
Abstract
A review of negligence reports, detailing 227 complaints from the practices of two orthopedic surgeons, was undertaken. There were demonstrable differences in the number of complaints over leg-length discrepancy; femoral fracture and cup malposition when cemented versus uncemented implants were compared. Surgeons must appreciate the less forgiving nature of uncemented hip implants and the importance of preoperative planning particularly in the presence of abnormal anatomy.
Introduction
Total hip arthroplasty in the UK is performed in ever increasing numbers with 87,000 procedures undertaken in 2010/11 across England and Wales. 1 Total hip replacement has long been recognized as among the most beneficial procedures for quality of life. Levels of expectation are changing; as well as being relieved of pain, patients now expect to be able to get back to high levels of activity, including sport. This changing level of demand and patient expectation is likely to be related to the growing number of litigation cases following complications of hip replacement.
A review of cases from the British National Health Service Litigation Authority (NHSLA) attempted to analyse the complications leading to litigation. 2 Of the cases with adequate data they found that 21% involved sciatic nerve damage, 16% leg length discrepancy, 8.5% infection and 6.8% femoral fracture. Reports via Freedom of Information Act requests have highlighted the practice of the NHSLA and shown the cost of orthopedic-related claims between 2006 and 2008 to be in excess of £6.85 million.3,4 The nature of the claims appeared to be evolving over recent years - fewer claims were for deep infection, with a greater proportion over deficiencies of surgical technique including consent, fracture, component malposition, dislocation and leg length discrepancies. 4 Experience from the USA appears similar, wherein a review of litigation following hip and knee arthroplasty demonstrated nerve injury as the most common citation, followed by limb length discrepancy, infection, vascular injury, hip dislocation, compartment syndrome, deep vein thrombosis, chronic pain, and periprosthetic fracture. 5
In an attempt to better understand the types of complication which lead to a complaint, we undertook a review of 167 consecutive negligence claims. We also examined the data for a correlation between negligence claims and the choice of implant fixation; be they cemented or uncemented. The medicolegal practices of two orthopedic consultant surgeons were studied.
Materials and Methods
All the medicolegal case files of two practising orthopedic consultant surgeons between 2003 and 2009 were reviewed. The inclusion criteria were any negligence claims pertaining to total hip arthroplasty, including reports for claimant and defendant. One hundred and sixty-seven negligence reports were included in the study, whether the claim was successful or not. In all instances the report had been compiled in accordance with the guidelines laid down by the Expert Witness Institute and Civil Justice Council. The principles of the Bolam test were applied in each case, 6 which states that a doctor is not negligent if he acts in accordance with a practice accepted at the time as proper by a reasonable body of medical opinion, even though other doctors may adopt a different practice.
Liability and causation plus condition and prognosis reports were analysed, as were the examination findings and radiology reports. The reason for which each case was brought was identified and classified into one or more of the following categories; infection, nerve damage (and which nerve), leg-length discrepancy, pain, fracture, cup malposition and stem malposition. Most claims had more than one complication. The surgical approach, implant type and fixation technique used was recorded. We analysed the data to identify any association between these parameters and identified complications.
Results
The data for the 167 claims are displayed in Table 1. There were a total of 227 different complaints. Forty-eight were in relation to a nerve injury, 39 leg-length discrepancy, 31 dislocation, 25 fracture, 25 infection, 42 cup malposition and 17 relating to a stem malposition.
Raw data
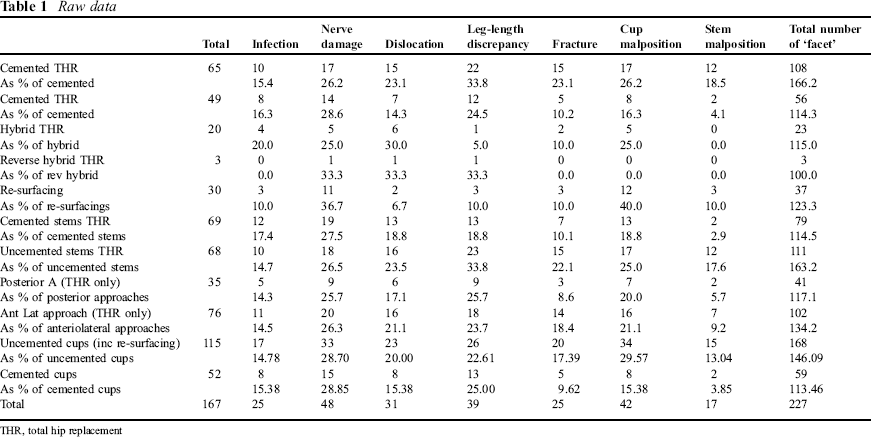
THR, total hip replacement
Of the total hip replacements, a posterior approach was used in 35 and an anterolateral approach in 76. The approach used was not recorded in the remaining 26 cases. There were 65 all cemented, 49 uncemented, 23 hybrid (20 cemented stem, uncemented socket and three uncemented stem, cemented socket) and 30 hip re-surfacings. Further breakdown of the figures showed 69 cemented and 68 uncemented stems, with 52 cemented and 115 uncemented cups. One hundred and twenty-seven complications were identified with cemented stems and 158 with uncemented stems (Figures 1 and 2).
Case mix

