
Abstract
Objectives.
To observe the effect of yoga on menopausal symptoms using a prospective, randomized, controlled and interventional study.
Main outcome measures.
Total Menopause Rating Scale (MRS) score and three subscale scores (somatovegetative, psychological and urogenital) were measured on day 1 and day 90 in the study group which performed yoga (asana, pranayam and meditation) under supervision for three months, and were compared with the control group that did not perform yoga. MRS has been designed to measure health-related quality of life of ageing women. It consists of 11 symptoms and three subscales.
Results.
It was observed that on day 1 the scores in both the groups were comparable. On day 90, the scores in the yoga group showed a reduction in score on all the subscales, which was statistically significant. No significant difference was noted in the control group.
Conclusion.
Yoga is effective in reducing menopausal symptoms and should be considered as alternative therapy for the management of menopausal symptoms.
Introduction
The origin of the word menopause lies in the Greek words, ‘meno’ (menses, month) and ‘pause’ (stop, cease). Clinically, natural menopause is diagnosed retrospectively after 12 consecutive months of amenorrhea. With increased life-expectancy today women spend one-third of their life after menopause. More attention is needed towards treating peri- and postmenopausal symptoms, which can prove to be quite debilitating causing problems at home and in the workplace.
Around 20% of patients suffer from severe menopausal symptoms, 60% suffer from mild symptoms and 20% may have no symptoms at all. 1 Menopausal symptoms include mood changes, bloating, aches and pains, headaches, hot flushes, night sweats, tiredness, insomnia, weight gain, depression, irritability, forgetfulness, urinary frequency, dyspareunia and lack of concentration. These symptoms vary in severity and character from person to person.
Health workers continue to examine different ways to manage menopause to minimize discomfort and inconvenience during menopausal transition, so as to improve the quality of life of these women. Since estrogen deficiency is the cause of menopausal symptoms, hormone replacement therapy (HRT) is the most effective treatment. However, HRT has been associated with an increased risk of breast cancer, uterine cancer, thromboembolic heart disease and stroke. Results from Women's Health Initiative (WHI) study and Heart Estrogen/Progestin Replacement study demonstrated increased risk of cardiovascular system disease and breast malignancy among women randomized to hormone therapy, although risks have been shown to be influenced by the type of HRT and the age at which it is commenced. More women are becoming aware of the serious side-effects and risks; hence, the use of HRT for menopausal symptoms has decreased. 2
Considering the limitation of HRT, the present need is to explore new options for management of menopausal symptoms in the form of non-hormonal drug therapy and non-pharmacological measures. Many of the potential therapies warrant further study in trials with rigorous scientific designs to determine benefit and safety 3 Yoga is one such therapy /technique.
Yoga originated in India more than 4000 years ago. 4 The Sanskrit word yoga means ‘to join or to unite’ and the practice of yoga brings union of mind with body. Yoga has been utilized as a therapeutic tool to achieve positive health and to control and cure diseases. Interest has been shown in this direction by many workers and studies on the effect of yoga on some ailments like bronchial asthma, hypertension, 5 diabetes mellitus (DM) 6 and obesity have been carried out. The exact mechanism as to how yoga helps in various disease states is not known. It has been suggested that there could be neuro-hormonal pathways with a selective effect in each pathological situation. For example, it has been observed that plasma levels of Cortisol increase in bronchial asthma and decrease in DM after practice of pranayama. It is possible that yogic exercises bring about normalization of the pathological state by control of counter regulatory hormones or by increased receptor sites. It has also been suggested that yogic practices create a hypothermic state and an alteration in the sympatho-parasympathetic axis. 7
Few studies on yoga and menopausal symptoms have been carried out throughout the globe. Further research is required to investigate whether there are specific benefits of yoga for treating menopausal symptoms. Systematic studies in this field are lacking and hence we carried out a systematic study to evaluate the effect of yoga practices on menopausal symptoms.
