
Abstract
Objectives.
To determine patterns of premenstrual symptom experiences across the reproductive age range, and the effects of other factors on premenstrual symptoms.
Study design.
Global cross-sectional survey.
Sample.
A total of 7226 women aged 15–49 recruited by random sampling with approximately 400 each from France, Germany, Hungary, Italy, Spain, UK, Brazil, Mexico, Hong Kong, Pakistan and Thailand.
Approximately 1000 women in Japan and Korea and 500 Australian women were found using Internet panels.
Main outcome measures.
Questionnaire of 23 premenstrual symptoms, sociodemographic and lifestyle variables.
Results.
Four different patterns of premenstrual symptoms were found with ageing: symptoms showing no change with age, symptoms decreasing with age, symptoms reaching a maximum just before or around age 35, and symptoms reaching a maximum around age 40–44. Smoking was associated with an increase in most of the premenstrual symptoms. Increasing parity was associated with a decrease in some of the symptoms.
Conclusions.
These results suggest that the premenstrual symptoms most associated with the years of regular ovulatory cycles are skin disorders, lack of energy, appetite problems, joint/muscle/back pain, anger, abdominal bloating, depressed mood and irritability. Other symptoms which peaked later (swelling of extremities, breast tenderness/pain, weight gain) may reflect exacerbation by hormonal changes of the late reproductive/early menopausal transition. Smokers report more problematic premenstrual symptoms.
Introduction
Ageing is the natural progression of changes in structure and function that occurs with the passage of time in the absence of known disease. 1 Women experience reproductive ageing (hypothalamic-pituitary-ovarian axis) superimposed on chronological ageing and reach an essentially non-functional state with regard to reproductive ageing at menopause. 1 Much of the research on the relative effects of reproductive ageing has focused on symptoms associated with the menopause.
Premenstrual symptoms are known to be aetiologically linked with ovulatory cycles. These symptoms do not occur before puberty and onset of ovulatory cycles, or after ovulations cease at menopause. Premenstrual symptoms also do not occur during pregnancy. Induction of menopause with danazole, gonadotropin-releasing hormone analogues or surgical removal of ovaries has been shown to alleviate premenstrual symptoms.2–4 Within the reproductive age group encompassed by the years between puberty and menopause, the peak reproductive years (approximately age 18–35) are known to be those associated with regular ovulatory function. After age 35, there is a shortening of the follicular phase of the menstrual cycle and other changes of ovarian ageing, with anovulatory cycles increasing exponentially after age 37. Late reproductive phase is characterized by an elevated early-cycle follicle-stimulating hormone concentration in the setting of regular menstrual cycles, whereas early menopause transition is characterized by irregularity of menstrual cycling. 5
It thus follows that premenstrual symptoms associated with regular ovulatory menstrual cycles would be expected to reach a maximum during the peak reproductive years and to decline with ovarian hormone changes of the late reproductive phase and early menopausal transition.
Classificatory systems for premenstrual syndromes have included many different symptoms. To our knowledge there has been no attempt to explore how these symptoms vary by age and which symptoms peak during the peak reproductive years, and are thus more likely to be truly related to regular ovulatory function. As well most studies of premenstrual symptoms have been carried out by focusing on women in small geographic areas or individual countries. There have been very few attempts to study women's premenstrual symptom experiences simultaneously across different countries or ethnicities. 6
The objectives of this paper are to determine whether there are different patterns of premenstrual symptoms related to ageing. We also set out to determine an additive prediction model for each symptom utilizing associated explanatory factors from sociodemographic and lifestyle variables.
It was decided to include all symptoms that had been mentioned by the major classificatory systems for premenstrual syndromes (WHO ICD-107 defined premenstrual syndrome – PMS, ACOG 8 defined PMS and APA 9 defined premenstrual dysphoric disorder – PMDD). As different persistence criteria were given for ACOG 8 and WHO 7 defined PMS (3 months and 1 month, respectively) and DSM-IV defined PMDD 9 (most cycles in 12 months), women were asked how many months each premenstrual symptom was experienced. The symptoms were included in a questionnaire administered in cross-sectional population-based surveys carried out in Europe and Latin America10, 11 in 2003–2004 and later extended to Asian countries in 2008–2009.12–14 We have separately published some results for Europe/Latin America10, 11 and some (but not all) of the Asian countries.12–14 We have not previously examined the differential effect of ageing on individual premenstrual symptoms. The present data analysis allows us to explore whether there are patterns of premenstrual symptoms related to ageing using a large database of 7226 women, from European, Latin American, Asian and Australian women.