Technique

The data were then analysed via a one-tailed Fisher's exact test to examine for significant differences between the sample groups. Three different groups were analysed namely stem (uncemented versus cemented), cup (uncemented versus cemented) and surgical approach (posterior versus anterolateral).
Stem fixation analysis showed no significant difference between uncemented versus cemented fixation with regard to infection, nerve damage or dislocation complaints. However there was a significant difference (P = 0.035) between the groups for complaints over leg length (23 of 68 uncemented stems versus 13 of 69 cemented stems).
Statistical significance was also demonstrated in complaints concerning femoral fracture (P = 0.047) and stem malposition (P = 0.004). Cemented stems attracted fewer complaints per case in both of these categories (Figure 3).
A comparison between cemented and uncemented stems
Analysis of cup fixation showed no significant difference between uncemented versus cemented fixation with regard to infection, nerve damage, dislocation or leg-length complaints. However there was a significant difference (P = 0.036) between the groups for complaints over cup malposition (34 of 115 uncemented cups versus 8 of 52 cemented cups).
There were significantly more claims made for dislocation and a leg-length discrepancy in patients having total hip replacement than in those having re-surfacings (Figure 4). Patients having re-surfacings did however have significantly more claims relating to cup malposition and, although not significant, a higher percentage of claims for nerve injury.
A comparison between complaints for re-surfacings and total hip replacements

Analysis of resurfacing versus total hip replacement showed significantly higher incidence of cup malposition (P = 0.03). There was a significantly lower incidence of dislocation and leg-length issues (P = 0.04 and P = 0.04). Other complaint types showed no significant difference (Figure 4).
Statistical analysis of the surgical approach revealed no significant difference between the number of complaints with regard to the claims around infection, nerve damage, dislocation, leg-length discrepancy, fracture, cup or stem malposition.
Discussion
The fixation technique in this data-set is comparable to national practice in England and Wales. The 2011 NJR figures showed 50% of implanted stems were cemented with 50% uncemented in primary hip arthroplasty. 1 This data-set also showed 50% of each. Similarly for cup fixation, the NJR report shows cemented cups made up 35% with 65% uncemented. This data-set showed 38% and 62% cemented and uncemented cups, respectively, exclusive of re-surfacings. With regard to re-surfacings, there was a much higher proportion of claims made in proportion to that expected from the NJR data. In our data, 18% of claims related to re-surfacings; only 3% of all total hip arthroplasty were re-surfacings.
In this series it is notable but not statistically significant that cemented stems resulted in a lower proportion of facets to each negligence claim when compared with uncemented stems. While it is difficult to draw useful conclusions from this, the analysis of the different types or facet to each claim did reveal some points of note. Whether the stem was cemented or uncemented did demonstrate a significant difference with regard to leg-length complaints, fractures and stem malposition.
It is inherent in the nature of uncemented stems to be less forgiving at the time of implantation. Depth of insertion can be difficult to control to the level planned preoperatively, leading to leg-length discrepancy. Intraoperative femoral fracture is a well recognized risk with both cemented and uncemented implants, which if not detected can be catastrophic. The National Joint Registry for England and Wales reported a higher incidence of intraoperative fracture in uncemented total hip replacements. 1
There were significantly more claims related to cup malposition with uncemented rather than cemented cups. While it is beyond the scope of this paper to comment on how malposition was defined and then determined, the literature suggests that it is more difficult to implant the acetabular component in the planned position with uncemented fixation, whereas the use of cement may give the surgeon more control over final implant position.7,8
Of the data gathered on re-surfacings, the worse record for complaints over cup malposition is in keeping with the apparently lower tolerances to this implant type. This has been shown with numerous resurfacing designs - most notably perhaps with the voluntarily recalled articular surface replacement (ASR) from DePuy (ASR; DePuy Leeds, UK). 9 As expected there were fewer re-surfacings with issues over dislocations or leg lengths.
When surgical approach was studied, there was no significance between number of complaints over nerve damage, dislocation, leg-length discrepancy, fracture, cup or stem malposition. A number of possibilities may explain this finding. Preoperative factors such as fastidious consenting may mean surgeons are more likely to mention sciatic nerve damage, while precise intraoperative practice will note the identification and protection of the sciatic nerve and hence avoid a subsequent claim. Again although not statistically significant it is also interesting to note the apparently higher rate of claims over infection in cemented implants, which would be contrary to popular opinion. Also of interest is the unexpectedly large number of cases when the surgical approach used was not recorded. At the very least this is a lamentable reflection on the quality of operation notes and indeed medical record-keeping.
It must be emphasized that these data are not a representation of the incidence of complications, but reflects the type of complications leading patients to make claims against surgeons for negligent practice. As a tool for learning from our mistakes, this perhaps again serves to highlight the variety in surgical practice and indeed outcomes. This study does highlight the types of complication which are likely to result in litigation claims. In particular we highlight the potential pitfalls with uncemented fixation, notably leg length, fracture and component malposition. Also raised is the need for careful preoperative planning, appreciation of the limitations of certain implants for varying anatomy, and care to avoid these complications.