
Abstract
Premature ovarian failure is a relatively common clinical condition, and carries important long-term health consequences. Estrogen replacement is recommended to alleviate unpleasant hypo-estrogenic symptoms and reduce long-term health risks. However, the most suitable form of estrogen replacement, and the exact effects of no treatment, is unknown. Surprisingly, little research has been carried out in this area. We describe the design of an ongoing clinical trial that will address these issues so that we can begin to provide evidence-based care for affected women.
Keywords
Introduction
Premature ovarian failure (POF) is defined by the British Menopause Society as a loss of ovarian function before the age of 45. 1 It is estimated to affect 1% of women under the age of 40 and 5% under 45. 2 In the short term, a lack of estrogen can cause distressing menopausal symptoms. Over a longer time period, early estrogen deficiency causes bone loss and increased cardiovascular risk. 3,4 Women with POF have only a very small chance of becoming pregnant spontaneously, and the only effective fertility treatment available is oocyte donation. 5
Estrogen replacement is recommended in POF to protect against bone loss and cardiovascular disease and alleviate symptoms. However, the most suitable form of estrogen replacement is unknown and management is not currently evidence-based. This is acknowledged in most reviews on the subject. 1,6,7 In 2004, the RCOG Menopause and Hormone Replacement study group advised that research is needed ‘to develop and assess treatment strategies in women with premature menopause’. 8 No such study has yet been published. Currently, hormone replacement therapy (HRT) or the combined oral contraceptive pill (COCP) is commonly prescribed. HRT is considered to be more ‘physiological’, but some young women dislike taking a preparation which they associate with older women. The COCP contains synthetic estrogen at a higher dose but with a ‘pill-free’ week. It is often seen as more ‘peer friendly’. Some clinicians do not recommend a seven-day break when the COCP is used in POF, citing concerns that symptoms will recur; however, this is not evidence-based and has not been observed in our clinical practice or in the trial to date. Almost all COCPs contain 19-nortestosterone-derived progesterones and the COCP and HRT preparations chosen for use in this study contain the same progesterone component. They are also both commonly prescribed and are widely available. There are also a significant proportion of women who, despite adequate counselling, decline treatment as they feel it is ‘unnatural’ or are concerned about the safety or side-effects. To date, there have been no prospective studies in spontaneous POF investigating the quantitative effects on bone density of different treatments or no treatment.
Some countries use the cut-off of 40 rather than 45 to define POF. However, a woman who experiences POF at the age of 44 has eight extra years of estrogen deficiency compared with a woman who has her menopause at the median age of 52. She is therefore exposed to all the risks of early estrogen deficiency, including early bone loss. We therefore use the British Menopause Society's definition both in clinical practice and for this research project.
Aim
The aim is to investigate the preferred treatment for POF (HRT or COCP), and the effects of taking no treatment, over two years.
Design
Prospective open randomized controlled trial of women diagnosed with POF to investigate the effects of active treatment with HRT (Nuvelle) or COCP (Microgynon 30), and observation of patients who choose no treatment.
Primary outcomes are percentage change in bone mineral density (BMD) at lumbar spine and hip at two years.
Secondary outcomes are serum markers of bone metabolism and cardiovascular disease, ovarian function, menopausal symptom scores, depression score, quality of life and sexual function.
Sample size calculation
The target sample size is 90 (30 in each group). Assuming that the BMD change within each group varies with a standard deviation of 4%, 22 in each group is sufficient to detect a difference in the mean BMD change at two years between groups of 4%, assuming a 5% significance level and a power of 90%.
Thirty women will be recruited to each group to allow for dropouts. If complete follow-up is attained, 30 women in each group will provide a power of 90% to detect a difference in mean BMD change of 3.3% between the groups.
