
Abstract
Lipomatous hypertrophy of the interatrial septum (LHIS) is a benign cardiac mass characterized by fat accumulation in the interatrial septum. It may represent an incidental autopsy finding or may be associated with atrial arrhythmias, obstructive symptoms or sudden death. The case described here is a peculiar case of sudden death secondary to LHIS.
Introduction
Lipomatous hypertrophy of the interatrial septum (LHIS) is a rare pathological finding characterized by the deposition of mature adipose tissue near the interatrial septum together with epicardial fat. 1 These lesions arise more frequently in obese, elderly and female patients; usually, the lesion involves the front or upper portion of interatrial septum, sparing the oval foramen and protruding into the right atrium. On average, the septum shows thickening of up to 2.5 cm (the normal thickness of the septum is less than 1 cm and the upper limit of a normal septum is about 2 cm); however, cases of tumours with a diameter of more than 10 cm have been reported. 2
From the histopathological point of view, unlike a real lipoma, LHIS consists of an area of non-encapsulated deposit of fetal and mature adipose tissue, together with atypical myocytes. Hence, the word hypertrophy is an incorrect term since the pathology consists of the increase of adipocytes and not of their increased dimensions; therefore, probably it is better described as hyperplasia. 3
Usually LHIS is an incidental finding and mainly asymptomatic, but it can be associated with supraventricular arrhythmias or flow disorders (according to the hypertrophy level), changes in P-waves, obstruction of superior vena cava and sudden cardiac death. 4,5
In the past few years, the rate of ante mortem diagnosis has been increasing, thanks to several new non-invasive techniques such as the two-dimensional ultrasound, computerized axial tomography (CAT) and magnetic resonance imaging that have allowed clinicians to make a timely diagnosis, even if a biopsy is sometimes required. 6,7
We present a case of the sudden death of a 74-year-old man, seemingly healthy, whose postmortem examination showed the presence of LHIS, but no other pathological findings.
Case report
A 74-year-old man (body mass index [BMI] = 27), was found dead in his home. The recent and past medical histories were negative. The external examination revealed the presence of small, multiple excoriations on his face, due to the fall that resulted from his sudden death. The internal examination showed no pathological abnormalities, with the exception of the heart, that weighed 445 g. The valvular endocardium was slightly thickened with fibrocalcific areas; there was hard-elastic thickening of the interatrial foramen measuring 5 cm × 3.5 cm and a thickness of 2.7 cm, causing deformity of the interatrial septum (Figure 1a). On dissection, the tumour had no capsule, was white-yellow coloured with reddish stippling. The coronary arteries showed no relevant atheroma or lumen stenosis; the myocardium presented no important morphological changes. The histological examination of the tumour detected the presence of adipose tissue, mainly mature and only locally fetal, where small groups of myocardiocytes were found (Figure 1b). These were mostly hypertrophic and with local sarcoplasmic vacuolation; myocardiocytes were associated with interstitial fibrous tissue, where few lymphocytic infiltrates were found. The toxicological examination results were negative.
(a) Gross photograph of the fatty deposition confined to the atrial septum, discovered at postmortem examination. (b) Mature adipocytes and vacuolated fat cells, with interspersed hypertrophied myocytes.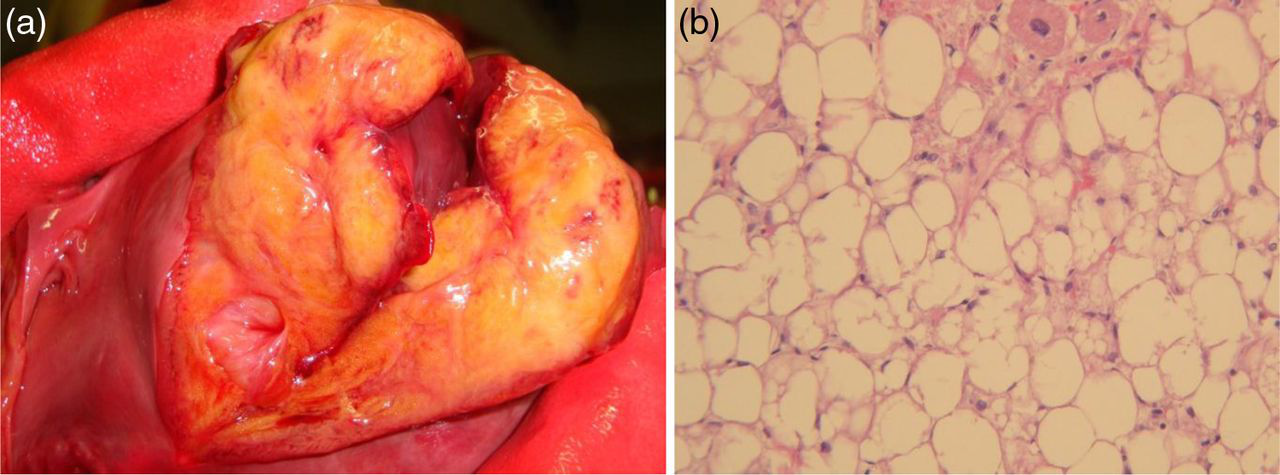
Discussion
LHIS was described for the first time during an autopsy in 1964, carried out by Prior; 8 since then, several cases have been reported in postmortem studies. The incidence of LHIS during postmortem examinations is about 1%, 9 while in vivo studies have shown a rate of 2.2%. 10 A study was carried out by AFIP (Armed Forces Institute of Pathology) 11 that analysed clinical and pathological reports of 45 patients presenting abnormal depositions of adipose tissue at cardiac and pericardial levels. Thirty-two turned out to be affected by LHIS; in 28% of the cases, death seemed to be directly connected to the atrial neoplasm. The patients died a sudden death or, after prolonged episodes of atrial or ventricular arrhythmias, congestive cardiac decompensation refractory to therapy. Clinically, it was not possible to confirm the aetiology of cardiac symptomatology for each and every case, and during the autopsy no other cardiac malformation or pathology were detected, with the exception of LHIS.
LHIS can be associated with the development of atrial arrhythmias: atrial fibrillation, premature complexes, supraventricular tachycardia, ectopic atrial rhythm, and connecting the rhythm to sudden death. 12,13 This association is understandable because the fat deposition is often located in the area where the sino-atrial node is, or where the ventricular atrium passes, next to the front portion of interatrial septum, entailing transmission anomalies or interference with the structure of atrial myocytes. 14 These changes cause the development of a P-wave, near the shunts II and III and causing atrio ventricular fibrillation (AVF), with very peculiar characteristics with “dome and dip” shapes. 2 The incidence of atrial arrhythmia is directly connected to the fat thickness at septum level.
The case presented here is, in this context, distinctive since death was sudden and totally unexpected. It was instant – as is typical in serious cardiac arrhythmias, where there are no other pathological conditions present and the toxicology results are negative. Considering the LHIS dimensions (5 cm × 3.5 cm × 2.7 cm) and the location (next to the atrio-ventricular sinus junction) we can conclude that this caused the development of the malignant arrhythmia that resulted in this man's rapid and unexpected death.
In conclusion, we think that clinicians need to know about this kind of pathology, to provide a more accurate ante-mortem diagnosis made possible by non-invasive diagnostic methodology such as echocardiogram and CAT and which should result in appropriate treatment. Also forensic pathologists need to be aware that in some cases LHIS can be the cause of death.