
Abstract
Long-term outcome of psychological problems in childhood is important in a variety of ways including understanding disease entities, managing treatment and implementing research. It is of particular importance to courts in cases involving children. Judges have the unenviable task of determining best action for the future of children. Research is now available showing linkages between childhood and adult disorder but also revealing increasing complexity of factors determining outcome. A model of child to adult continuity can be constructed showing linkages between genetic influence, intrauterine environment, perinatal risks, early upbringing and lifetime risk and resilience influences. Known continuities of behaviours are traced from child to adult life. The presentation is intended to give a glimpse of some of the data available to assist in decision-making. Childhood determination of disorders such as schizophrenia may enable treatment to prevent further damage. Exciting developments particularly in genetics and functional imaging, will radically improve data over the next few years, possibly challenging currently held beliefs. At present expert witness contribution is under challenge but knowledge of the continuities can save court time, help prevent future heartache for vulnerable children, and later cost to the taxpayer.
Let us look briefly at one aspect of its connection with expert witness work with courts which at present is under fire with concerns about its cost. But there may be a good reason why expert witness work in the field of child and adolescent mental health became increasingly involved with court work from about the 1970s onwards. Prior to the 1960s, there was relatively little data on the outcome from childhood to adult life either from the presence of problems or as a result of what people did to children. There is for example even now ongoing confusion and lack of data as to whether smacking is harmful and abusive or useful in helping children to learn discipline.
A principal problem is the difficulty in obtaining good longitudinal data. Prospective studies, such as the Cambridge study, which identify a cohort of children born in a particular period and follow them for 30 years, have major problems both in terms of sample attrition but also in the ageing of the researcher. Retrospective studies selecting the sample in adult life and asking the subjects to remember their childhood illustrate the notorious unreliability of memory. I don't know if any of you have come across a very important book called Deviant Children Grown Up by Lee Robins, published in 1966? Apparently Lee Robins was walking past the Judge Baker Clinic in Boston, saw bundles of papers being thrown out and asked what they were. They were records from children who they felt were then far too old for the records ever to be relevant. She obtained those records, found the subjects and interviewed them. Good data independently at two points. This was probably the first two-point study that was able to give reliable data on children over a long period of time. I carried out the second two-point study using the records of Maudsley Hospital and correlating those from the children's department with those in the adult apartment.
As noted, one of the tasks of the courts is to decide what should or should not be done now in the light of what you think is then going to happen to the children as a result. That decision will affect the person for much of their life. Since the '60s, the data has been improving. Hopefully this assists judges in making decisions that are appropriate to reducing the probability of either further damage to the child in childcare cases or recidivism in child offending cases. If so then there should be a secondary effect of reducing subsequent costs which would more than offset the cost of obtaining an “expert” to provide the necessary data.
Can I ask if many of the people here are doing expert witness work? (Show of hands.)
Moving on to the subject of the actual continuities, the subject is enormous and I will have to romp through a variety of topics. I would like to just set the scene to start with. We are going to be looking at “Continuities”, and we can consider different sorts of continuities. There are problems resulting from the better longitudinal data now available, as for example, it has become increasingly apparent that diagnostic categories do not necessarily contain single entities and that indeed the childhood diagnostic categories include within them a range of relatively disparate clinical entities.
In the continuities we can look at causal factors, i.e. what causes something to happen, what causes a child to be aggressive? Secondly we can look at the child's behaviour over the years. If a child shows a particular behaviour, would it persist and will they show a similar behaviour in adult life? Thirdly, I am sure that the lawyers amongst you would pounce on me immediately if I didn't include the issue of vulnerability. What is it that can cause a person to be vulnerable to later disturbance even though it doesn't in childhood cause a manifest problem? This is very important because it gives the courts that I go to a really big headache if you say, “the child shows no current problems but will remain particularly vulnerable in the future.” The social service or court is likely to say, “If there is nothing wrong with the child manifest at the moment, don't do anything”, and then, when things do go very wrong some 15 years later, there is a law suit for £3 million for not having done anything.
