
Abstract
Objective.
To find out the association of menopause-specific quality of life of women with both working status and duration of postmenopausal years.
Study design.
We conducted a cross-sectional study on 250 postmenopausal women belonging to Bengali-speaking Hindu ethnic group, aged 47-62 years in the city of Kolkata, West Bengal, India. The participants were literate, living in wedlock with at least one surviving child, attained natural menopause at least two years ago and have never taken hormone replacement treatment. Menopause-specific quality of life was measured using a self-administered standard questionnaire (Menopause-Specific Quality of Life questionnaire, or MENQOL). MENQOL consisted of 29 menopausal symptoms (items) that are grouped under four domains. Additional information on sociodemographic aspect and reproductive history of the participants were collected using a pretested questionnaire.
Main outcome measures.
Both bivariate and multivariate analyses showed that menopause-specific quality of life decreases with the increase in duration of postmenopausal years. Although bivariate analysis demonstrated that working women had a better menopause-specific quality of life than their non-working counterpart, multivariate linear regression model did not corroborate to this finding.
Conclusion.
Duration of postmenopausal years had a significant association with menopause-specific quality of life of women.
Introduction
Quality of life is understood as the individual's perception of status in life according to the cultural and value system the person lives in, considering their aims, expectations, standards and worries. 1 This concept centres on various domains like, philosophical, psychological, social, political and health, and is considered for assessment of wellbeing at both individual and community level.
Menopause is an inevitable reproductive phase during midlife when various physical and mental changes may impair the quality of life of women.2-5 The quality of life during the menopause is a complex interaction of several different kinds of variable, 5 which is assessed not only by the frequency and severity of menopausal symptoms, life satisfaction and perceived health and mental status,6,7 but also by the individual's attitude towards loss of fertility, increase in duration of postmenopausal years, educational, working and marital status and also parity.2,8-11 Like other developing countries, Indian women posses a positive attitude towards menopause as they consider this phase as a relaxation from menstrual hassles.12-16 Studies from India also reveal that impairment in quality of life of middle-aged women is associated with psychological and somatic problems rather than other menopause-specific health problems.12,13,17,18
In the Indian context, studying quality of life after menopause is important because of an observed trend in the advancement of age at menopause, increase in both life-expectancy and subsequently the number of elderly women.19-21
So far, few studies have been carried out on menopause-specific quality of life in India. The present study aims to find out the association of menopause-specific quality of life with respect to working status and duration of postmenopausal years.
Methods
Study area
The present study was conducted in the city of Kolkata, the state capital of West Bengal, located on the eastern side of the country. In this state, English language is still taught as a compulsory subject at least till school level. At present, the literacy rate of this state ranks in higher order compared with other states of this country. 22
Study population
From a list of 141 Kolkata Municipal Corporation wards, 10 wards were selected randomly. From these, a total of 410 women belonging to Bengali-speaking Hindu ethnic group aged between 47 and 62 years were enlisted. From this list, following criteria of selection only 250 women were finally selected. The selection criterion includes living in wedlock with at least one child, have attained natural menopause at least two years prior to the study and received no hormone therapy and received at least 10 years of formal education with English language as a compulsory subject. Among those who did not participate (160), one-third (59) was either unwilling to participate in or unavailable during the time of study, and the rest (101) did not fulfill the study criteria. Written consent was taken from all the participants who finally took part in the study.
Data collection
A self-administered Menopause-Specific Quality of Life questionnaire (MENQOL) developed by Hilditch et al. 23 was used in collecting data. This questionnaire was introduced and explained explicitly to all the study participants by one of the authors (NS). The MENQOL questionnaire include a list of 29 menopausal symptoms (items) grouped into four domains (Box 1). The participants were asked to fill up the questionnaire on the basis of their experience of all the 29 symptoms during the past one-month period. Another pretested questionnaire was used to collect sociodemographic characteristics (present age, education and occupation of self and husband, monthly household expenditure) and reproductive history (age at menarche, marriage and menopause; use of oral contraceptives) of the participants. The entire data were collected during the period March to June 2010.
