
Abstract
The bladder and its surrounding structures are rich in estrogen receptors and there are demonstrable physiological and anatomical changes that occur around and immediately after the menopause. The prevalence of many bladder symptoms, such as frequency, urgency and incontinence, does seem to increase around the menopause, but there is continuing debate over whether these effects are due to ageing, menopause or a combination of the two. The impact of the menopause varies with individual symptoms; stress urinary incontinence being associated more with estrogen deficiency than urge incontinence which seems to be more age-related. Both estrogen and progesterone have a variety of effects on the urogenital tract which are reviewed. Based on these effects, it could be anticipated that estrogen replacement would have a positive effect on bladder symptoms. However, the data are far from clear cut on this issue. It seems that topical estrogens do have some positive effects, particularly on symptoms of urgency, frequency and urge incontinence, the prevention of urogenital atrophy and in the prevention of recurrent urinary tract infections. The role of systemic estrogens is less clear cut with some studies even suggesting they can be associated with a worsening of some symptoms. The possible explanations for this apparent contradiction are explored, but based on current evidence, it would appear preferable to use vaginal estrogens rather than systemic as part of the management of menopause-related bladder problems.
Introduction
The menopause has a profound physiological impact throughout the body, which leads to changes in many organs and systems, and the bladder and lower urinary tract are no exception. While the clinical problems associated with the bladder and lower urinary tract are by no means exclusively a problem of the menopause, many women first present with bladder symptoms around or shortly after the menopause. This article reviews the role estrogen deficiency plays in the development of the principle bladder problems that are encountered in clinical practice and looks at their treatment with particular reference to the impact of hormonal intervention.
Prevalence of urinary symptoms
Urinary incontinence (UI) is nearly twice as common in women as it is in men and the prevalence generally increases with advancing age. UI is reported by between 12% and 42% of middle-aged and younger women and between 17% and 55% of older women, with between 3% and 17% reporting daily incontinence. 1 More specifically, the prevalence of UI in postmenopausal women varies widely depending on the definition of incontinence in each study, the population studied and the diagnostic tools employed. Data from the Medical Research Council (MRC) survey of National Health and Development cohort indicated that just under half of women aged 48–54 reported stress incontinence and about a quarter reported urge incontinence. 2
Although from a clinical perspective it has long been assumed that urinary symptoms are an integral part of menopausal transition, the actual relationship independent of ageing is far from clear. 3,4 A peak prevalence in mid-life for urinary symptoms including stress and urge incontinence has been reported by many studies. 5–7 While this would appear to implicate the menopause as one possible contributory cause, other studies have just found a steady increase in urinary symptoms with age. 8,9 Looking at individual symptoms, the prevalence of stress UI appears to peak perimenopausally (45–49 years), 10 while the prevalence of urge UI increases generally with age. 11
Epidemiological studies comparing pre- and postmenopausal women have found mixed associations depending on the symptoms and type of UI. 12,13 Thus, the impact of the menopause per se on urinary symptoms is controversial and the collection of accurate data is difficult. Ovarian activity fluctuates for many years before the menopause, yet the ‘menopause’ in epidemiological terms is often seen as a specific time point. This may be further confounded by delayed reporting of urinary symptoms. Many women put up with their symptoms for many years before consulting a health professional and association of symptoms with major life events like the menopause is variable. In Iosif's study of 2200 women aged 61, 14 70% of women with incontinence related the onset of their urinary symptoms to the menopause, but Barlow et al. 15 found that although nearly 50% of women aged 55–85 had had urinary symptoms, the majority did not relate them to the menopause.
