
Abstract
Postmenopausal estrogen deficiency can lead to symptoms of urogenital atrophy. Individuals with urogenital atrophy have symptoms that include vaginal dryness, vaginal and vulval irritation, vaginal soreness, pain and burning during urination (dysuria), increased vaginal discharge, vaginal odour, vaginal infections, recurrent urinary tract infections, pain associated with sexual activity (dyspareunia) and vaginal bleeding associated with sexual activity. Despite the frequency and effects of vaginal atrophy symptoms, they are often under-reported and, consequently, under-treated. Therefore, care of a menopausal woman should include a physical assessment of vaginal atrophy and a dialogue between the physician and the patient that explores existing symptoms and their effect on vulvovaginal health, sexuality and quality-of-life issues. The development of the ultra-low-dose 10-µg estradiol vaginal tablets is in line with the requirements of regulatory agencies and women's health societies regarding the use of the lowest effective hormonal dose. Because of its effectiveness and safety profiles, in addition to its minimal systemic absorption, the 10-µg estradiol vaginal tablet can offer greater reassurance to health-care providers and postmenopausal women with an annual estradiol administration of only 1.14 mg.
Introduction
Vaginal atrophy, caused by postmenopausal estrogen deficiency, is a common but under-recognized and undertreated disorder. Despite the prevalence of vaginal atrophy, only about 25% of women who have vaginal atrophy volunteer this information to their health-care provider, and 70% of these women report that physicians rarely or never ask about vaginal dryness, with patients and physicians both preferring to cite the ageing process as the reason for problems. 1
Because the vagina and surrounding tissues require estrogen stimulation to maintain normal structure and function, postmenopausal estrogen deficiency can result in significant cytological and structural changes in the vulva, vagina and lower urinary tract. The decrease in estrogen levels also prompts the development of vulvovaginal symptoms, including vaginal dryness; itching, burning and inadequate lubrication during sexual activity; and urinary symptoms, including frequency, urgency, incontinence and dysuria. 2–4 These symptoms, which range from mildly annoying to very bothersome, can cause significant emotional distress, reduce patient quality of life and contribute to sexual dysfunction. 5–8
Symptoms of vaginal atrophy, in contrast to the vasomotor symptoms associated with menopause, typically do not resolve without elective treatment and do not diminish over time. 2 Therefore appropriate treatment should begin before irrevocable atrophic changes occur. 1
Local estrogen therapy is the treatment of choice for women with vaginal atrophy without any other postmenopausal symptoms. Local estrogen therapy also provides the benefits of a lowered potential for systemic exposure and reduced occurrence of adverse effects. 9 The development and approval of an ultra-low-dose intravaginal estrogen tablet (10-µg estradiol [E2] tablet, Vagifem®, Novo Nordisk A/S Bagsvaerd, Denmark) aligns with the recommendations of regulatory authorities and therapeutic experts from menopause societies to prescribe estrogen at the lowest effective dose. 9–11 The purpose of this review is to summarize the pharmacokinetic profile, safety and effectiveness of Vagifem® 10 µg, the lowest E2 dose commercially available.
Development of the 10-µg E2 vaginal tablets: review of pivotal studies
Minimal E2 absorption – pharmacokinetics
The direct administration of estrogen to atrophic vaginal tissue results in little systemic exposure and is the preferred route for the treatment of local atrophy symptoms, per the recommendations from women's health societies. 1 Since vaginal atrophy is a chronic condition requiring long-term treatment, the main goal in the development of the 10-µg E2 vaginal tablets was to provide symptom relief while reducing systemic exposure to estrogen. Therefore, the pharmacokinetic properties of the 10-µg E2 tablets were evaluated using gas chromatography-mass spectrometry (GCMS). 12,13 The pharmacokinetic properties of 25-µg E2 vaginal tablets were also included in the assessments, as the 25-µg tablets have been available for many years, but their pharmacokinetic parameters were never previously evaluated by this very sensitive method. 14
The main objective of this trial was to evaluate the absorption of E2 in subjects taking one tablet of 10- or 25-µg E2 every day during the first two weeks and two tablets per week for the remaining 10 weeks. The dosing regimen chosen for this study mirrored the current recommended prescription. Systemic concentrations of estrone (E1) and estrone sulphate (E1S) were also assessed. Blood samples were drawn from 58 women randomly assigned in equal numbers to self-insert the 10- or 25-µg E2 vaginal tablets. Plasma E2 concentrations were measured by GCMS over 24 hours as follows: at baseline (day –1), on the first day (day 1) and on the last day (day 14) of the two-week, once-daily treatment, and immediately before (day 82) and after (day 83) the last dose during the twice-weekly maintenance period.
