
Abstract
Endometrial cancer is the fourth most common female cancer in the UK and the most common gynaecological cancer. Quality of life and symptom control needs to be considered in women who enter a surgically induced menopause. Hormone replacement in this population has been controversial to date. The current evidence regarding the safety of estrogen only and combined hormone replacement therapy is discussed in this review. The use of topical vaginal therapies, alternate therapies and the current data regarding testosterone use for symptom control is also outlined.
Introduction
Endometrial cancer is the fourth most common female cancer in the UK, and the most common gynaecological cancer. The incidence is 22 per 100,000 women in the USA and 13 per 100,000 in Western Europe, mortality from which is approximately two per 100,000. In 2007, 7536 new cases of endometrial cancer were diagnosed in the UK, and approximately 1600 women die each year of this disease. Although endometrial cancer is in general a disease of postmenopausal women (93% occurs in women over 50 years of age), approximately 480 women each year will have treatment for endometrial cancer before the menopause. 1 The most common treatment for endometrial cancer is hysterectomy and removal of both fallopian tubes and ovaries, so all women will enter a surgical menopause after treatment, which can be challenging symptomatically. The role of osteoporosis prevention needs to be considered. Quality-of-life analysis and symptom-free survival need to take into account the risks and benefits of hormone replacement therapy (HRT).
We will review the available literature and discuss the different options of hormone replacement.
Epidemiology
Endometrial carcinomas can be divided into type 1 or type 2. Type 1 endometrial cancer is a slow-growing cancer, thought to be linked to the female hormone estrogen and obesity through the peripheral conversion of androstenedione to estrone in body fat. It accounts for 80% of cases. Type 2 endometrial cancer is a more aggressive, faster growing form of cancer that does not appear to have any connection with estrogen and accounts for around 10% of cases. Due to its more aggressive nature, the prognosis for type 2 endometrial cancer is less favourable and it may present at a more advanced stage. Cancer can also develop in the stroma and myometrium of the uterus and these cancers are called uterine sarcomas.
Women who receive tamoxifen have a three- to six-fold increased risk of endometrial cancer. 2 The risk rises with both increased dose and length of treatment, with treatment beyond five years increasing the risk at least four-fold. 3
The vast majority of endometrial cancers are sporadic, but hereditary non-polyposis colon cancer is responsible for 2-3% of endometrial cancers. It is inherited in autosomal dominant pattern and is characterized by a familial aggregation of colorectal cancer in addition to extracolonic cancers of which endometrial cancer is the commonest. The estimated lifetime risk of developing endometrial cancer in women carrying these mutations is around 30-60%. Importantly, in contrast to ‘sporadic’ endometrial cancer, women from such affected families usually develop endometrial cancer premenopausally.4–6
Postmenopausal HRT
This comprises of estrogen-only therapy (ERT [estrogen replacement therapy]) in women without a uterus, or as combined estrogen/progestogen continuous or sequential treatment (cHRT). The large studies have mainly investigated oral preparations. ERT and cHRT are used for the control of vasomotor symptoms, hot flushes, night sweats, which can significantly affect a woman's quality of life. Other benefits are the prevention and treatment of osteoporosis, protection against bowel cancer and possible protection against cardiovascular disease in younger postmenopausal women depending on the age of the women studied. 7
The Million Women's Study (MWS) and Women's Health Initiative (WHI) figures on the overall impact of HRT on cancers are usually quoted. The MWS comprises an increased risk of breast cancer (RR 1.26/CI = 1.00–1.59) with users of cHRT showing a higher risk than ERT; a decrease in colon cancer (RR 0.63; CI = 0.43–0.92) and a small increase in the risk of ovarian cancer with either cHRT or ERT (RR 1.20/CI = 1.09–1.32). With unopposed estrogen therapy, an increase in endometrial cancer has been shown (RR 0.83/CI = 0.47–1.47). 8 The WHI cHRT versus placebo study found that users had an increased risk of myocardial infarction, stroke, deep-vein thrombosis and breast cancer but a decreased risk of colon cancer. The WHI trial which looked at estrogen versus placebo found no difference in risk for myocardial infarction or colon cancer; an increased risk of stroke and thrombosis; and an uncertain effect on breast cancer risk. 9