Longitudinal studies should therefore provide us with the most accurate information, but here too the results are mixed. The SWAN study in Australia found no particular association between the prevalence of urinary symptoms and the menopausal transition. 16 However, further data from the MRC 1946 Birth cohort 4 indicates that women who become perimenopausal or who had been perimenopausal for more than one year were statistically more likely to have symptoms of stress UI than were postmenopausal women or women who remained premenopausal (Figure 1). Women in the cohort were divided into eight categories aged between 49 and 54 based on menopausal status defined by menstrual history (premenopausal, perimenopausal or postmenopausal). The highest prevalence (63%) of stress incontinence was in women who at the age of 54 had been perimenopausal for more than 12 months (peri–peri). The lowest prevalence (43%) was in women who were postmenopausal throughout (post–post). Going through the menopausal transition was not associated with any change in symptoms of urge or severe UI.
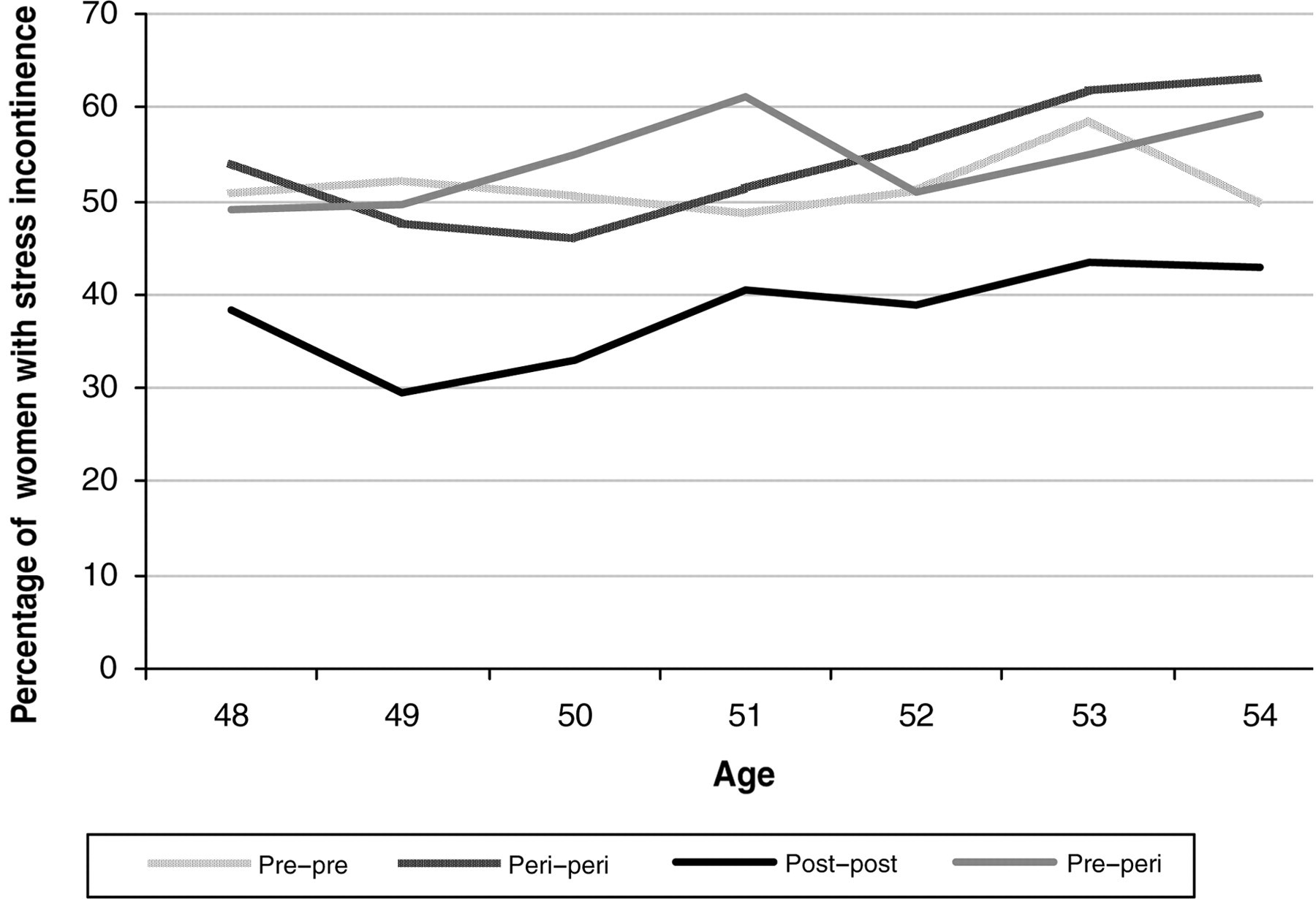
Percentage of women in each menopausal transition category with stress incontinence by age (n = 843). A detailed description of the categories is in the text (from Mishra et al. 4 with permission)
In summary, the menopause per se is not the main cause of either stress or urge incontinence, but probably does influence the prevalence at least of stress incontinence. It is conceivable that falling estrogen levels impact on the integrity of the pelvic floor due to urogenital atrophy and decreased collagen synthesis and is thus at least a contributory factor in the clinical presentation of urinary symptoms and incontinence. Equally, the presence of other menopausal symptoms may influence the reporting of incontinence symptoms around the menopause. The prevalence seems to decline after menopause, suggesting that women may learn how to manage their symptoms more effectively. Urge incontinence seems more related to age than menopausal status.