List of MENQOL symptoms under four domains
Vasomotor
Hot flushes
Night sweats
Sweating
Psychosocial
Dissatisfied with personal life
Feeling anxious or nervous
Experiencing poor memory
Accomplishing less than before
Feeling depressed, down or blue
Impatient with other people
Desire to be alone
Physical
Flatulence or gas pains
Aches in muscles and joints
Feeling tired or worn out
Difficulty in sleeping
Aches in back of neck or head
Decrease in physical strength
Decrease in physical stamina
Feeling a lack of energy
Drying skin
Weight gain
Increase in facial hair
Changes in tone of skin
Feeling bloated
Low backache
Frequent urination
Involuntary urination during laughing and coughing
Sexual
Change in sexual desire
Vaginal dryness during intercourse
Avoiding intimacy
Quality of life
Data analysis
Data were analysed using Statistical Package for Social Science (SPSS Inc., Chicago, IL, USA) version 11.0. Descriptive analyses of sociodemographic characteristics and reproductive history were performed. The participants who were homemakers have been considered as non-working’ (125) and those engaged in various professions as ‘working’ (125). The age at menopause was found to follow normal distribution and its mean value and standard deviation was calculated. Duration of postmenopausal years was measured by calculating the difference between present age and age at menopause. Since the duration of postmenopausal years did not follow normal distribution, its median value was considered. The participants were categorized into three groups on the basis of duration of postmenopausal years as Group 1 (<5 years), Group 2 (5-10 years) and Group 3 (>10 years).
The score for each of the symptoms of every domain of MENQOL questionnaire was first recoded and then analysed for mean values and standard error following Hilditch et al. 23 Student's ‘t-test’ and analysis of variance (F test) were used to compare mean scores of botheration for each of the symptoms and domains and quality of life (summary score) between working and non-working groups and among three postmenopausal age groups, respectively. Multivariate linear regression (stepwise) analyses were done to find out the significant predictors of each of the four domains and quality of life using sociodemographic and reproductive characteristics as independent variables. In this case, some of the sociodemographic (educational level of participants and of their husbands and occupational types of the husbands) and reproductive characteristics (age at menarche and parity) were multilevel in nature, so, they were converted into dummy variables. Reference group for each multilevel categorical variable was as follows: educational level of participants and of their husband (above graduate), occupational types of the husbands (others), age at menarche (>13 years), parity (more than 2). Variables like working status and use of oral contraceptives were introduced as binary variables. Other variables (monthly household expenditure, age at marriage and duration of postmenopausal years) were used as continuous variables in this linear model. Only significant predictor variables were presented. A minimum P value ≤0.05 was considered as statistically significant. Internal consistency of four domains (vasomotor, psychosocial, physical and sexual) was checked using Cronbach's Alpha test, and the test results proved to be acceptable.
Results
The mean age of the participants was 54.40 + 4.373 years. Most of the participants and their spouses had attained education till graduation level; half of the participants were homemakers. The husbands of these participants were mostly in service. The monthly household expenditure of most of the participants was between 200.90 and 301.32 (in US dollars) (Table 1).
Sociodemographic characteristics of study participants (n = 250)
Private tutor
Retired from service
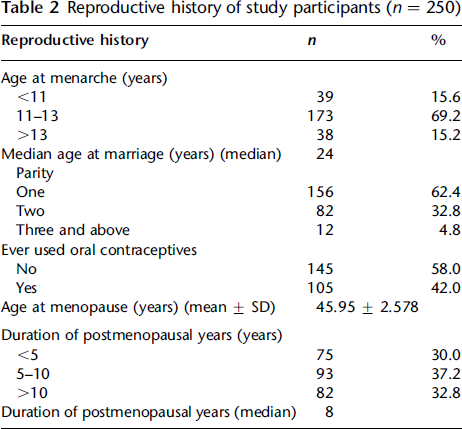
Table 2 demonstrates that most of the participants had attained menarche in the age period 11-13 years, got married around 24 years, never used oral contraceptives and given birth to one child. The mean age at menopause and the median value for duration of postmenopausal years (median) were 45.95 + 2.578 and eight years, respectively.