The 10- and 25-µg vaginal tablets had similar E2 absorption patterns (Figure 1). The initial higher absorption rate followed by a decrease over time was observed with both doses and can be explained by the fact that systemic absorption is more likely to occur with the thinner, more friable atrophic epithelium.
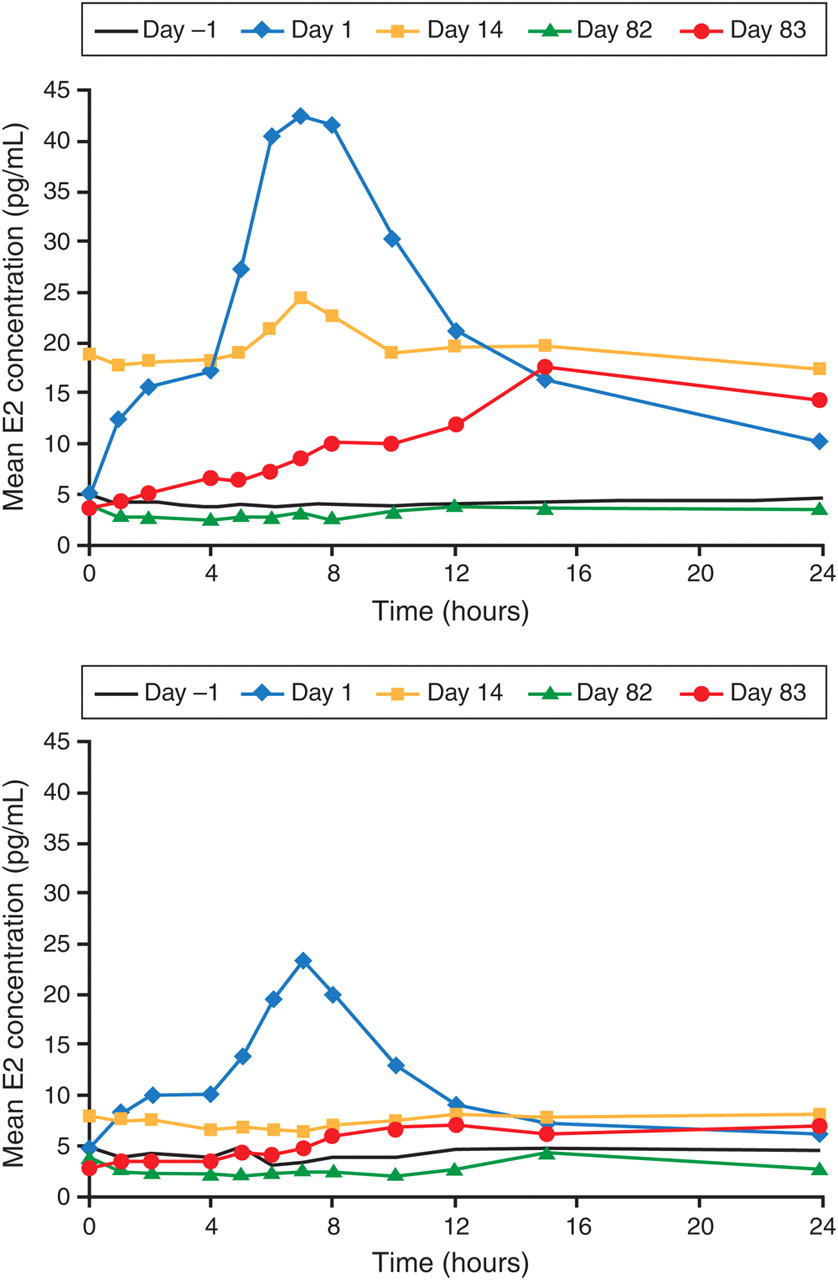
Time course of mean estradiol (E2) plasma concentrations during the 24 hours after vaginal administration of 25-µg E2 tablet (top panel) and 10-µg E2 tablet (bottom panel) on days –1, 1, 14, 82 and 83 of treatment (reprinted with permission from Eugster-Hausmann et al. 14 )
The mean E2 concentration was approximately 50% lower on days 1 and 83, and approximately 65% lower on day 14 with the 10-µg dose of E2, compared with the 25-µg dose (Figure 1). 14 Across the entire evaluation period, mean E2 concentrations with 10-µg E2 remained within the reference ranges that have been previously published for normal postmenopausal women (mean ± SD, 7.26 ± 4.82 pg/mL; n = 30; normal postmenopausal women measured also by GCMS 12 ), whereas with the 25-µg dose, the reference range was exceeded in the first two weeks (Figure 1). 14
E1 and E1S (less active metabolites) may potentially be converted to E2, consequently increasing estrogen levels. With the 25-µg dose a small increase in E1 levels was observed, but no increase of either metabolite was observed with the ultra-low-dose 10-µg tablet, therefore, confirming minimal estrogen absorption. As concluded by Eugster-Hausmann et al., 14 these results suggest that systemic estrogen exposure with the ultra-low-dose 10-µg E2 vaginal tablet is minimized, implying that the likelihood of occurrence of clinically relevant systemic side-effects is also minimal.