However, these figures have recently been challenged by Shapiro et al.'s 2011–2012 studies. In the fourth paper, Shapiro concluded that the observational MWS did not meet several criteria for causality such as information bias, detection bias (the study did not exclude breast cancers that were already present), confounding (data such as age at menopause, menopausal status and body mass index was missing for 57–62%), statistical stability and strength of association or duration–response. The earlier papers suggested that the WHI and the Collaborative Reanalysis also could not satisfy the criteria for establishing causality. This epidemiological group concluded that ‘HRT may or may not increase the risk of breast cancer, but the MWS did not establish that it does.’10#x2013;13
A Cochrane review showed that unopposed estrogen therapy (ERT) will lead to endometrial hyperplasia and cancer with a reported odds ratio (OR) ranging from 5.4 (CI = 1.4–20.9) after six months of use, to OR 15.0 (CI = 9.3–27.5) at 36 months of continued use. 14 However, combined HRT can reverse established complex hyperplasia and sequential regimens require 10 or more days of progestogen therapy per month to be protective. A population-based cohort study followed up 40,000 women between 25 and 64 years without prior cancer for 15.5 years, to assess the risk of endometrial cancer with the use of hormone treatment. The risk was significantly increased for oral users but not for local low-potency estrogen use (OR 2.1, 95% CI 1.1–3.6 versus OR 1.5, 95% CI 0.4–6.2). 15
Sturdee et al. 16 found that sequential cHRT increased the risk of hyperplasia if given for more than five years. They also found that there was no increased risk of hyperplasia with continuous combined HRT.
HRT after endometrial cancer
Estrogen stimulates the endometrium, and many endometrial cancers have estrogen receptors within them, so the standard advice has been to avoid ERT in women with a past history of endometrial cancer. In women with severe or life-affecting menopausal symptoms, ERT has only been prescribed with informed consent after discussing the potential to stimulate occult residual disease. Due to a lack of evidence regarding the safety of use, patients with type 2 or grade III endometrial cancers have traditionally been advised to avoid ERT despite low rates of estrogen receptor expression.
Estrogen replacement
The only randomized control trial to date which compared ERT versus placebo in histologically confirmed primary stage 1 or 2 endometrial adenocarcinoma was undertaken in 2006. 17 As a minimum, patients were treated with total abdominal hysterectomy and bilateral salpingo-oophorectomy and entered onto the treatment pathway 20 weeks after surgery if they presented with menopausal symptoms. Endpoints were time to recurrence and all-cause mortality. Treatment was given for three years and follow-up was for a further two years. The sample size was 618. Originally the estrogen hormone treatment group was divided into patients with stage 1A, 1B/C and stage 2 cancers, but this yielded insufficient numbers statistically so the groups were joined together. In total, 2.1% (n = 26) showed recurrence, 12 were from the placebo group and 14 from the ERT group.
Forty-six women (3.6%) died; nine (0.7%) were a result of endometrial cancer, of which four were taking placebo and five ERT. This paper has shown no excess risk of recurrence after an average 36 months follow-up. This study was prematurely terminated following the WHI publication, and the majority of cases were stage 1A–C (1167 of 1236, see Table 1).
Evidence for estrogen-only hormone replacement therapy
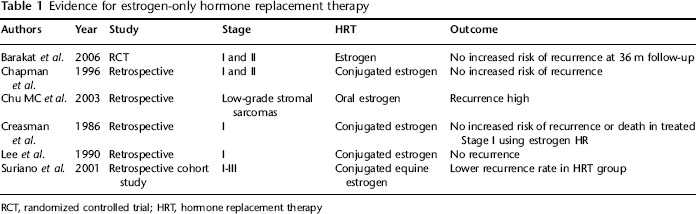
RCT, randomized controlled trial; HRT, hormone replacement therapy
This supported an earlier finding in a study by Creasman et al. 18 , 1986 of no significant excess risk of recurrent endometrial cancer in 47 of 221 women treated for Stage 1 endometrial cancer who were given estrogen-only therapy for a median time of 26 months.