Materials and method
This prospective, randomized and interventional study was carried out at Janardan Swami Yogabhyasi Mandai, Nagpur, an institute dedicated to ‘yoga’ education and research, between 22 November 2009 and 21 February 2010. An advertisement was published in local newspapers about a yoga camp to be conducted for women above 40 years of age lasting for three months. Pamphlets were distributed and hoardings were displayed around the city. A total of 220 women responded to the advertisement and registered for the camp. After screening, explanation about the study and obtaining written informed consent, 200 women fulfilled the inclusion-exclusion criteria. We planned to include 200 women to the study, as it was thought that this was the maximum number that was feasible to recruit.
Inclusion criteria were women between 40 and 55 years of age, women with irregular cycles and postmenopausal women within five years of menopause starting. Exclusion criteria: women taking HRT, women with severe psychiatric or medical disorders and women already performing yoga. Subjects were randomized into the study group (n = 100) and control group (n = 100) by a simple random sampling method of picking a chit with either ‘study’ or ‘control’ written on it. After noting the preliminary data on day 1, the women were asked to fill in the Menopause Rating Scale (MRS).
The MRS has been designed to measure the health-related quality of life of ageing women. It was developed by the Berlin Centre for Epidemiology Health Research and validated from the research network of many institutes. 8 It consists of 11 symptoms with scores varying from 0 (no symptom) to 4 (severe symptoms), the total score ranging from 0 to 44. Three independent dimensions are identified: somatovegetative symptoms (0–16 points, four symptoms are sweating/flush, cardiac complaints, sleeping disorders and joint and muscle complaints), psychological symptoms (0–16 points, four symptoms are depression, irritability, anxiety and exhaustion) and urogenital symptoms (0–12 points, three symptoms are sexual problems, urinary complaints and vaginal dryness).
The study group attended the camp daily from 6:00 to 7:00. The study group performed daily yoga practices including physical postures (asana), breathing techniques (pranayama) and meditation under supervision of an expert yoga trainer. A minimum attendance rate of 80% was compulsory. The physical postures of yoga were performed while standing, sitting, lying prone or in the supine position on the floor. Each joint in the body was taken through its full range of motion – stretching, strengthening and balancing each body part. Internal awareness and synchronization of asanas with breathing was considered important. Pranayama included the complete yoga breath – conscious breathing, duration of inspiration and expiration being altered, along with alternate nostril breathing (Nadi shodhan pranayam) and Bhramri pranayam. Meditation included techniques such as listening to one's own breath or chanting omkara to bring about a state of self-awareness and inner calm.
The control group was asked to report for the next camp after 90 days. This group was advised not to perform yoga practices or take medication for menopausal symptoms during the study period. On day 90, both the control group and the study group were again asked to fill in the MRS. Findings of the study group and the control group were compared and analysed by paired and unpaired t-tests and z-test.
Results
There were 10 dropouts from each group at the end of this study. Five women from the study group had less than 50% attendance and none of them reported on day 90 as they were aware that they did not fulfill the required attendance. Five women could not continue after the first few days because of domestic reasons. From the control group, 10 women did not report on day 90. Therefore, the data of 10 women from each group could not be obtained on day 90, and so the results of the 90 women belonging to each group were analysed.
It was observed that the age and body mass index of the two groups were comparable (P > 0.05) and peri- and postmenopausal status of women in both the groups were comparable (Table 1).
Menopausal status, age and BMI
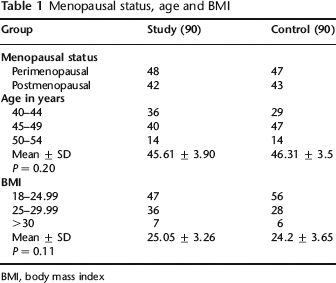
BMI, body mass index
The total MRS scores in both the study group and control group were high on day 1; mean total score of 9.37 ± 7.28 in the study group and 9 ± 6.76 in the control group, but on day 90 the mean score was significantly less (P < 0.001) in the study group (4.36 ± 4.8) compared with the control group (9.2 ± 6.72). By calculating the mean and median for the data, it is observed that the scores were normally distributed. Case-control significance on applying unpaired t-test shows highly significant difference in the two groups (Table 2).