Effectiveness and safety
The effectiveness and safety of the 10-µg E2 vaginal tablet for the treatment of vaginal atrophy was evaluated by a one-year, double-blind, randomized, parallel-group, placebo-controlled trial conducted in 309 postmenopausal women in the USA and Canada. 15 The participants were randomly assigned 2:1 to receive vaginal tablets containing 10-µg E2 or placebo and were instructed to insert one 10-µg E2 vaginal tablet or placebo daily for 14 days and, subsequently, one tablet twice per week at the same time of day.
Efficacy endpoints included mean change from baseline to week 12 in
Vaginal Maturation Index; Vaginal Maturation Value; Vaginal pH; Mean composite score of the most bothersome moderate to severe symptoms of vaginal atrophy as identified by the patient, including vaginal dryness, vaginal and/or vulval irritation/itching, vaginal soreness, dysuria, dyspareunia and vaginal bleeding associated with sexual activity.
Cytology samples were taken from the upper third of the right lateral vaginal wall. Additionally, participants also completed a vaginal atrophy symptoms and severity questionnaire. They were also instructed to identify the one symptom that was most bothersome to them. The mean score of the most bothersome urogenital symptom within each treatment group was calculated.
After two weeks of daily administration of 10-µg E2 tablets, the following changes were observed:
A significant increase in the proportion of vaginal superficial (P < 0.001) and intermediate cells (P < 0.001), along with a concurrent decrease in the proportion of vaginal parabasal cells (P < 0.001), compared with placebo; Maturation value showing a statistically significant treatment effect (P < 0.001), indicating maturation of the vaginal epithelium and calculated according to the formula MV = (0 × % parabasal cells) + (0.5 × % intermediate cells) + (1.0 × % superficial cells) where MV is the maturation value; Vaginal pH score was significantly reduced to a more normal, acidic value (P < 0.001).
At baseline, most participants indicated dyspareunia (placebo: 62 [61%]; 10-µg E2: 107 [53%]) and vaginal dryness (placebo: 27 [27%]; 10-µg E2: 58 [28%]) as the most bothersome symptoms. Symptom relief was apparent after four weeks of treatment (P = 0.053). After eight weeks of treatment, there was a statistically significant decrease from baseline in the mean score of the most bothersome urogenital symptoms, compared with placebo (P = 0.014) (Figure 2). The effects on subjective and objective parameters were sustained at week 52.