Hormonal influences on the lower urinary tract
Estrogen and progesterone receptors are found throughout the lower urinary tract, 17,18 which reflects its shared embryological origin with the lower genital tract. During the fourth to seventh weeks of development, the urogenital sinus separates from the cloaca and develops into the bladder and proximal urethra in the upper part and the distal urethra and the vestibule of vagina in the lower part. Within the lower urinary tract, estrogen receptors (ERs) are widespread being found in the epithelial tissues of the bladder, trigone and urethra, as well as supporting structures such as the pubocervical fascia, levator muscles and uterosacral ligaments. 19
Changes in lower urinary tract function after the menopause can be ascribed to a combination of age-related changes and loss of estrogen. Ageing results in gradual atrophy of the skin and mucosal surfaces, a decrease in skeletal muscle volume, a fall in smooth muscle tone and nerve degeneration, all of which will potentially affect the lower urinary tract. Histologically there is an age-related increase in fibrosis at the bladder neck, 20 reduced number of muscle fibres in the urethral sphincter 21 and reduction in muscle fibres within the pelvic floor. 22 Functionally, urodynamic studies have demonstrated that the bladder becomes less efficient with age with an increased bladder capacity, reduced flow rate and higher residuals. 23,24
Estrogen deficiency after the menopause leads to progressive atrophy of estrogen-sensitive tissues resulting in thinning of the vaginal and urethral mucosa and the trigone of the bladder and weakening of the supporting tissues and ligaments. The potential mechanisms by which estrogen deficiency may result in urinary dysfunction in postmenopausal women are listed in Table 1.
Possible mechanisms by which estrogen deficiency may result in lower urinary tract dysfunction
Effect of sex hormones
Further evidence of the role sex steroids play in postmenopausal lower urinary tract dysfunction comes from looking at the effects of estrogen treatment. Urinary continence is maintained by a complex interaction of a number of factors both intrinsic and extrinsic to the urethra. Urethral integrity depends on its epithelium, vascularity, elasticity, the tone of its smooth and striated muscle, and the collagen content and strength in surrounding supporting structures. Urethral closure pressure and functional urethral length both decrease with age.
24
Estrogens improve urethral closure pressure
25,26
that may be achieved by a number of mechanisms:
Estrogens improve the cellular maturation and proliferation of the squamous epithelium,
27
which may lead to an improved mucosal seal. Estrogens increase periurethral vascularity,
28
which contributes to about a third of urethral pressure.
29
Estrogens increase α-adrenergic tone and smooth muscle contractility.
30
Effect on connective tissue of supporting structures. Skin collagen content declines after menopause
32
and there is a correlation between skin collagen content and urethral length and closure pressure.
32
Estrogens increase collagen synthesis and turnover in periurethral tissues,
33
which may potentially weaken urethral tone. Animal studies suggest that estrogens may increase the amount of detrusor muscle fibres and thus overall lead to a decrease in the collagen/smooth muscle ratio in the detrusor and urethra.