We can also look at “Resilience” and what factors increase a person's capacity to deal with future adversity? There is again a very nice piece of work by Dahl and Dahl some time ago which showed that if a child met with adversity and successfully came through it, it wasn't such a bad thing, because in the future he or she was more resilient to future adversities as an adult. Unfortunately, the reverse is also true, and accordingly, if they met adversity and had difficulty in coping as a child, then they were particularly vulnerable to adversity in later life.
Figure 1 shows a simple model on which to base ideas about factors which affect children and their development. It is meant to represent the child with factors around the child that either protect or create risk. It is represented as three-dimensional as these factors change over time both in themselves and in the influence they have on children. The “child system” refers to such things as schools, clubs and even social services.
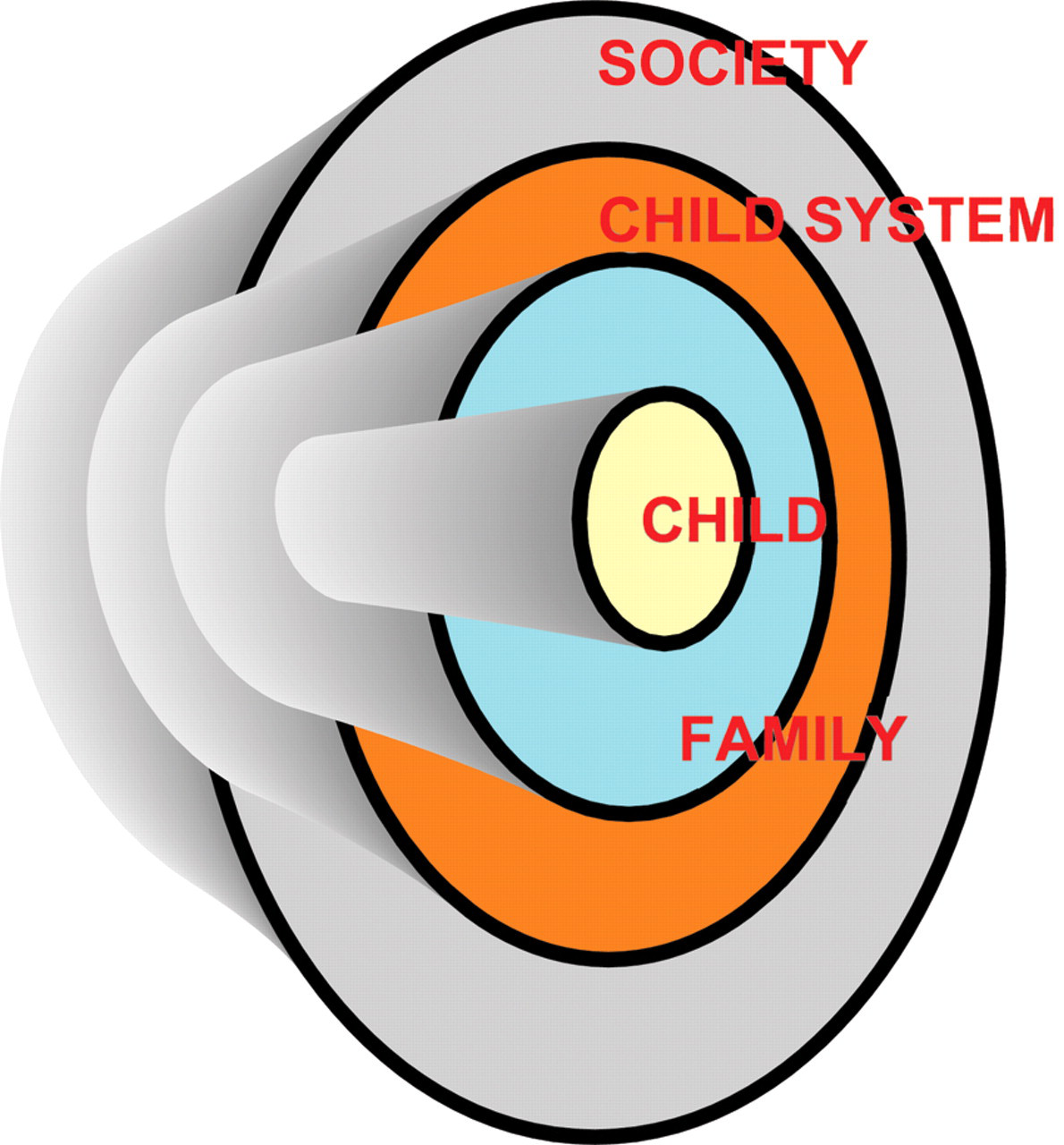
Simple model on which to base ideas about factors which affect children and their development
We have so far begun to look at the following major areas that are relevant in understanding child to adult continuity: behavioural continuities, causal factors, vulnerability and resilience.