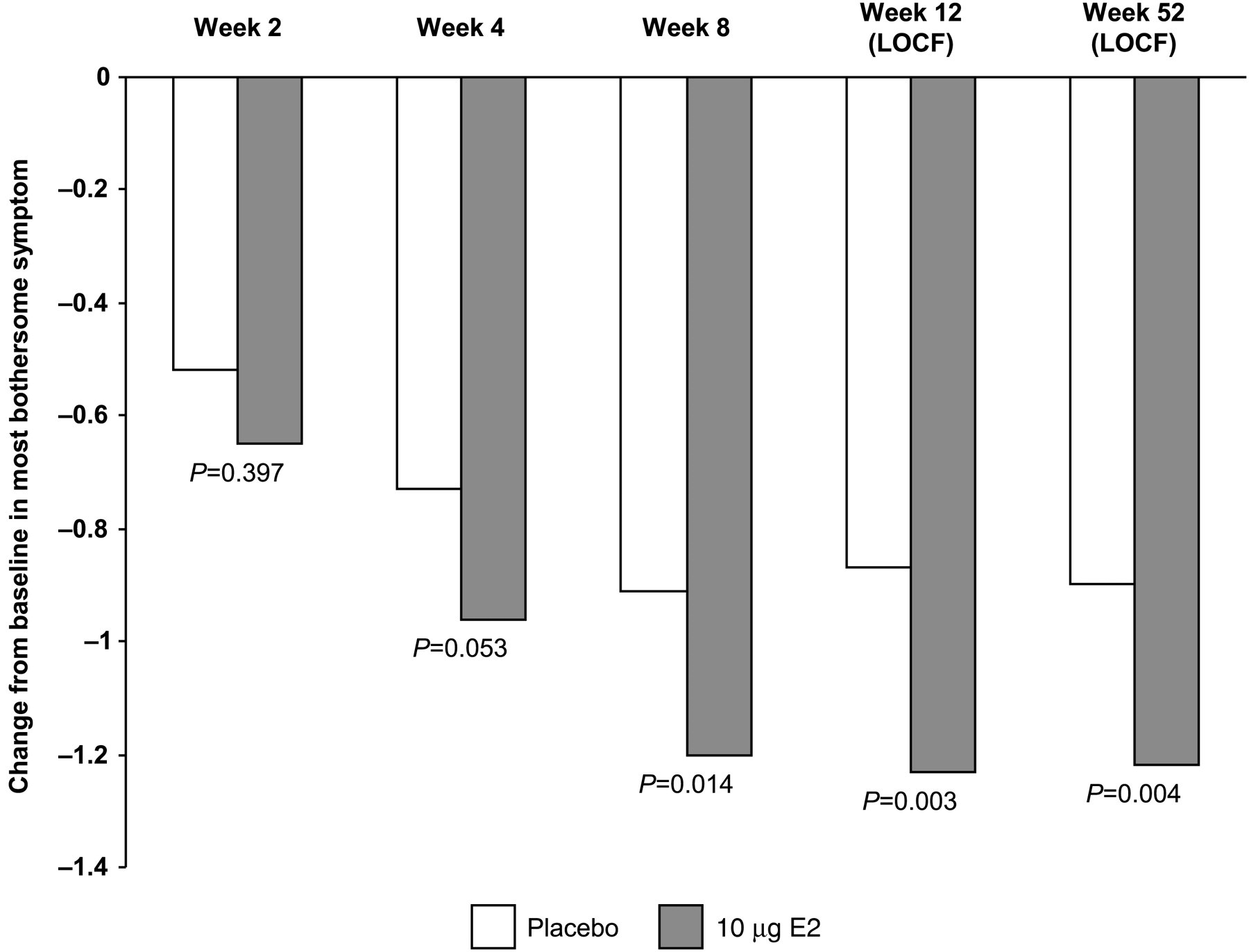
Change from baseline to week 52 in most bothersome symptom. P values are derived from the comparison between treatment groups. Data are reported for intent-to-treat analyses and missing values are imputed using the LOCF approach. LOCF, last observation carried forward; E2, estradiol
Similar proportions of participants reported adverse events (AEs) in the placebo and 10-µg E2 groups (75% and 77%, respectively). The most common AEs among placebo-given participants were headache and vaginal discharge. Vulvovaginal mycotic infection, vulvovaginal pruritus and back pain were more frequent in the 10-µg E2 group than in the placebo group. 15
In this study, seven participants (2.3%) reported a total of nine serious AEs (SAEs). In the placebo group, two participants (1.9%) reported three events (one gastrointestinal haemorrhage and two events of stent occlusion). In the 10-µg E2 group, five participants (2.4%) reported six events (pneumonia, infraorbital squamous cell carcinoma, endometrial adenocarcinoma [grade 2], ventricular extra systoles, gallstones and inflammation of the gallbladder). 15
This study demonstrates that the 10-µg E2 vaginal tablet significantly normalized vaginal pH and vaginal cytology profiles while providing significant relief of the participants' most bothersome urogenital symptoms shortly after initiation of therapy. 15
Endometrial safety
The systemic administration of unopposed estrogen has been shown to be associated with an increased risk for endometrial hyperplasia and carcinoma in a dose- and duration-dependent manner in postmenopausal women who have not undergone hysterectomy. 9,16 Few studies have investigated these risks with regard to unopposed vaginal estrogen. 2 Safety information, especially regarding potential long-term exposure associated with local estrogen therapy, is not well documented in published literature.