34
Estrogens may increase the sensory threshold of the bladder.
35
Estrogens increase the neuromodulation function associated with sympathetic nerve density in the rat pelvis.
36
Estrogens have a direct effect on detrusor function resulting in reduced frequency and amplitude of spontaneous detrusor contractions,
37
possibly by reducing movement of extracellular calcium into the muscle cells.
38
In addition, there are a number of other reported effects of estrogen that may influence lower urinary tract function:
Progesterone
Although progesterone receptors are also expressed throughout the urinary tract, they are not found as consistently as ERs. 18 Progesterone appears to have an overall detrimental effect on lower urinary tract function being associated with an increase in irritative bladder symptoms, 39 worsening of urinary symptoms premenstrually 40 and during the combined phase of hormone replacement therapy (HRT). 41 The mechanisms are poorly understood and most of the limited data on the physiological effects of progesterone are related to pregnancy. 42 Progesterone appears to modify the blocking effect of estrogens on the responsiveness of the muscarinic receptors, thus increasing the β-adrenergic response. 43
Using estrogens in the management of lower urinary tract disorders
Estrogens clearly have an important physiological action on the lower urogenital tract and the patho-physiology of the impact of estrogen deficiency outlined above would suggest that estrogen treatment should have a beneficial effect on many of the conditions affecting the postmenopausal bladder. However, the evidence for the use of estrogen is far from clear and quite contradictory. Many of the studies are observational, have used varying preparations and different progestogens, inconsistent doses and routes of administration and have used various different outcome measures with inconsistent follow-up. Some of the more recent studies have tried to address these issues, but the true role of estrogens in managing the postmenopausal bladder is still unclear. Estrogens can either be administered topically or systemically as part of HRT and there does appear to be a differential effect.
Topical estrogen
Vaginally administered estrogens certainly improve vaginal atrophy and the associated symptoms 44 and the use of vaginal estrogens is increasing partly due to the concerns raised about the long-term safety of systemic HRT. Most of the randomized controlled trials (RCTs) comparing vaginal estrogen with placebo for the treatment of urinary symptoms in postmenopausal women have shown some symptom improvement; however, the overall numbers in these trials have been relatively small with a short follow-up of six months or less. 45 In an earlier meta-analysis by the hormones and urogenital therapy (HUT) committee, 46 topical estrogen was shown to be superior to systemic estrogens for subjective improvement of lower urinary tract symptoms including stress incontinence. A randomized double-blind placebo trial comparing a 25 µg estradiol vaginal tablet with placebo in 110 women with symptoms of frequency and urgency found a slight improvement in sensory urgency, but no benefit on other parameters. 47 A more recent RCT of 57 hysterectomized women, receiving either oral (conjugated equine [CEE]) or vaginal estrogens, found a significant improvement in urinary frequency and nocturia in both groups, but no significant change in urge or stress incontinence. 48 There appears to be no synergestic effect when topical estrogens are administered together with an antimuscarinic. 49
Various systematic reviews have all concluded that vaginal estrogens do seem to improve symptoms of frequency, urgency and urge incontinence to a varying degree; 45,46,50,51 however, there is little evidence for any continuing benefit once the treatment is discontinued. Recent NICE guidelines on the management of UI recommend the use of vaginal estrogens for the treatment of overactive bladder in postmenopausal women with vaginal atrophy. 52
Systemic HRT
Most of the systematic reviews have included both systemic and topical estrogens. Fantl et al. 46 reported an overall benefit for estrogen treatment with a subjective improvement in incontinence symptoms, but no objective improvement. This analysis highlighted the relative paucity of the data. Of the 166 papers published between 1969 and 1992, only six were controlled trials and 17 uncontrolled. Subsequently, a systematic Cochrane review in 2003 identified 28 suitable randomized trials on the effects of various HRT doses and preparations on UI. 50 Generally, the overall impression was of higher cure rates in the estrogen-treated groups as compared with placebo for all categories of incontinence, especially for urge incontinence. However, most of the evidence was subjective and it was not clear if this was maintained once treatment was discontinued. The addition of progestogen in combined HRT appeared to reduce the benefit of estrogen, possibly due to negative effects of progesterone on the bladder. In the same year, another meta-analysis concluded that there was no evidence that estrogens improved stress UI. 53