I must now introduce the three huge social factors which cause tremendous problems and have overriding influences on the continuities from childhood and adult life:
Family breakdown; Drugs; Media.
Does everybody know the rate of family breakdown in most areas? I say family because there was this interesting statistic about six months ago which said that the rate of marital breakdown was falling. Does anybody know why it is falling?
Not so terribly long ago I was driving to a clinic and I heard a man on a phone-in radio programme talking about drugs and young people. He said, “They're all doing it”, and went on to say “… as they're all doing it, they might as well do it at home”. This was a broadcast and would act as an “instruction” to people in society. So I phoned him up, went on air, and said, “I really don't think you should say that, because the indications are, first of all, that just over 50% of youngsters do not do drugs. Why are you not talking about them? Secondly, there is good evidence that a really clear family ethos at home against drugs is protective. It doesn't prevent use of substances, but the rate is lower.”
He said to me over the air, “And on what authority do you say that?”
I replied, “Actually, I am a Professor of Child and Adolescent Psychiatry”, and he cut me off. What he presumably did not want broadcast was that he was talking rubbish and that there was value in a good family ethos against the danger of drugs to young people.
There is currently considerable pressure to legalise cannabis. There is an argument that the pathology induced by alcohol is far greater than the pathology induced by cannabis so let's make cannabis socially like alcohol! Can anybody explain the logic of that? If anybody has a good argument to say legalise it, please let me know and I will fight them outside.
In the past when lecturing in Asia I have found myself pointing out that it is reasonable to copy the West in some things, but their family system is better. So family breakdown is a huge problem. Yes, single parents can successfully raise children, but it's much harder.
The third major influence is the media. This can be educative but more often than not acts as an adverse influence increasing both antisocial behaviour and future vulnerability. It must be now something like 25 to 30 years since Belsen did his study on the impact of media violence, Television Violence and the Adolescent Boy. He showed very clearly that media violence induces violence in young people. The media also almost certainly increases inappropriate sexual behaviour and there is currently also evidence that it is increasing behaviour in young people that causes physical injury. Have we learned anything in the meantime? I regret that if anything the current situation is worse.
Let me move on to look at the observed behaviour and our diagnostic categorisation of that behaviour. As noted before, it is becoming more apparent that the diagnostic categorisations that we use are extremely primitive. An optimistic digression is that with the recent development of genetics, our increasing knowledge will give much better clarity about clinical entities, and using fMRIs (functional magnetic resonance imaging), we can begin to separate out genetically different problems and vulnerabilities and we can also (with functional imaging) begin to look at the brain and see how it functions. Our diagnostic categorisation is thus destined to change radically in the future.
We have looked at some important issues in continuities and interactions, now let us look at case histories: I have five very brief descriptions of cases that might help to illustrate some key points.
Case 1: boy of 15 before the courts for stealing from a store. Case 2: girl aged 14 before the courts for stealing from a store. Case 3: a child of four; depressed mother; absent father; tantrums and bruises; place with grandmother? Case 4: a child of six with severe tantrums, no friends and behind at school. Parents doubt that they can continue to cope and are looking for respite. Case 5: A girl of seven, parents separated, child with mother; parents battling over residence and contact.
Cases 1 and 2 are a boy and a girl of similar ages who at face value did the same thing in stealing from the store. I have said before, the best continuities can be seen in the actual behaviours, but Cases 1 and 2 illustrate the difficulties that exist with that. They both stole but were not actually doing the same thing as one another. The girl stole a wall ornament and took it home; when I asked her mother what she then did with it the mother replied that she had “put it on the wall, of course”. The girl was normal but conforming to an antisocial environment. The boy picked up an ornament and wandered back home. He was losing his appreciation of thought connections and was developing a psychosis.