Reproductive history of study participants (n = 250)
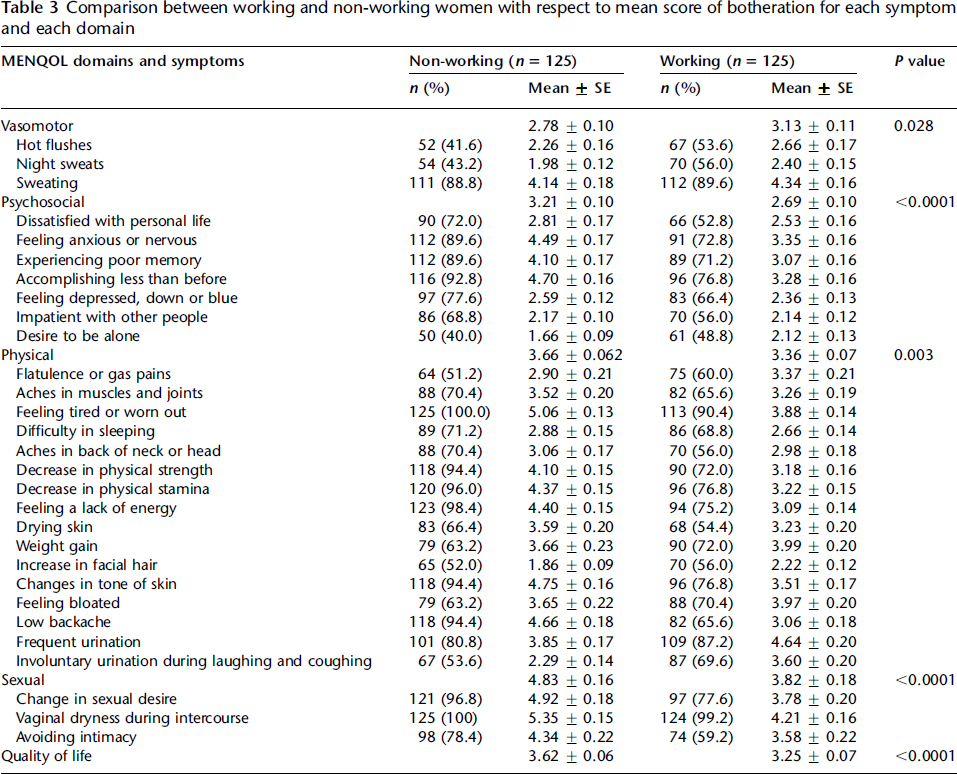
Comparison between working and non-working women with respect to mean score of botheration for each symptom and each domain
Comparisons among three groups of postmenopausal women with respect to mean score of botheration for MENQOL symptoms and domains

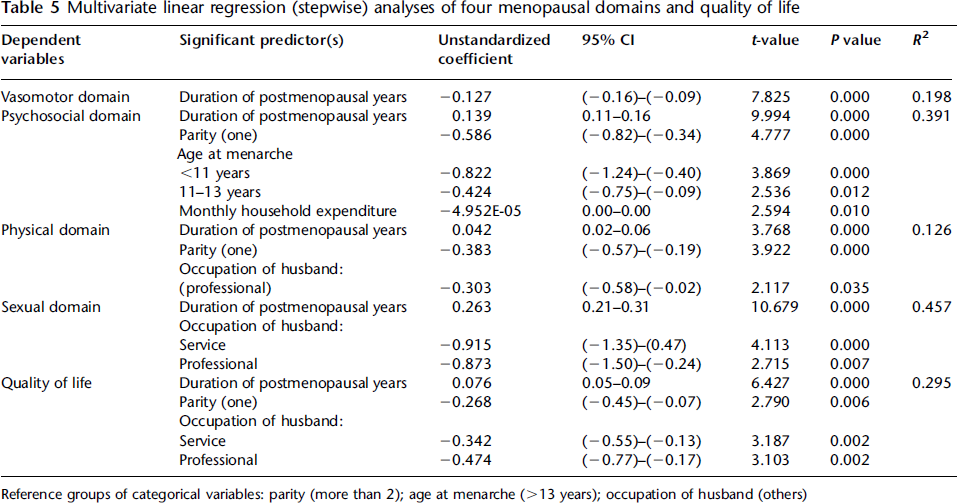
Multivariate linear regression (stepwise) analyses of four menopausal domains and quality of life
Discussion
In this cross-sectional study, we attempt to evaluate the quality of life of postmenopausal women for differential working status and duration of postmenopausal years using the MENQOL questionnaire. Bivariate analysis demonstrates that working women have a better menopause-specific quality of life than their non-working counterpart. This finding is in close agreement with other studies.2,10,11,24 The poor quality of life among non-working group of women is likely to be associated with their lack of economic independence, which reduces the possibility of availing healthcare services. On the other hand, working women are supposed to have better social support, relatively higher self-esteem, economic independency and also ability to access better healthcare services. In developing countries, women have more limited access to food, education and medical care, and increased physical and mental health risk because of the existence of gender-based social, cultural and economic inequalities;25-27 however, one study suggests that gender differences in health is found to be less apparent during midlife. 28 In our study, multivariate analysis does not show any significant association between working status of the participants and menopause-specific quality of life. Here, occupational types of husbands seem to be the predictor for most of the MENQOL domains. It is likely that socioeconomic status of spouses rather than their own work participation per se contributes more in determining the health status of women. A study from rural India corroborates with this finding. 29
Duration of postmenopausal years seems to be an important factor that affects menopause-specific quality of life. Our study shows that the chance of experiencing the problems among postmenopausal women (barring vasomotor) tends to be higher with increase in duration of postmenopausal years. The same trend has been observed in a study on Iranian women. 