More recent studies of systemic HRT seem to be challenging the assumption that estrogens are largely beneficial or at least neutral as far as the bladder is concerned. The Nurses Health Study, 54 a large prospective cohort study, followed 39,436 postmenopausal and continent women over a four-year period. The incidence of new UI was significantly higher (relative risk [RR] between 1.34 and 1.64 depending on the type of hormone replacement) in HRT users. This risk diminished after stopping HRT and returned to baseline after 10 years of no HRT. The Heart Estrogen/Progestin Replacement Study also suggested a significantly increased risk of UI in women who used HRT. 55 The Women's Health Initiative (WHI), a large RCT, also reported an increased incidence of UI in HRT users at one and three years both in those who were symptomatic at baseline and those with no reported urinary symptoms at baseline. 56 The risk was highest for stress and mixed incontinence with no uniform effect on urge incontinence. In general, the estrogen (CEE) alone group appeared to have a more detrimental effect on incontinence than the combined CEE and medroxyprogesterone acetate (MPA). A more recent systematic review of 22 RCTs of hormone administration in postmenopausal women found an inconsistent improvement in UI. 57 Oral administration resulted in a worsening of mixed UI (RR1.5 [95% confidence interval (CI) 1.1–2.2]) and stress UI (RR1.8 [95% CI 1.6–2.1]). For both parameters, the risk was lower with combined estrogen and progestogen therapy than for estrogen alone. Indeed, oral estrogen alone increased stress UI with an RR 2.1 (95% CI 1.7–2.5) and total UI with RR 5.3 (95% CI 1.2–23.5). By contrast, transdermal therapy and estrogen gel were associated with high continence rates, although this study was self-reporting. 58 An RCT of ultra-low-dose transdermal therapy over two years primarily for bone protection in postmenopausal women did not show any improvement or worsening in subjective urinary symptoms. 59
Thus, the larger RCTs would appear to contradict previous assumptions based on earlier data and the patho-physiological changes seen with estrogen deficiency. There are a number of possible explanations for this:
Most of these studies were not specifically studying urinary symptoms as their primary outcome measure and the reporting was largely subjective. Most of the meta-analyses have been dominated by a couple of large RCTs such as the WHI. Although this is the largest RCT of postmenopausal hormone use the design of this study has been criticised even for its primary outcome measures due to a number of factors such as a relatively elderly population (21% over 70), wide age range (50–79) and the use of relatively high dose of estrogen and progestogen replacement. All these reservations equally apply to the interpretation of secondary outcome measures such as incontinence. Many of the studies have used oral CEEs and studies using other estrogens and different routes of administration show a more varied response.
We are thus left with the conclusion that either these studies are misleading because of poor design or systemic estrogens genuinely have a negative effect on the incontinence mechanisms. Estrogens are known to increase collagen remodelling,
60,61
and although this is generally thought to be a positive effect, this initially reduces total collagen and cross–linking, which may transiently weaken the pelvic floor and destabilize the detrusor muscle. If this was the case, then it might be expected that over time the symptoms would improve as collagen content increased, but as yet this is unproven and remains speculative. Equally, why vaginal estrogens have a better effect on urinary symptoms than systemic HRT is not clear. It is possible that the effects of topical estrogen on the genital mucosa and the improvement in genital atrophy are partly responsible for the improvements observed in lower urinary tract symptoms. Properly conducted randomized trials are needed, but are unlikely to occur in a large enough samples to give us the answers.
While the effect of estrogens on UI is certainly contentious, estrogens do have some proven positive effects on other bladder symptoms.