Case 4 is one that I would like to come back to right at the end, because this young man I followed, almost accidentally, for 13 years, so I know what happened to him, and it was something surprising. Case 5 is a very common problem of acrimonious parental separation that preoccupies the courts and for which we are currently trying to raise money for long-term outcome research. The indications are that such contact disputes damage children but we need more clear evidence. It is a problem which I deal with every day. Does anybody know the Philip Larkin quote by Lord Justice Wall relevant to that?
They **** you up, your mum and dad. They may not mean to, but they do. They fill you with the faults they had And add some extra, just for you. But they were ****** up in their turn …
Shall I say that I know that particular case very well. It illustrates not only that the family environment is a modifying factor to the long-term continuities but also that the continuities may extend over more than one generation.
The various factors that we have considered that affect long-term continuities can be incorporated into a system diagram that tries to represent some of the interactions, Figure 2.
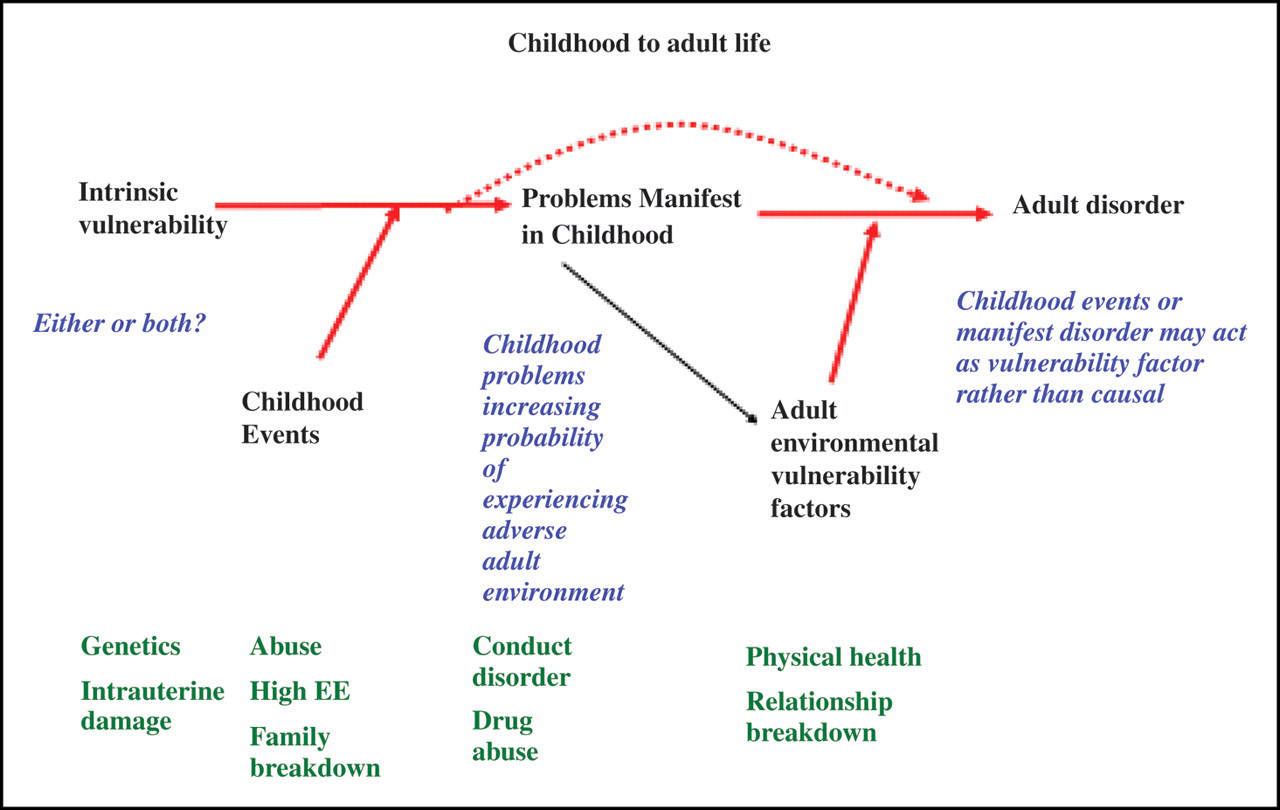
Interactions affecting long-term continuities, childhood to adult life
The model endeavours to illustrate various influences on continuities both phenomenological and diagnostic. We should perhaps start with genetics on the far left. We can look at a range of influences that are going to make a difference to both the manifestation of problems in childhood and also to the likelihood of continuity. We can look at what makes a difference as the child gets older and we can look and see that there is a rather curious paradox. The earlier the adverse influence on a child, the more profound the pathological effect. By the same token, the younger the child and the more definitive the intervention, the more you can do about it. Once you get a youngster who has been with a conduct-disordered peer group, by the time they are 12 or 13 you really, really are up against making a difference if you intervene. Has anybody got experience of working with severe conduct-disordered young teenagers?