Endometrial safety of 10-µg E2 tablets was evaluated in a pooled population from two 52-week studies in which the incidence of endometrial hyperplasia and carcinoma was assessed. 17 Study 1 was a double-blind, randomized, parallel-group, placebo-controlled trial conducted in 309 postmenopausal women (205 treated with 10-µg E2) in North America, 15 and study 2 was an open-label endometrial safety trial conducted in 336 postmenopausal women in Europe. 18 Treatment regimens in the trials were identical. A 10-µg E2 tablet was inserted vaginally once daily during the first two weeks and then twice weekly for an additional 50 weeks, resulting in a total annual estradiol exposure of 1.14 mg.
Endometrial biopsies were performed at screening and at week 52, preceded by endometrial ultrasonography. In these two trials, an atrophic endometrium was defined as an endometrial sample with insufficient tissue for diagnosis and an endometrial thickness less than 4 mm, as determined by ultrasonography. 18,19
In the placebo group, the mean baseline endometrial thickness was 2.20 ± 0.87 mm and remained unchanged (2.16 ± 1.30 mm) at 52 weeks (last observation carried forward [LOCF]). In the 10-µg E2 group, endometrial thickness was 2.14 ± 0.90 mm at baseline and remained unchanged at 2.16 ± 1.26 mm at week 52 (LOCF) (Figure 3). 17
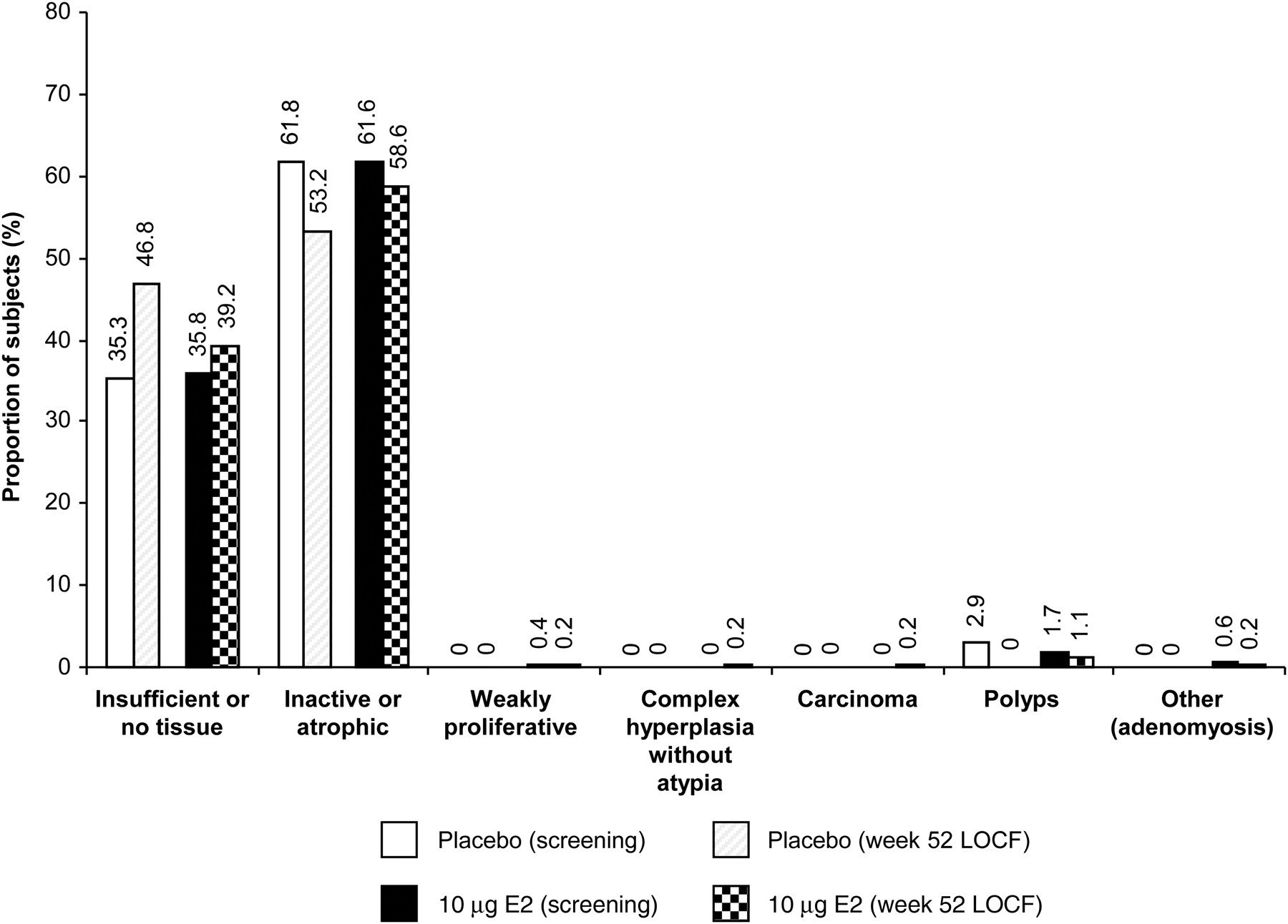
Endometrial biopsy results. Data are shown as the proportion of subjects with endometrial biopsy results. n = 102 (placebo, screening); n = 79 (placebo, week 52 LOCF); n = 537 (10-µg E2, screening); n = 469 (10-µg E2, week 52 LOCF). LOCF, last observation carried forward; E2, estradiol
During this study, a 62-year-old woman treated with 10-µg E2 for 324 days was diagnosed with endometrial adenocarcinoma (grade 2). The initial screening biopsy for this patient revealed ‘no tissue’ and was not repeated; therefore, it is unclear whether the carcinoma was present at baseline. It is unlikely that 11 months of exposure to the E2 administered in the trial could have induced this case of endometrial cancer. 15,17 It was subsequently determined that, prior to this study, the participant had received unopposed estrogen and methyltestosterone combination therapy to treat vasomotor symptoms for approximately two years, 17 and unopposed estrogen is associated with an increased risk for endometrial hyperplasia and carcinoma. 9,16 The risk for endometrial cancer caused by unopposed estrogen may remain elevated for more than 10 years, even after cessation of therapy. 20,21