Lee et al., retrospectively followed 44 patients after treatment for Stage 1 endometrial cancer who took ERT for a median of 64 months and compared them with 99 similar patients who did not take ERT. No recurrence occurred in the ERT group but only 23% started treatment within a year of surgery. 19 Chapman et al. 20 followed up 123 surgical stages 1 and 2 women; 62 of whom were given ERT from eight months postsurgery and found no significant difference in recurrence. Suriano et al. followed 75 women who had surgical stage I–III disease, excluding any sarcomas; 51% of whom took ERT and 49% of whom took cHRT and they compared these with 75 non-users. There were two recurrences in the estrogen-only group and 11 in the never users group. However, this study suffered from a small sample size, 85% had Stage 1 disease and women using HRT after treatment for endometrial cancer were more likely to have been HRT users pretreat-ment, which may have affected the tumour biology of the cohort. 21 These factors contributed to the need for Barakat et al.'s randomized control trial.
Progesterone replacement
Natural progestogens such as megestrol acetate have been used in the treatment of vasomotor symptoms in the non-oncological population. 22 There has been interest in its use as megestrol acetate has compared favourably to placebo in decreasing vasomotor symptoms. 23 However, there have been no studies to date looking at progesterone therapy for vasomotor systems following treatment for endometrial cancer.
Combined HRT
Combined HRT contains both estrogen and a progestogen. Small studies have looked at the use of this form of HRT in the endometrial cancer population. A study by Ayhan et al. 24 looked at 50 women receiving combined HRT after surgery, with no recurrences in the time of follow-up.
Topical estrogen
Topical vaginal estrogen has systemic implications for endometrial cancer. Haaften et al. 25 measured estrogen receptors in the endometrium, myometrium and vagina of 29 postmenopausal women. They looked at the effect of vaginal estriol (0.5 mg daily) compared with 17 beta-estradiol (0.05 mg daily) on these receptors and found biological and histological signs of estrogenic stimulation in all three tissues with no significant difference between 17 beta-estradiol and estriol. A Cochrane review in 2006 looked at local estrogens for vaginal atrophy in postmenopausal women. It concluded that there was a significant endometrial over-stimulation following use of the cream (conjugated equine estrogen) when compared with use of the estradiol-releasing vaginal ring. The ring also appeared to be favoured by women for ease of use and overall satisfaction with symptom control (P < 0.0001). 26 It should be noted that conjugated equine estrogen vaginal cream is no longer available in the UK.
Topical estrogen primarily has local effects on the vagina and a recent study of treatment with the vaginal estradiol tablet, Vagifem (Tm) (25 μg 17B estradiol) has been shown to significantly raise systemic estradiol levels, at least in the short term. 27 It would appear from these data that the systemic effects of topical vaginal estrogen are therefore greater than previously thought, so caution about their long-term use is advisable.
However, a randomized double-blind study in 2010 looked at the endometrial biopsies from 205 postmenopausal women who were either treated with a placebo or 10 μg of 17 β-estradiol vaginal tablets for 52 weeks. These data were then added to the results of 336 open-label biopsies. A total of 443 treated women were biopsied. In total, 85.6% of whom had atrophic endometrium, 12.6% had non-evaluable samples, 1.1% had polyps, 0.2% were weakly proliferative, one result showed complex hyperplasia without atypia and one was reported as endometrioid adenocarcinoma. The background rate of endometrial hyperplasia in postmenopausal women is less than 1% and therefore the study suggests that the use of low-dose vaginal estrogen may be safe. 28
ERT use after endometrial stromal sarcomas
There are minimal data in the literature regarding this rare cancer and the affect of hormones on the risk of recurrence. One small study investigating the use of ERT following endometrial stromal sarcomas showed an increased risk of recurrence even with low-grade cancers. Ten of 22 patients had recurrent disease, four of whom were treated with ERT. Of the patients given estrogen-only treatment, 80% had recurrent disease. 29 Further studies are therefore required to clarify whether ERT should be avoided after a diagnosis of stromal sarcoma.