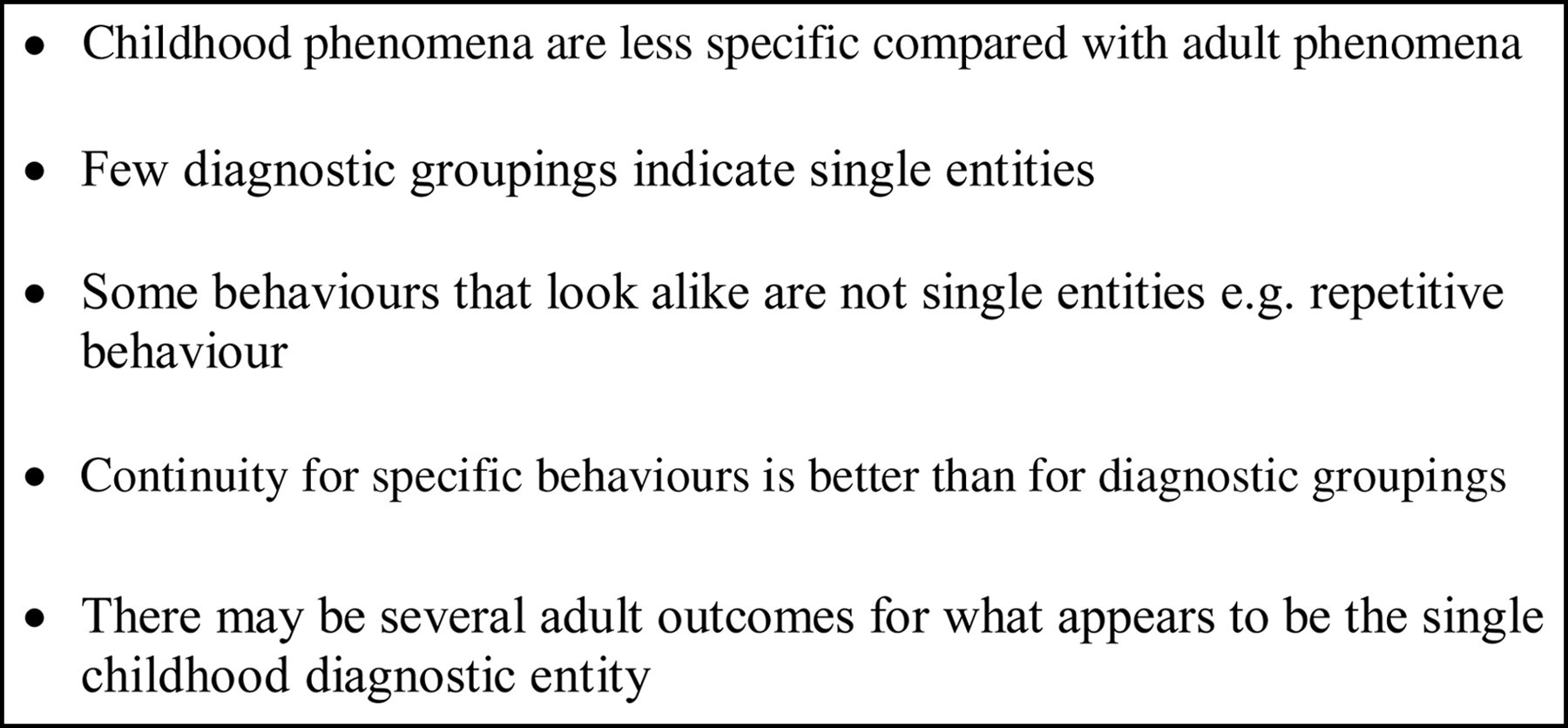
The following chart, Table 1, lists some of the available data with regard to specific behaviours and behavioural patterns.