Another patient was screened and then enrolled in the study, but subsequent blood work was inconsistent with the inclusion criteria and she was withdrawn from the study after only nine days of trial drug exposure. A follow-up endometrial biopsy was still performed and revealed complex hyperplasia without atypia, findings that were not seen at the screening biopsy. Since treatment duration was only a few days, this event was not considered related to 10-µg E2 treatment. 15,17
The background incidence rate of endometrial hyperplasia in postmenopausal women is 0–1%. 22 Across these two studies, the incidence rate for endometrial hyperplasia or cancer was 0.52% per year. 17 These results suggested no increased risk for endometrial hyperplasia or carcinoma in postmenopausal women undergoing treatment with 10-µg E2 vaginal tablets for one year.
Conclusions
Vaginal atrophy and its associated symptoms comprise a chronic condition. Estrogen therapy, including low-dose local estrogen therapy, is the most effective treatment for moderate to severe symptoms of vulval and vaginal atrophy. Because low-dose local estrogen therapy is not associated with endometrial stimulation, a progestogen is generally not indicated. 2,9,23 Long-term treatment is often required because symptoms may recur after cessation of therapy. 24 The current article summarizes the pharmacokinetics, effectiveness and safety of the ultra-low-dose 10-µg E2 vaginal tablets in treating and managing symptoms of postmenopausal vaginal atrophy, with a total annual estradiol exposure of only 1.14 mg.
The progressive nature of vaginal atrophy, including the persistence of symptoms in the absence of treatment and significant impact on quality of life, should encourage clinicians to engage routinely in an open dialogue with patients about urogenital health. These discussions will ensure that vaginal atrophy, whether symptomatic or asymptomatic, is recognized early and appropriately managed through treatment implemented before irrevocable atrophic changes can occur. 1
Competing interests
Nick Panay has lectured and acted in an advisory capacity for a number of pharma companies including Novo Nordisk. He has also received study grants from pharma companies including Novo Nordisk.