Statistical analysis of data thus far has generated the following key findings, which may have significance in understanding women's experiences of premenstrual problems. The most prevalent symptoms were abdominal bloating, cramps or abdominal pain, irritability, mastalgia and joint/muscle/back pains. Severity of symptoms was directly proportional to duration (number of affected cycles) (R = 0.78). Symptom prevalence (when studied as a summed or total duration × severity index TDS) was associated with age (linear and quadratic effects), parity, current smoking and country 15 In an earlier analysis of data from women in Europe and Latin America, 10 we have shown that the total premenstrual symptom index (TDS) varies with age, reaching a maximum by age 35, suggesting a possible link with regular ovulatory function that declines after this as women enter the late reproductive phase and early menopausal transition.
Materials and methods
Design
A cross-sectional questionnaire survey of premenstrual symptom experience was conducted with around 400–500 women of reproductive age found by random population-based sampling, in each of the following regions (countries): Europe (Germany, Spain, Italy, Hungary, France, UK); Latin America (Mexico and Brazil) and Asia (Hong Kong, Pakistan and Thailand). In addition, 1000 Korean and Japanese women and 500 Australian women were surveyed using Internet methodology.
Subjects
Europe/Latin America: Based on government national statistics in each country, a representative sample of women aged 15–49 years who were not pregnant at the time of the interview were randomly recruited according to demographic quotas primarily for age, and secondly for region (urban or rural) and education. Recruitment was based on telephone calls using numbers derived from different sources. Computer-assisted telephone interviews were conducted with consenting women.
Asia: A representative sample of urban women aged 15–49 years, who were not pregnant at the time of the interview, and who reported having had at least two menstrual periods in the past three months, were randomly recruited according to demographic quotas for age, for region and education. In each country, a small number of regions were a priori selected. In Hong Kong, 400 women were selected from New Territories (n = 181, 31%), Kowloon (n = 122,45%) and Hong Kong Island (n = 97, 24%). In Thailand, the sample of 400 women were selected from Chiangmai (n = 150, 37.5%) and Bangkok (n = 250, 62.5%). In Pakistan, women were selected from Karachi (n = 153, 38%), Lahore (n = 149, 37%) and Islamabad (n = 100, 25%). A record was kept of refusals and of those households where an eligible woman could not be contacted. The data were collected using face-to-face interviewer-administered questionnaires.
In both Thailand and Pakistan, the samples were selected using a two-stage cluster approach, with each city first divided into clusters of about 100 houses, and then selecting the clusters which would be finally included according to a random process. Women who met the eligibility requirement were randomly sought. In Hong Kong the study was conducted using telephone prerecruitment followed by a face-to-face interview in a central location.
In Japan, Korea and Australia, women in the age group 15–49 were sought using an Internet-based panel and the questionnaire was web based. Thus these three countries did not have randomly selected samples.
Participating women did not receive any payment for completing the survey.
Questionnaire
Each woman was asked about symptom experience premenstrually using a checklist of 23 symptoms (Table 1). The symptoms were those on the lists of the classificatory systems used in the diagnosis of PMDD according to DSM-IV 9 and PMS according to the ACOG criteria. 8 To ensure that women were only referring to symptoms occurring in the days before their menstrual periods, symptom questions were introduced with the statement: ‘In the following interview we would like to focus only on the symptoms that might occur within the days before your menstrual period starts and that disappear as soon as, or a few days after, the period begins’. This point was reiterated with each question.
