
Abstract
Organ transplantation significantly improves the health, quality of life and life-expectancy of people whose organs have failed. Most patients in the UK cannot enjoy the benefits of a transplant because of an extreme shortage of organs. This paper demonstrates the magnitude of the problem of organ shortage and identifies possible causes. The current UK legislation regarding consent to organ transplantation is analysed and compared with other jurisdictions. The hypothesis of changing the legislation to a system of presumed consent in order to address the organ shortage is explored. The main issues surrounding a change in the legislation are considered, and the effects on society and the individual are discussed. This paper argues that there is not enough convincing evidence to support a change in the legislation to a system of presumed consent at this time. Instead, an increase in organ donations could be achieved by improving the effectiveness of the current system of organ donation, and by improving the public's awareness and understanding of organ transplantation issues.
Introduction
Organ transplantation significantly improves the health, quality of life and life-expectancy of people whose organs have failed. It offers substantial and rapid benefits for patients in liver, heart or lung failure, where the only alternative to a transplant is early death. Renal transplantation, which is the most common organ transplantation performed, has established itself as the optimum treatment for end-stage renal failure in terms of results, rehabilitation and costs. 1
Unfortunately, it has not been possible to fulfil the full potential of advances in transplantation surgery because of a severe shortage of available donor organs. Many of the patients who potentially could benefit from receiving an organ transplant cannot be treated in that way. 2 Patients may wait for an organ transplant for years, while undergoing difficult and stressful treatment. Many patients die before a suitable organ becomes available for transplant.
The severe shortage of human organs for transplantation has prompted numerous proposals to alleviate this problem, including: educational campaigns, ‘presumed-consent’ legislation, a ‘required request’ policy, compensation or payment of organ donors, organ exchange mechanisms for living donors with incompatible recipients, preferential assignment of organs to registered donors, the use of organs from living unrelated donors, use of marginal donors, xenotransplantation (transplantation of organs from a different species) and the use of pluripotent stem cells. 1,3–5
This article attempts to demonstrate the magnitude of the problem of organ shortage and identify possible causes. The current UK legislation is described and compared with the legislation in other jurisdictions. The main issues surrounding a change in the current legislation to a system of presumed consent to organ donation are also explored.
Sources of transplant organs
Organs for transplantation can be acquired via three routes:
Live donation: Live donation is the donation of an organ from one living person to another. Under the Human Tissue Act 2004,
6
all living donors have to be assessed to ensure that they understand the risks which donation involves and that their consent has been given freely and voluntarily;
Donation after brainstem death: Donation after the diagnosis of brainstem death (DBD) is the main source of donor organs. Most of the donors are patients who have suffered irreversible brain injury resulting in brainstem death and are being cared for in intensive care units (ICUs), where they are being ventilated. It must be established that the patient has suffered an event of known cause resulting in irreversible brain damage with apnoeic coma. During apnoeic coma the patient has no spontaneous respiratory movement and is mechanically ventilated; Reversible causes of coma must be excluded; A set of bedside clinical tests of brainstem function are undertaken to confirm the DBD.
7
(3) Donation after cardiac death (DCD): DCD, or non-heartbeating (NHB) organ donation, takes place from donors who have suffered a cardiorespiratory arrest, i.e. there is no heartbeat and breathing has stopped.
Guidelines for DBD are well established and clearly set out. According to the Intensive Care Society, brainstem death is diagnosed in three stages:
Despite these guidelines, there are scientists who disagree with this way of defining and confirming death because they believe it is not accurate. They prefer the traditional process for certifying death by establishing that there is no heartbeat and that breathing has stopped.
DCD commonly occurs after the planned withdrawal of life-sustaining treatments for patients in ICUs when there is no hope of recovery and it is in the best interests of the patient to withdraw any further active treatment.
7
Sometimes DCD may take place after an emergency admission of a patient who suffered sudden cardiorespiratory arrest, e.g. following a heart attack or a car crash, in which case organ retrieval should be done quickly because there is no blood supply to the organs.