Recurrent urinary tract infections
The incidence of both urinary tract infections (UTI) and asymptomatic bacteriuria increases with age 62 as does the potential severity of any infection. Bacteriuria is present in one-fifth of over 65 year olds and increases steadily with advancing age, but how much of this tendency to infection is due to ageing and how much to the menopause is not clear. Loss of lactobacilli in the vagina after menopause results in the loss of the acidic vaginal environment and allows colonization with pathogenic bacteria and overgrowth of Gram-negative enteric organisms, including Escherichia coli, in the vaginal flora. In addition, vaginal and urethral atrophy leads to foreshortening of the vagina and retraction of the urethra reducing the body's natural defences against potential pathogens. However, Hextall et al. 62 found no specific changes in the rate of infection in relation to menopause. Estrogens readily reverse these microbiological changes in the vaginal flora and are thus are potentially useful for the treatment and prevention of recurrent UTI. Although there were some promising results from early studies, randomized trials have been less conclusive, although again the success may depend on the type of estrogen used. 63–65 Intravaginal estriol prevented recurrent UTI, 63 whereas there was no statistical difference between oral estriol cream and placebo. 64 However, in the largest study the vaginal ring (7.5 mg estradiol/24 hours) was significantly better at preventing recurrent UTI than placebo (45% versus 20%). 65 The HUT committee concluded in their third report that estrogens were of benefit in this situation particularly when used locally. 66 A reduction in the incidence of infections also seems to be associated with a reduction in the severity of other urinary symptoms. 67
Urogenital atrophy
Urogenital atrophy is a common observation in postmenopausal women affecting about 25% of women, even if they are taking systemic estrogen replacement. 68 In a population-based study of Australian women observed over seven years, vaginal dryness was a complaint in 3% of premenopausal women, 4% of women in early menopause, but up to 47% of women three years or more into their menopause. 69 More than a third of women presenting at a specialist menopause clinic were noted to have urogenital atrophy and an even higher percentage some degree of urogenital prolapse. 70 Urogenital atrophy can cause discomfort and dyspareunia and may result in a cessation of sexual activity with a reduction in quality of life. Atrophic urethritis and trigonitis can present with a range of presentations, including bladder pain, recurrent UTIs, urinary frequency and urgency, enhanced awareness of prolapse and vulval pruritis. 68
These symptoms can be successfully treated with estrogen replacement either topical or systemic. The vaginal route of administration provides better symptom relief than systemic treatment, 71 and the very low doses used in the vaginal preparations avoid the problem of endometrial stimulation and the need for progestogens 68 (this does not apply to CEE cream). Although all the different vaginal preparations are effective, as a treatment choice, women appeared to favour the estradiol-releasing tablet or vaginal ring for ease of use, comfort of product and overall satisfaction. 44 It may take several months for the symptoms to improve and treatment should be continued long term, otherwise symptoms are likely to return on its cessation. 72
Conclusion
Estrogens play an integral role in the development, function and maintenance of the urogenital tract. The estrogen deficiency seen after menopause is implicated in the pathogenesis of a number of conditions affecting the postmenopausal bladder. However, while there is no doubt that estrogens improve urogenital atrophy and its associated symptoms, its role in the management of bladder symptoms remains less clear. Topical estrogens are not only better for reversing the effects of urogenital atrophy, but also appear to have a positive effect on urinary frequency, urgency and to a lesser extent urge incontinence and reduce the incidence of recurrent UTI. This can all be achieved without any concerns about endometrial stimulation and the wider concerns about the safety of systemic HRT. Indeed, currently available evidence would suggest that systemic HRT far from improving urinary symptoms may actually make them worse, although this remains debatable. In clinical practice, faced with a postmenopausal woman with urogenital symptoms, the optimum solution should be to use vaginal estrogens initially to correct any underlying atrophy. This can be done in conjunction with other recommended interventions such as pelvic floor re-education and anticholinergics. If systemic HRT is used for other indications, then vaginal estrogens may need to be used as well to obtain maximal urogenital effects.
Competing interests
In the last 12 months, the author has received speaker fees from Astellas and Pfizer.