10 Vasomotor problems are directly related with changes in the hormonal level (progesterone and estrogen) that occur prior to menopause (perimenopasual period) and continues till the first few years of postmenopausal life. Thus, the incidence of vasomotor problems is found to be higher during the period of menopausal transition rather than after menopause. 30 Additionally, a study on Pakistani women reveals that with transition from perito postmenopausal stage, there is a gradual decrease in the score for psychosocial domain and increase in score for physical domain. 31 Our findings imply that both chronological ageing and ovarian ageing may be the factors that bring impairment in menopausal quality of life. Increase in chronological age gives rise to loss of reproductive function due to the decline in number, quality and endocrinal activity of ovarian follicle. 32 Relative contribution of chronological ageing and ovarian hormonal changes seems to have a broad range of effects on physical, psychosocial, sexual and mental health consequences.33,34 Acknowledging the effects of ageing and menopause on health, presently doctors of several Asian countries share a more negative view of menopause with their patients and encourage older women to consider medical interventions.35,36 As a result, in developing countries, educated women from higher social classes have started to consider menopause as a health problem and seek treatment for it, although they may not fully understand it. 37 Apart from this, general awareness programmes related to menopause and menopausal health may improve the quality of life of menopausal women, as found in Iran. 38 Thus, the findings of the present study will help in increasing awareness among health practitioners and health planners about menopausal health in India.
The study has certain limitations like, small sample size and representation from a particular urban ethnic group. However, since this type of research is a maiden effort in Indian context, the findings may lead to future research on menopause-specific quality of life in diversified ethnic groups.
We conclude that duration of postmenopausal years has significant effect on quality of life, but not the working status of women per se.
Footnotes
Acknowledgements:
We would like to express our gratitude to the study participants and are thankful to Dr Arupendra Mozumdar, Dr Shailendra Kumar Mishra and Bhubon Mohon Das for their valuable comments in preparing this manuscript. The project has been approved by the Ethical Clearance Committee of the University of Calcutta. Funding was provided by University Grant Commission, India.
Competing interests: None declared.