Organ transplant demand and supply
The principal problem in organ transplantation is the discrepancy between supply and demand. In the UK three people die every day while they wait for an organ. 8 In 2008–2009, 448 patients died in the UK while waiting for their transplant. 9
The number of patients registered for a transplant continues to increase. On 31 March 2009 there were 7877 patients on the active list waiting for an organ transplant, and a further 2385 patients were on the temporarily suspended transplant list. This represents an increase of 3% and 14%, respectively, on the corresponding figures at the end of the previous year. 9 At the same time, the UK has one of the lowest organ donor rates in Europe at 14.9 per million population (pmp). 9
Figure 1 shows the numbers of patients on the active transplant lists, the numbers of deceased donors and the organ transplants received from deceased donors for 1 April 1999 to 31 March 2009. 9 It shows that the number of organs available for transplantation has remained largely static for the last 10 years in the face of increasing demand, and the gap between the number of people waiting for a transplant and the number of organs that become available is increasing.
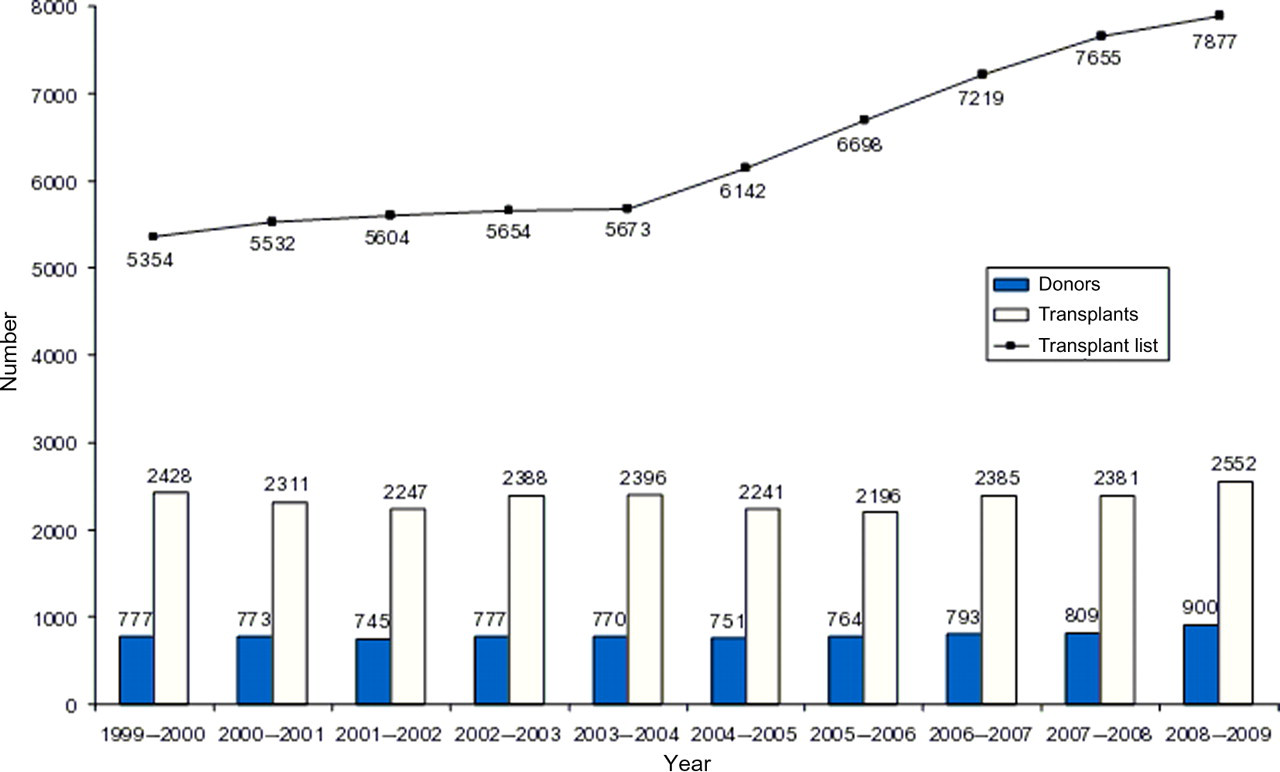
Numbers of patients on the active transplant lists on 31 March of each year, numbers of deceased donors and organ transplants received from deceased donors, 1 April 1999–31 March 2009. Source: NHSBT, Transplant Activity in the UK 2008–2009 9
In the UK, between 1 April 2008 and 31 March 2009, 3513 patients had their lives saved or improved by an organ transplant. Of these, 2552 organs were received from deceased donors, and 961 were received from living donors. In addition, 2711 patients had their sight restored through a cornea transplant. There were 900 deceased donors of solid organs and 2075 donors of ocular tissue. Nearly all deceased donors (95%) gave a kidney and of these the majority (78%) also donated at least one other organ. 9
It is difficult to define the true need for organs for transplantation because the number of people who are on the waiting list for an organ transplant does not reflect the true extent of the number of people who would benefit from a transplant. The true need is, at minimum, 50% more than the people who are on the waiting list. Of the 1000 or so people who die each year for lack of an organ transplant, only about 500 are on the waiting list. 10
Patients are not put on the transplant waiting lists because clinicians know there is no hope of them getting treatment and are cautious about raising the expectations of patients who have little chance of being met. Most transplant units limit the number of people who are put on the waiting list to an approximation of the likely number of organs that are going to be available.