Rudiments of psychological damage: prognosis
I thought, because of the limitation of time, we could take a look at one or two things that we can identify. What about anxiety? We can see overall the children who show anxiety are likely to be anxious as adults. However we need to be careful as anxiety is a normal phenomenon and moderate degrees of anxiety may actually improve task performance. It is only associated with dysfunction if it is severe, situationally specific or sustained at a high level when it serves no purpose.
If we look at obsessive disorder, OCD, overall there is a relatively poor prognosis with some 50% continuity into adult life. However the longitudinal data also indicates that not all problems of repetitive behaviours are the same phenomenon. For example, the repetitive behaviours of Tourette's syndrome may generally look like OCD though the actual phenomena have somewhat different characteristics. Recent studies have even questioned whether Tourette's syndrome is a single entity itself.
Aggression is also very interesting. Lee Robins in her book said that if there is aggression and violent behaviour in childhood, it predicts violence in adult life, and one researcher, Olweus, confirmed that. She also said that the absence of aggression and violence predicts the later absence of aggression in adult life, and to a large extent this is true, unless you start looking at psychosis, because aggression can be a precursor for schizophrenia. Children who refuse to go to school may not show overt aggression in childhood but may become increasingly violent when resisted in their teens. I had a telephone call from a parent who said, “You saw my youngster who was refusing to go to school four years ago when he was 13. He is now 17. He is in a secure unit. He is due to come out and he is threatening to come home and murder us.” The exceptions to continuities are also important. So overall there is strong continuity from childhood violence to adult violence, Conduct disorder continues to antisocial personality but the exceptions are important to note. Figure 3 summarises some of the points with regard to this.
Long-term significance of childhood phenomena
We can see from the data that there are patterns of continuity but also a variety of confounding factors that need to be taken into account. For expediency, Figures 4 and 5 list some of these in terms of vulnerability factors and resilience factors.

Rudiments of psychological damage
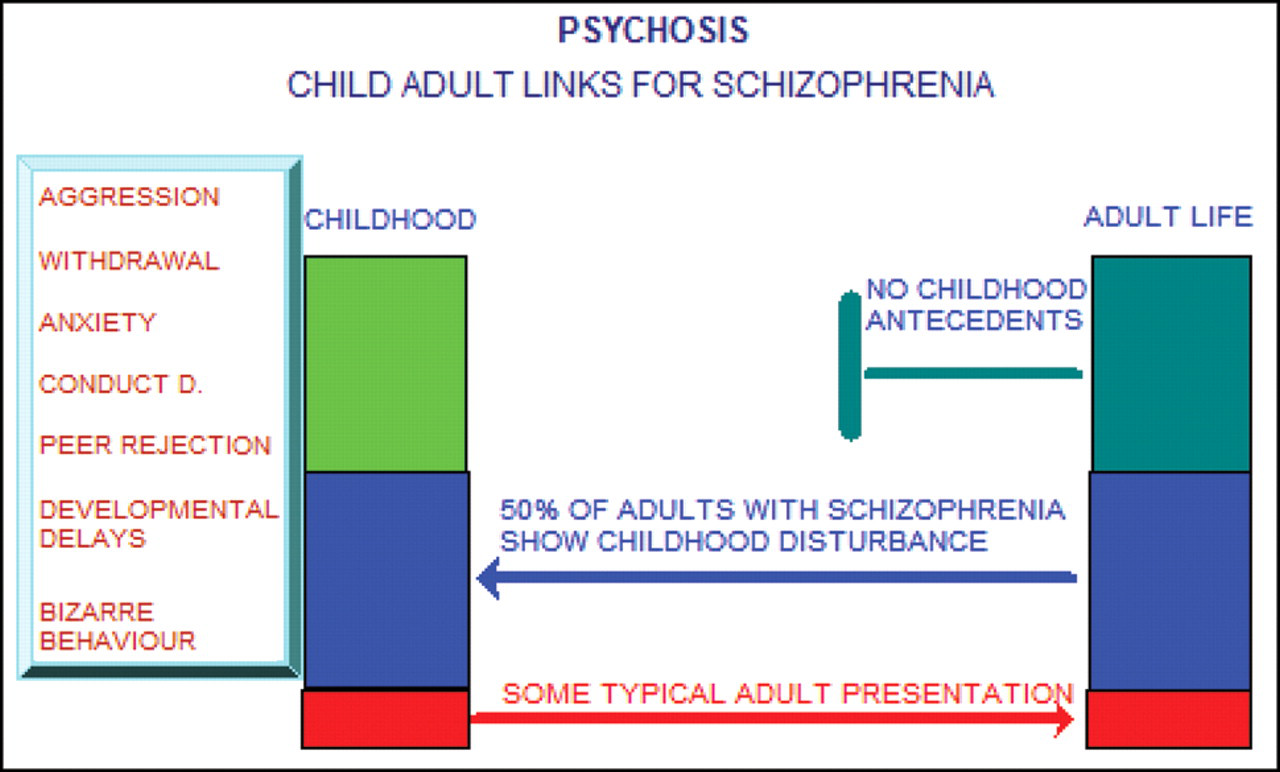
Child adult links for schizophrenia
Figure 4 shows some of the environmental factors that influence outcome. We can look at things like the impact of maternal bonding. A little bit of data: pregnant women in refuges do not transfer their maternal-fetal bond so well to maternal-infant bond when they deliver their child. Is it because they are in the refuge in the first place or could it be that there is an adverse effect when in the refuge? Maternal bonding and disorders of disruption of that bond are not only increasingly interesting, they are increasingly complex as well.