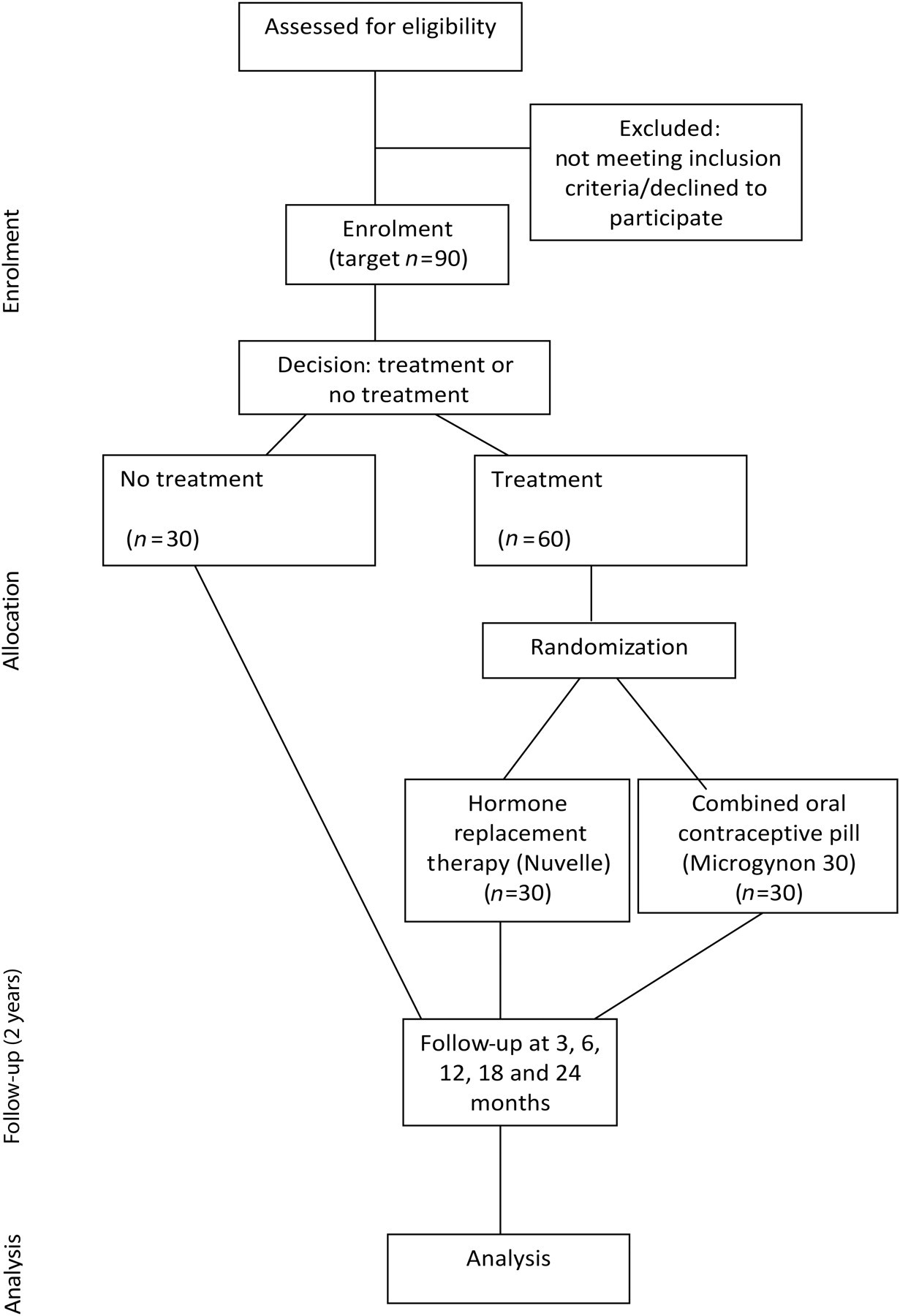
Flowchart of trial participants
Study outline
We aim to recruit 90 women aged 18–44 with a confirmed new diagnosis of spontaneous POF (2 follicle-stimulating hormone levels of over 30 IU/L) within the last 36 months. Participants choose whether to be in the ‘no treatment’ or ‘active treatment’ group. Those in the active treatment group are randomized to HRT or COCP (see Figure 1).
We are recruiting women from the POF, Menopause and Reproductive Medicine Clinics at Guy's and St Thomas' NHS Foundation Trust (GSTT); The Daisy Network (patient-run support group for women with POF), the Menopause Matters website and magazine, the British Menopause Society website and local general practitioners. The total recruitment period is expected to be approximately 18 months. Women will be enrolled into the trial as they are recruited.
Women with absolute contraindications to hormone treatment or a current desire for pregnancy are excluded from the active treatment group. The full inclusion and exclusion criteria are detailed in Table 1. Women are requested not to take any herbal/alternative medication or calcium/vitamin D supplements for the duration of the trial. Women currently taking hormone treatment are requested to have a two-month ‘wash out’ period prior to participation in the trial.
Inclusion/exclusion criteria
Following informed consent and confirmation of eligibility, the women have an initial assessment by medical examination, gynaecological assessment and a trans-vaginal ultrasound scan to assess ovarian volume and antral follicle count. Blood tests are taken for cardiovascular markers, markers of bone metabolism and markers of ovarian function. A DXA bone scan is also performed. The women are asked to complete questionnaires to assess menopausal symptoms, depression, sexual function and quality of life. See Table 2 for details of the assessment tools used for each outcome.
