized as frequencies and percentages and the continuous ones as means and standard deviations when the data followed a normal distribution or medians and interquartile range when they did not. The percentages were compared using the chi-square test, the means by the t-test and the medians by the Wilcoxon test. Those variables that showed independent association with poverty were then entered in a multiple logistic regression analysis. A selection was carried out using a retrospective method based on the Akaike's information criterion. For selected variables, we use the additive logistic regression to obtain the non-linear effects of continuous variables on the outcome. 13 For the resulting model the adjusted odd ratios of the selected factors were obtained and the significance was estimated by means of 95% confidence intervals. Statistical significance was set at P < 0.05. Data were analysed with the SPSS statistical program (16.0, SPSS, Chicago, IL, USA).
Results
Table 1 shows the baseline characteristics of the population studied. Women were classified into two groups according their SES: Group I (in poverty) was composed of 449 women with low SES, whereas 776 women were classified as not being in poverty (Group II). Women in poverty were older, heavier and shorter than those not in poverty. Because of this, all the comparisons were performed after adjusting for age and BMI. Current calcium intake was similar in both groups.
Basal characteristics of the population studied
BMI = body mass index; IQR = interquartile range
*t-test
† χ 2 test
‡Values are expressed as frequencies (percentages) and means (±SD) or medians (IQR)
§Wilcoxon test
Table 2 shows the gynaecological data of the women who participated in the study. Women with low SES had the menarche earlier than those not in poverty (13.4 ± 1.9 versus 13.1 ± 1.9 years, P < 0.01). There were no statistical differences between the groups either in the age of menopause or in the number of fertile years. Women in poverty had a higher number of pregnancies than those not in poverty (3 versus 2), and a higher number of abortions: 25.9% of women in poverty had had at least one abortion and 14.5% more than one, while in women not in poverty 19.5% had had one abortion and 11.6% more than one, these differences being statistically significant in all cases.
Gynaecological history
HRT = hormonal replacement therapy, IQR = interquartile range
*t-test
†Values are expressed as frequencies (percentages) and means (±SD) or medians (IQR)
‡Wilcoxon test
§ χ 2 test
Breastfeeding was more frequent among women with low SES than those not in poverty (65% versus 59%, P = 0.037). There were no statistically significant differences in the use of hormonal replacement therapy (HRT) but the prevalence of bilateral oophorectomy was higher in women in poverty (32.7% versus 27.2%, P = 0.016).
Table 3 shows the additive logistic model of gynaecological variables that showed an independent association with poverty. They were: age at menarche (P = 0.012, odds ratio 1.09 [1.02; 1.17]), the number of pregnancies (P = 0.01, odds ratio: 1.17 [1.10; 1.24]) and body mass index (no linear effect) (Figure 2).

Odd ratios (95% confidence interval) for the poverty for every unit of increase of the body mass index
Additive logistic model of gynaecological variables with independent association with poverty
Discussion
The term ‘feminization of poverty’ was first used by Diana Pearce when she observed that poverty seemed to be becoming more of a female problem. 3,4,14 The magnitude of the problem is even greater in older, postmenopausal women and with the global economic crisis, with which people are struggling throughout the world, it will probably get worse. The first problem we faced in the study was the need of a clear definition of poverty. Despite expert consensus that SES is complex and multifactorial, most health studies that consider SES use a single socioeconomic variable measured at a single period and level. Occupation is frequently used as a measure of SES in Europe, 15–17 while income or education is more commonly used in the United States. In our study we have chosen the income as the definition variable, because the Spanish National Institute of Statistics has clearly established a ‘poverty threshold’ cut-off point. 12
Postmenopausal women in poverty in our study were of shorter height than women not in poverty. People at a higher socioeconomic level have better nutrition and this conditions an increase in height, as previously reported. 18,19 We also observed that women in poverty weighed more. Because of this and their shorter height, the BMI was higher in these women compared with those not in poverty. The mean BMI was 29.2 kg/m2 in women in poverty, a figure very near the definition of obesity (BMI ≥ 30 kg/m2); while in women not in poverty the mean BMI was 27.0 kg/m2. Consequently, the prevalence of obesity was 44.2% in women in poverty compared with 24.3% in those not in poverty. Similar findings have previously been described. 18–21