Moving on fairly quickly, I am going to pick out “a good relationship with mother and father”, but please note that relationships with mothers and fathers are different. It is quite interesting that there is a huge denial that there are essential differences in the psychology of men and women, but in fact it is a very important difference. Grotevant, who was one of the people who started writing about this, noted that women are much more easily able to allow intrusion into their own psychological sphere than men. That doesn't come as any surprise to women but is usually resented by men. However, most men don't have a youngster starting within themselves. With very young children the relationship between mother and the infant up to about three or five is a very important one. That does not deny the importance of the father and father's role in later behavioural modelling and involvement in the parental system around the youngster.
Identity and identity formation is another important factor in determining children's continuity of behaviour. There is a risk that we actually encourage persistence of behaviour. In most of our work there is pressure to identify people by the difficult behaviours that they show. Doing that risks inducing a pathological identity. I got into a big argument about this at a meeting in San Diego. It was being pressed that our job is treating disease, and it was not unreasonable to identify youngsters by the problem: “I saw a schizophrenic today.” That attitude makes matters worse. It is extremely important to work hard with young people to induce a process of normalisation. One youngster – he was a pleasant, big lump of a lad, but something happened, he got into an argument and he picked up a knife. He had never done this before. He wasn't a violent youngster. What happened immediately was everybody jumped on him. They said, “He's violent, he's an aggressive, dangerous chap.” When I spoke to him I said, “Tell me about yourself”, and he thought, and he thought, and he said “Well, I suppose I'm violent.” We need to be very careful that we give at least as much emphasis to young people's assets and positive skills and have a process of normalisation. I am afraid doctors/psychologists are very good at pathologizing.
Conduct disorder, antisocial behaviour, is a big, big problem. I am going to go through it very, very quickly, but it is a major problem in our society. It is something for which we tend to put responsibility on to other people but for which we should take personal responsibility. The more we can have an ethos which is against antisocial behaviour, the better. Remember that I discussed the two different cases of a boy and a girl both of whom took things from a store. The boy actually was losing his appreciation of social rules; he was developing a psychosis. His future will be that he will be under treatment, and in good hands he will be able to function. There was nothing wrong with the girl – there will be – because she was behaving appropriately to the social environment in which she was living. She will show increasing antisocial behaviour; she is at high risk. Same behaviours, two different outcomes probably in the opposite direction to the one that you expected.