Methods of assessment of outcomes
Women who choose the active treatment group are randomized (using a secure randomization website) to HRT or COCP. They are aware of which medication they are allocated to and both are oral preparations. The HRT is Nuvelle (oestradiol 2 mg daily for 16 days, then oestradiol 2 mg with levonorgestrel 75 µg daily for 12 days). The COCP is Microgynon 30 (ethinylestradiol 30 µg/levonorgestrel 150 µg daily for 21 days, then a 7-day pill-free break).
Participants are seen at 3, 6, 12, 18 and 24 months. The questionnaires are repeated at each visit. The DXA bone scan, markers of bone turnover, cardiovascular markers and markers of ovarian function are repeated at 6, 12 and 24 months. Each woman is followed up for two years. Compliance with treatment is recorded. A telephone helpline is available for participants.
Screening tests and cardiovascular markers are analysed on an ongoing basis due to instability when frozen. The other samples (CTX, P1NP, AMH and Inhibin B) are stored at −80°C as frozen serum (CTX, P1NP and Inhibin B) or plasma (AMH) and will be analysed in one batch at the end of the trial to minimize variability. All samples will be analysed by GSTT Laboratories.
Data are collected on paper forms, which are kept in a locked secure room, and then anonymized and collated onto a customized secure database.
The trial is conducted in compliance with the principles of the Declaration of Helsinki (1996), the principles of Good Clinical Practice and in accordance with all applicable regulatory requirements including but not limited to the Research Governance Framework and the Medicines for Human Use (Clinical Trial) Regulations 2004, as amended in 2006 and any subsequent amendments.
Monitoring is performed by the KCL/GSTT Joint Clinical Trials Office.
Statistical analysis plan
The mean change in BMD at two years (primary outcome) between the two randomized groups will be compared using analysis of covariance, adjusting for the baseline level and for other major predictors of BMD. A similar approach will be followed for secondary outcomes.
Logistic regressions will be used to model the effect of randomized treatment on the proportion of women that maintain or increase BMD and the presence of serum markers for cardiovascular disease. Interaction tests will be used to identify subgroups of women with different treatment effects.
The non-randomized comparison between treated and untreated women will follow a similar sequence, with particular attention applied to selecting the best combination of confounders to adjust for. If there is a clear evidence of one randomized treatment being superior to the other, the inferior treatment group will be excluded from this analysis.
Discussion
We recognize that different clinics will have different rates of women who decline treatment and that to some it may seem unrealistic to recruit 30 women to a ‘no treatment’ group. In our POF clinic, estrogen treatment is initially declined by over half of women seen within 12 months of diagnosis. This is despite recommendation of estrogen replacement to all women (unless there are absolute contraindications) and adequate counselling about the risks of estrogen deficiency. Women entering the trial are given the same information, are aware that estrogen treatment is recommended and are free to withdraw from the trial at any stage. While we do not actively recommend the ‘no treatment’ group, the observation of these women provides a valuable opportunity to gather data on the natural history of POF, as well as providing a control group. To date, this group has the largest number of recruits. Clinicians should be wary of believing that they have a very low rate of women declining treatment as we have been approached by many women seen at other centres who do not currently wish to take treatment (and have not been using their prescription), but felt unable to communicate this to their doctor. These women often welcome the chance to be followed more closely for the duration of the trial.
Over this short study, there may be only small differences in BMD between the two treatment groups. This study will provide an important starting point but it is likely that larger and longer studies will be needed to fully answer the question of whether HRT or the COCP has a more beneficial effect on bone density in POF. Markers of bone turnover are more responsive following initiation of treatment and will provide further information on differences between the groups. More importantly, we are also monitoring other differences between the two treatments (i.e. sexual function, depression, quality of life, menopausal symptom control), which may influence women's treatment choices depending on their symptoms and concerns.
Unfortunately, since this trial was started, Nuvelle has been withdrawn from the market. However, we have secured supplies for the duration of the trial and therefore do not plan to change the HRT.
Summary
It is widely acknowledged that insufficient research has been carried out in this field and no research has addressed the question of the best treatment for POF, or fully quantified the risks of no treatment. In a patient-centred approach to health care, these data are vital to enable affected women to make treatment choices. This study investigates a wide range of outcomes of importance to women and will gather important preliminary data. We hope that it will facilitate a subsequent larger, multicentre trial to further evaluate the optimum treatment for this neglected condition. Future research would ideally evaluate ‘hard’ endpoints such as cardiovascular disease, fracture and breast cancer incidences in relation to different types of HRT and COCP.
Competing interests: None declared.