Testosterone replacement
There are no data available regarding the use of testosterone after a diagnosis of endometrial cancer. Advice regarding testosterone would be based on evidence in the general population and can be offered for those women suffering from reduced libido and vaginal dryness. 30 Prolonged use of high-dose oral testosterones is associated with liver dysfunction and hepatocellular carcinoma31–33 and therefore transdermal patches with lower doses (300 |xg) and topical gels which avoid first-pass metabolism have been investigated and should be the preferred formulations. Improvements in libido and mood based on scoring a Brief Index of Sexual Functioning and the Psychological General Weil-Being Index were significantly higher than those taking placebo. However, there are insufficient data at present for use longer than six months.34,35
Alternative treatments
Asymptomatic women who do not wish to take HRT can aid maintenance of bone mass and cardio-protection by using strategies such as smoking cessation, regular sustained exercise (swimming and jogging), dietary advice and vitamin D and calcium supplementation if there are dietary deficiencies. Recent National Health Service government guidelines recommend that vitamin D supplements should be given to all women over 65 years of age. The Scientific Advisory Committee on Nutrition has suggested that vitamin D may be of benefit in reducing the risk of cancer, cardiovascular disease and multiple sclerosis and improving cognitive, neuromuscular and immune function. Although further research is required.36,37
Symptomatic women have found that alcohol, smoking, spicy foods and caffeine can trigger hot flushes. Aerobic exercise can improve mood and insomnia.38,39
Trials have confirmed that selective serotonin re-uptake inhibitors (such as venlafaxine and escitalopram) can help control hot flushes in some women.40,41 Evidence from randomized control trials about alternative therapies is poor regarding their effectiveness. Interest has been raised in populations whose diets are high in phytoestrogens such as red clover, black cohosh and ginseng due to their low levels of vasomotor symptoms. A Cochrane meta-analysis of 30 trials looking at phytoestrogens and vasomotor symptoms showed no benefit. 42 The use of these products has to be cautioned in women with hormone-sensitive cancers as most of the data on their estrogenic activity are derived from animal studies. Liver toxicity has been reported with black cohosh and gingseng has caused bleeding problems. The quality of the products offered is not well controlled either.38,43,44
Conclusions
The diagnosis of endometrial cancer has a profound impact on many women's lives. In addition to coping with the diagnosis and treatment, many women will seek accurate advice about the potential effects of hormone-based treatments on their risk of recurrence. Quality of life in the face of severe menopausal symptoms is an important consideration. In situations of risk (such as endometrial stromal sarcomas) hormone therapies should be avoided. Risk is often based on theory and extrapolation from data not relating to endometrial cancer recurrence. The literature that is available suggests that ERT does not significantly increase the risk of recurrence, but data are limited and are supported by only one randomized control trial to date.
The publication of the WHI and the MWS results has had a large impact on the perception of and use of HRT and ERT in the general population. HRT and ERT remain very effective at controlling vasomotor symptoms, which can have a significant effect on quality of life. Indeed, the recent studies by Shapiro and Howell would call the validity of the WHI and MWS results into question and advise caution in the advice given regarding risk of breast cancer. The evidence suggests that at least in the short term (no more than 5 years), it should continue to be prescribed in the general population. After five years, studies have shown a significant increase in breast cancer risk.8,9 Women need to be informed of the inherent risks of HRT, their baseline risk of recurrence or development of cancer and then be allowed to make decisions informed by their understanding of that risk. The current evidence suggests that this same approach could be applied to women who have had curative surgery for endometrial cancer.
While caution is appropriate, ERT may offer benefits for symptomatic women. A woman with a stage 1A endometrial cancer treated surgically with a recurrence risk of less than 2% may find it entirely acceptable to use topical estrogen cream for troublesome atrophic vaginitis. Women with a stage 1 or 2 endometrial cancer treated surgically could consider starting ERT up to six months after treatment to allow time to assess for symptoms and therefore whether there is a need for HRT. This also allows time to assess for early recurrence independent of HRT. At present, use for up to three years would be supported by Barakat et al.'s 17 2006 randomized control trial. Asymptomatic women who do not wish to take HRT should be advised on strategies that will aid in cardio- and osteoporosis protection.