Separate model for each symptom measured by the DS score
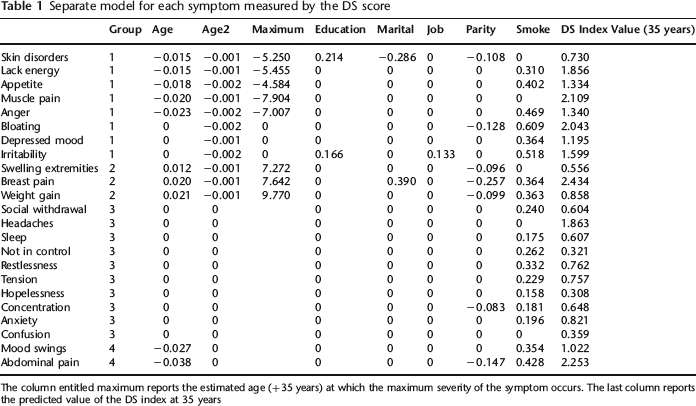
The column entitled maximum reports the estimated age (+35 years) at which the maximum severity of the symptom occurs. The last column reports the predicted value of the DS index at 35 years
Women who reported that any premenstrual symptom did occur were asked (for each symptom) information on symptom severity (mild, moderate or severe) and duration of symptom (during how many of the menstrual cycles in the last 12 months had she experienced the symptom). The order of symptoms in each group was changed between interviews.
Women were also asked if the premenstrual symptoms affected activities of daily life, including work, studies, housework, leisure activities and social relationships.
Sociodemographic variables
These included age, country and region, education level, age at first occurrence of premenstrual experiences, marital status, working status (full time, part-time, no paid work), smoking habits, income level, exercise participation, and use of oral contraceptive pill and other medications.
Statistical analysis
Sample description
The countries were compared for sociodemographic and lifestyle variables (age, education, marital status, work status, parity, exercise, smoking status and oral contraceptive use).
Premenstrual symptom experience
Symptoms were described by their severity (0 = no, mild, moderate, severe = 3) and their duration (number of cycles symptoms were experienced in last 12 months).
Our first objective was to determine whether there were different patterns of premenstrual symptoms across the lifespan from 15 to 49 years. Symptoms can be specific to premenstrual syndromes but there may also be confounding, as symptoms might occur for other reasons. The prevalence of a symptom specific to endocrine changes underlying premenstrual syndromes might be expected to increase after puberty, reach a maximum around the expected age just proximal to ovarian hormonal changes of the late reproductive phase and early menopausal transition, and then decrease with age and these phases of declining ovarian function. Such an inverted U-shaped curve was used to identify symptoms at menopause where the peak incidence was presumed to be around age 50. 16 In contrast, symptoms not related to reproductive ageing but linked to chronological ageing will be expected to vary linearly over time. Finally age was also hypothesized as only one of many possible variables affecting symptom prevalence.
To identify the effect of age on symptom prevalence, the variables listed above were considered as independent explanatory variables in a linear model in which premenstrual symptom prevalence (calculated as duration × severity) was the dependent variable. For age, a linear model associated with a continuously increasing or decreasing effect was assumed for the studied symptom. A quadratic component, Age 2 was also added to the model to detect the presence of non-linear effects, i.e. U-shaped curves (decreased prevalence followed by increased prevalence) or reverse U-shaped curves (increased symptom prevalence followed by decreased prevalence). The age at which the prevalence of each symptom was greatest was calculated in relationship to the reference age of 35 years, as after this age women increasingly pass into the changes of late reproductive functioning and the menopausal transition.
The country of origin is a complex variable encompassing many factors such as sociocultural attitudes, behaviours, use of medications, diet and lifestyle. Country was therefore considered as a random variable. A general linear model was used in which main effects and first-order interaction effects were introduced into the model.
Miscellaneous
Given the large sample size, only P values of at least 0.001 were considered as significant. With a sample size of at least n = 7000, when calculated on the whole sample, the half-confidence interval or precision of the proportions is less than 1% and will not be mentioned. The statistical analysis was carried out with R Statistical Package.
We assumed that missing data were missing at random. A systematic allocation of missing data by the full maximum likelihood principle was used, when the proportion of missing data was less than 5%.