We can start to look at the very, very powerful factors to do with conduct disorder. An important predictor of conduct disorder is pervasiveness. If we are advising courts, we tell them that the more pervasive it is in terms of range of behaviours, the longer it has been present and the more pervasive it is in locations, then the longer it is likely to persist. So a youngster who nicks something from you on one occasion at home – worry but don't go over the top – is very, very different to the youngster who is doing it regularly.
Five months ago we had a youngster, a girl, who was going out at night and coming back with more money than she went out with, and I reported it to the Social Services and they said, “Oh, kids do that.” Her behaviour was regular, repeated and persistent. She was a 13-year-old prostitute – this was persistent, regular and repeated behaviour. Her outlook is terrible. As I have said, conduct disorder has a 50% continuity into adult life, childhood pervasiveness of the behaviour can help us predict which children will be in each of the 50% areas.
The question is: where are we going from here? It is very likely that better understanding of the continuity data will be an important factor in changing our concepts of single disease entities. Schizophrenia probably isn't an entity. Could any adult psychiatrists here help! Is there a likelihood that what we classify as schizophrenia is a single entity? Almost certainly not in childhood; it's probably a mixture of things. However, its presentation before 16 is about 0.5% of the population. If anybody thinks that is rare, be clear that it is not – that is an awful lot of young people.
There is increasing interest in early intervention and often with little regard for what is known of the progressive changes in continuities between childhood and adult life. Most such programs look at the early presentation of the adult phenomena rather than at the childhood phenomena that continue on changing into the adult disorder.
There is longitudinal data which shows that if you have the combination of behaviours on the left in Figure 5, none of them specific – none of them clearly psychotic behaviours, except perhaps the last one, bizarre behaviour – you have a worse prognosis, and the question is, can we do anything? Can we identify them and change the course of events? Case 4 in my list was a boy who presented at about the age of six. I followed him for over 15 years. It was extremely difficult to alter his behaviour initially. The older neuroleptics produced an improvement but also very marked side-effects. Atypical neuroleptics gradually enabled him to function with much more appropriate and social behaviour over a period of about six months. Annual trials off the medication caused marked relapse and as he matured he showed more typical signs of schizophrenia. What was remarkable was that we were able to maintain his well state with a very small dose of the neuroleptic. It is extremely exciting to think that early intervention may prevent secondary damaging compensation in the brain for the disordered thinking.
Any orthopaedic surgeons here? If you have a bad foot and you limp the whole time, you will compensate and you are likely to develop a lateral curvature of the spine; a normal spine now becomes abnormal. In due course the abnormal use and position of the spine will generate its own problems. When I first came into medicine it was accepted that the brain was fully formed at birth. It then became apparent, with better studies, that there is still neurone change for a significant period of time after birth. There is now growing evidence that usage actually changes brain structure and systems. There is evidence that this is correct with regard to the social functioning in people with early-onset disorder, and is likely to be so also for some organic functions of the brain. It is possible therefore that early identification of long-term disorder and its early treatment can prevent some of the abnormal functioning.
Turning to ADHD (attention deficit hyperactivity disorder), this condition has a good outlook. We did a two-year follow-up. We looked at youngsters at 13 and 14 and followed them to GCSE, and children with treated ADHD did just as well, ability for ability, as the rest; but if they were co-morbid with antisocial behaviour they did badly, really badly. Twenty five percent of young adult males in prison have evidence for ADHD. That is roughly five times the general population. Should the courts, interventional courts, be able to say not “You will have treatment”, but “You must have a trial of treatment so you can see what it does for you”? If we catch the youngsters early enough can we prevent them becoming recidivists?
So I am going to say both for lawyers and for those in my field that there are going to be some extremely exciting times ahead. A better knowledge of long-term outcome combined with some of the newer techniques such as fMRI and the advances in genetics are likely to enable us to have much better identification of clearly defined entities that are currently within relatively crude and almost certainly heterogenous diagnostic categories. Hopefully our knowledge of long-term outcome will also help us identify the best means of early intervention and prevention of secondary damage.
Discussion
Footnotes
*
Charles Bell's father was a clergyman and his brother a surgeon but that does not alter the issue of identified positive skills giving resilience to young people in adverse environments.