We found a higher prevalence of oophorectomy in postmenopausal women in poverty (32.7% versus 27.2%, P = 0.04). Socioeconomic factors are also related to variations in hysterectomy rates. Specifically, in the United Kingdom, 22,23 Denmark, 9,24 the United States, 25,26 and Australia, 27,28 this intervention has been observed to be more common among women of lower educational and income level. In the United States, the rate of hysterectomy was reported to be higher for black women than for white women. But on the other hand, in other studies, the opposite findings have been reported, and hysterectomy has been shown to be positively correlated with income in studies performed in Los Angeles (USA) 29 and Finland. 30
There were no statistically significant differences in the age of menopause of the women of our study. Existing research has yielded inconsistent findings on the relationship between adult social class and the menopausal transition. Several studies have reported an independent association between early age at natural menopause and low adult socioeconomic position, as measured by educational attainment, 31–34 income, 32 and occupation, 33 even after adjustment for current smoking, 31–34 or ever smoking. 32 However, other studies have shown no independent effect of adult socioeconomic position measures on either age at menopause 35–37 or age at perimenopause. 38
Surprisingly in our study, women with poverty showed a lower tobacco consumption than those without poverty. It has been widely described the association between tobacco consumption and lower socioeconomical level. 39,40 Nevertheless, in some particular group of women, tobacco consumption seems to be higher in women with higher socioeconomical levels. 40,41 This contrasts with the gradient seen in high-income countries. On the other hand, many studies in low-income countries, particularly in more recent years, found a social gradient similar to that of Western countries. 42,43
Incidence of perimenopause was 1.75 times higher (95% confidence interval [CI] 1.10–2.79) and the median age at onset was 1.2 years younger (44.7 versus 45.9 years) for women reporting childhood and adult economic distress compared with women reporting no lifetime economic distress. This suggests that adverse socioeconomic conditions across the lifespan, when measured in terms of economic hardship and low educational attainment, may be associated with an increased rate of entry into perimenopause. 44 Similar results were reported by Lawlor et al., 45 who found that the age at onset of menopause for women who had 9 or 10 adverse socio-economic indicators was on average 1.70 years (95% CI 0.36, 3.0) younger than that of women with none or only one indicator.
We found no differences in the patterns of HRT use in postmenopausal women regardless of their SES status (15.6% versus 17.7%, P = 0.381). The use of HRT has been classically associated with women of medium and high SES. 46–48 In a study performed in Italy, higher education was associated with an increased frequency of HRT use in comparison with women reporting no, or primary/middle-school, education. 49 Similar results have also been described in Norway, 50 the United States, 51 Spain 52 and the United Kingdom. 53
The causes of the feminization of poverty are varied and complex, as are any solutions. 1–4,14 However, experience suggests that, contrary to the above expectations, abortion may actually be a contributing factor, in addition to an increase in broken relationships, psychological difficulties, and substance abuse, abortion, a practice which is carried out exclusively on women, may put them at greater economic disadvantage.
We found that women in poverty had a greater number of abortions, either as a single abortion or repeated abortions. In the bibliography consulted, the abortion rate is much higher among the population of women who have already had at least one abortion, 54,55 and some studies have reported that the SES of women tends to deteriorate as abortion is repeated. 56
Low breastfeeding rates have been historically associated to socioeconomically disadvantaged mothers, mainly because of the little knowledge they have about its advantages. 57–59 Nevertheless, in our study, we have shown exactly the opposite findings. Women with low income breastfed more than those at medium and high socioeconomic levels (65% versus 59%, P = 0.037).
In conclusion, disadvantaged women have a higher prevalence of obesity and oophorectomy than women with no poverty and also have a higher number of pregnancies, and abortions and a higher prevalence of breastfeeding than those women from medium and high socioeconomic levels. Women in poverty showed no differences in age of menopause compared with women not in poverty and showed a similar use of HRT to those who were not in poverty.
The reason of this finding may be due to the fact of the characteristics of the Spanish Health Service, which is free to every citizen who is either retired or aged more than 65 years old.
Health authorities should take into account that postmenopausal women suffering from poverty are at high risk and subsequently have greater morbidity. This should lead to the development of simple and direct objectives such as programmes to reduce the high prevalence of obesity in these women.
Competing interests
None declared.