Results
Sample description
There was a total of 7226 women from 14 countries with national sample sizes between 400 and 1039. The response (and refusal rates) are not known for all countries. We have published these response (and refusal rates) for Thailand, Pakistan and Hong Kong. 12 The distribution of sociodemographic and lifestyle variables across countries revealed differences. 15 The proportion of women aged >35 years was significantly higher among the samples for European countries and Australia. Educational level was observed higher in women sampled in Australia, Korea and Hong Kong. Overall 67.7% of women in the sample were living with a partner, with much lower proportions of partnered women in Hong Kong and Korea (≈40%). Fifty percent of the whole sample of women worked outside the home, but the percentages were much lower for Mexico (33%) and Pakistan (9%). Parity was not very different across countries with 48% having no children and 10% with at least three children. Only Mexico was characterized by larger family size (21% with at least 3 children). Important disparities were observed in exercise, smoking habits and oral contraceptive current use.
Patterns of premenstrual symptoms with age
Age (linear and quadratic effect), educational level, occupational status, parity, exercise participation, smoking habits, relationship status and use of oral contraception were used as potential associated factors with the severity and duration of each premenstrual symptom. Our results can be summarized as follows:
Effect of age
For nine symptoms, there were no effects of age; thus, these symptoms remained constant during the lifespan 15–49 years. These were social withdrawal, headaches, sleep disturbances, not in control, restlessness, tension, hopelessness, poor concentration and anxiety.
For 11 symptoms there was a U-curve related with age (skin disorders, lack of energy/lethargy/fatigue, changes in appetite, joint/muscle/back pain, anger, abdominal bloating, depressed mood, irritability, swelling of extremities, breast tenderness or pain, weight gain). Thus all these symptoms increase in severity from 15 years to reach a maximum value, and then decrease until 49 years. The maximum value was calculated (Table 1): for three of these symptoms (swelling of extremities, breast tenderness or pain, weight gain), the maximum value occurred between seven and nine years after 35 years, whereas for the other symptoms of this category, the maximum occurred before or around 35 years.
Finally three symptoms were characterized by a decreasing value from 15 years: confusion, mood swings, and cramps or abdominal pain.
Thus we found the four categories of premenstrual symptoms ordered in Table 1, and summarized in Figure 1:
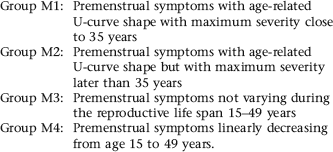
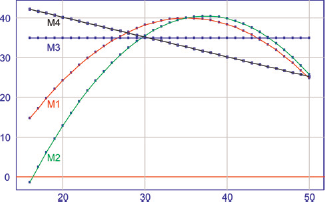
Mean growth curve for the four groups of symptoms. Group MI: all the symptoms with age U-curve shape with maximum severity close to 35 years; group M2: symptoms with age U-curve shape but with maximum severity later than 35 years; group M3: symptoms not varying during the whole life span 15–50; group M4: symptoms linearly decreasing from 15 until 50 years
Effect of other factors
Smoking was associated with a strong aggravation of many symptoms. Compared with mean predicted value at 35 years (last column of Table 1), the mean aggravation was 21% over all the symptoms.
Increasing parity was shown to be associated with a decrease of severity and duration for five symptoms (4 of which were physical symptoms). Age cannot be an explanation, as this variable was specified in the model.
Higher educational level was associated with increased prevalence of premenstrual skin disorders and irritability while employment was associated only with increased irritability.
Living with a partner was associated with increased prevalence of premenstrual breast tenderness or pain but less premenstrual skin disorder.
For each symptom, the standard deviation between countries estimated by the mixed model remained constantly small compared with the overall mean (less than 10%). Similarly this value was found small compared with the mean residual of the model (always less than 25%). However, for all the symptoms, five countries were observed to have significantly higher values (UK, Japan, Brazil, Australia and Korea). Hong Kong, Pakistan, Thailand and Germany were characterized by small values of symptoms. (Tukey multiple comparison of means adjusted for the other predictors, P < 0.05).
Discussion
This study uses non-linear modelling to indicate which premenstrual symptoms are most likely related to ovarian hormonal changes associated with ovulatory cycles.