Total Menopause Rating Scale

It was observed that the score on each of the three domains of the MRS scale, i.e. somatovegetative, psychological and urogenital subscales showed similar results (Tables 3, 4 and 5). On day 1, the scores in the study group and the control group under each subscale were comparable, but on day 90, the study group showed statistically significant difference in the score (P < 0.001) on all three subscales, whereas the control group did not show statistically significant difference in any of the three domains. The scores were normally distributed.
Psychological subscale

Somatovegetative subscale

Urogenital subscale

Discussion
Menopausal transition is a very important phase in a woman's life and menopausal symptoms are encountered by 60–80% of women. In developed countries, because of increased awareness, women seek medical advice for these symptoms, but in developing countries a large number of women consider these symptoms as physiological and continue to suffer without seeking any medical advice. Even those who seek medical advice and are candidates for hormone therapy undergo much anxiety because of the need for periodic follow-up and the perceived associated risk (WHI 2008). For this reason there is great interest in the use of alternative options for menopausal symptoms. A large number of non-hormonal options have been studied so far. Review of randomized controlled trials of complementary and alternative medicine (CAM) for menopausal symptoms by Krohenberg concluded that black cohosh and food containing phytoestrogens show promise for treatment of menopausal symptoms. This review also concludes that clinical trials do not support the use of other herbs or CAM therapies. Long-term safety data on individual isoflavones or isoflavone concentrates are not available. 9
Our age-old science of yoga has been studied for various medical disorders. Different studies have demonstrated effectiveness of yoga in hypertension, DM, heart disease and asthma.
A systematic review of yoga for menopausal symptoms concludes that the evidence is insufficient to suggest that yoga is an effective intervention for menopause and further research is required to investigate whether there are specific benefits of yoga for treating menopausal symptoms. 10
Our study is the only study in the literature where subjects performed daily yoga practices at a yoga centre under expert supervision for three continuous months ensuring consistency. In most of the published studies yoga practices were carried out for 8–10 weeks.11, 12 Yoga practices were taught to the subjects and they were instructed to perform them at home along with periodic classes.
Chhattha 12 has carried out a study to compare the effect of yoga and exercise on the Greene Climacteric Scale following two months intervention. In that study, the yoga group practiced an integrated approach to yoga therapy comprising sun salutations with 12 postures, pranayama and avartan dhyan, whereas the control group practised a set of simple physical exercises under supervision of trained teachers for eight weeks (1 hour daily for 5 days a week). The Greene Climacteric Scale was used to assess menopausal symptoms before and after intervention. A significant difference was observed in vasomotor symptoms, marginally significant difference in psychological symptoms but no difference in the somatic component. The effect size was higher in the yoga group for all factors.
The present study indicates a statistically significant improvement in menopausal symptoms after yoga intervention in all the three domains of MRS. There was a statistically significant difference in the total score along with the scores on all three subscales in the yoga group. No significant difference was noted in the control group at the end of the study. This study proves effectiveness of yoga in reducing menopausal symptoms. Yoga can be considered as a non-pharmacological option for management of menopausal symptoms.
Conclusion
It is concluded from this study that our age-old therapy, yoga should be recommended to all women of menopausal age. It is an effective, non-invasive, non-pharmacological method that is available free of cost or at low cost and is free of side-effects. Finally, the limitations of the study need to be acknowledged. Lack of blinding is the main limitation. Further systematic research is needed on a large scale on this topic.
Footnotes
Acknowledgements:
The authors would like to thank Di Jaydeep Nayse – Statistician, NKPSIMS, Nagpur; Seema Mujumdar – Yoga teacher, Janardan Swami Yogabhyasi Mandai; Dr Shobha Gandhi – President, Nagpur Obstetrics and Gynaecology Society; Dr Seema Kanetkar – Joint Secretary, Indian Menopuse Society, Nagpur; Dr Sarita Bhonsule – Executive member, Indian Menopuse Society Nagpur.