These findings are of importance to clinicians and researchers alike. The 11 symptoms that reach a peak during reproductive life are in the 13 most prevalent premenstrual symptoms experienced by this group of women in terms of severity and persistence. 15 Thus all these symptoms (skin disorders, lack of energy/lethargy/fatigue, changes in appetite, joint/muscle/back pain, anger, abdominal bloating, depressed mood, irritability, swelling of extremities, breast tenderness or pain, weight gain) should be included in any questionnaire assessing premenstrual symptoms. Three of these symptoms (swelling of extremities, breast pain and weight gain) seem to worsen as women enter their 40s and may be exacerbated by the ovarian hormonal changes associated with the later phases of reproductive functioning. Premenstrual symptoms that show no change with age (social withdrawal, headaches, sleep disturbances, not in control, restlessness, tension, hopelessness, poor concentration and anxiety) or decrease with age (confusion, mood swings and cramps or abdominal pain) may have different aetiology to the other groups of symptoms and there may be little utility of including them in clinical enquiries or questionnaires.
We have previously reported that age had a significant effect on the summed duration severity index of premenstrual symptoms but had not carried out an exploratory analysis to identify if there were different patterns with regard to how individual symptoms relate to age.10, 12 In previous analyses using stepwise linear regression we had identified that smoking affected the summed duration severity index in Europe 10 but not in Asia, 12 possibly related to lower rates of smoking in Asia. Parity was shown to affect the summed duration severity index in Asia. 12 We have not previously reported the effect of factors such as parity, smoking, education on individual premenstrual symptoms.
Unfortunately, we did not have hormonal or other indicators of ovulatory function. Thus, our findings will need to be confirmed by studies that include these measures. As well our study involved retrospective recall by women rather than prospective daily ratings of symptoms. Self-report measures can introduce bias, and discrepancies have been found between retrospective and prospective ratings in the same population of patients.17–20 However, daily charting is difficult with up to 50% of women refusing21, 22 making these studies not generalizable to most women's experience of the menstrual cycle. The retrospectivity was not considered to be as crucial for the present study, which is not aiming to diagnose the prevalence of the syndromes of PMS or PMDD in the women studied but rather to characterize women's own perceptions of the symptoms they experience. All reporting of symptoms to clinicians is based on retrospective recall. The present study thus provides clinicians and researchers with reliable information on premenstrual symptom experience from women in 14 different countries.
Cigarette smokers reported increased duration and severity of most of the premenstrual symptoms studied. The following symptoms were not affected by cigarette smoking: skin disorders, joint/muscle/back pain, swelling of extremities, headaches and confusion. Cigarette smoking affects many body systems adversely, including ovarian functioning, with an earlier age of menopause reported for cigarette smokers.23, 24 Cigarette smoking is also known to be associated with mental morbidity, which may also exacerbate symptom perception. Thus it is not clear whether the exacerbation of premenstrual symptoms reported by cigarette smokers is due to biological or psychological factors or both. Further research is needed to clarify the impact of cigarette smoking on women's experience of premenstrual symptoms.
Strengths of the present study include the large sample size and use of the same instrument so that countries can be compared. Population-based sampling was used in all but three of the countries, to reduce bias from convenience or clinic samples. Interestingly those three countries where Internet panels were used had higher symptom values reported when all symptoms were considered together, suggesting some bias may have been introduced by this method of sampling. There were no differences observed between regions. The current study also incorporated all symptoms listed by the current classificatory systems and did not limit symptom experience to those required for PMDD, 9 which is very much weighted to psychological symptoms with only one somatic group of symptoms among 11 symptom groups. Thus women's experiences of premenstrual symptoms could be ascertained more broadly.
Conclusion
These results suggest that the premenstrual symptoms most associated with the years of regular ovulatory cycles are skin disorders, lack of energy, appetite problems, joint/muscle/back pain, anger, abdominal bloating, depressed mood and irritability. Other premenstrual symptoms peaked later, during the years of the late reproductive phase/early menopausal transition (swelling of extremities, breast tenderness/pain, weight gain) suggesting these symptoms may be exacerbated by hormonal changes occurring then. Further studies, which include markers of ovulatory function or ovarian hormonal changes and are prospective in nature, are needed.
Footnotes
The scientific content of this contribution reflects the opinion of the authors, the first two of whom received an honorarium. The authors were solely responsible for writing this article. Data were analysed independently of the company by the first two authors.