Based upon experience of the last few years there is nothing to suggest that demand for organs will do anything but increase at a linear rate. 11,12 Figure 2 shows the projected demand for organ transplants over the next 10 years.

Projected demand for organ transplants over the next 10 years. Source: ODTF, Organs for Transplants – The Supplement Report 12
The list of patients waiting for an organ transplant is rising rapidly with changing demographics in the UK. The population ages and develops more chronic diseases which precipitate the failure of organs. In addition, there is a surge in diseases related to organ failure, for example type 2 diabetes that can cause kidney failure and lead to the need for a kidney transplant.
Despite an increase in recent years in the number of both living and NHB donors, the number of deceased heartbeating (HB) donors, which is the main source of donor organs, has changed little over the last few years. 9 Figure 3 shows the number of HB, NHB and living donors in the UK between 1 April 1999 and 31 March 2009.

Number of heartbeating, non-heartbeating and living donors in the UK, 1 April 1999–31 March 2009. Source: NHSBT, Transplant Activity in the UK 2008–2009 9
It is thought that the decrease in DBD in the UK is partly due to a decline in the number of fatal road traffic accidents and due to a decline in deaths following cerebrovascular accidents where early management has become more precise and ventilation less frequent due to improving imaging technology. 1,2,4
Furthermore, the number of intensive care beds in the UK is inadequate in comparison with other western European health services, resulting in many potential donors not being ventilated. 2
Several other factors have been hypothesized to influence cadaveric organ donation rates in the medical literature, including: legislation, level of wealth, religious beliefs, social norms, education, medical and transplant infrastructure and overall health expenditure. 4,13,14
During 2008/09, there was a 7% increase in the number of people joining the Organ Donor Register (ODR), rising from 15.14 million to 16.12 million by the end of March 2009. 8 The majority of new registrants came from driving licence applications and reminders through the DVLA, general practitioner registration and through applications for a Boots Advantage Card. 9 Of the 900 deceased organ donors in 2008–2009, 37% were registered on the ODR. 9
Black and minority ethnic people
The gap between supply and demand of organs for transplantation is particularly large among people of black and minority ethnic (BME) origin. People of BME origin are significantly under-represented on the ODR and yet are disproportionately more likely to require a transplant.
People of BME origin are three to four times more likely than Caucasians to develop renal failure and need a kidney transplant, due to a higher incidence of type 2 diabetes. Furthermore, one in nearly 10 of all cornea transplants are performed on South Asians because they develop keratoconus at a younger age (under 30) than white people, and South Asian people are more likely to need a liver transplant due to their higher prevalence of viral hepatitis (hepatitis B and C). 12
Although one in five people waiting for a transplant are from BME background, in 2008–2009 only 4.7% of deceased organ donors came from BME communities, 9 who in the 2001 census made up 8% of the UK population. 12 Just 1% of people registered on the ODR are South Asian and 0.3% of people registered are African-Caribbean. 12 This is a particular problem because for a transplant to be successful the donor should come from the same ethnic group as the recipient so that there is a better chance of a close match of tissue type and blood group between the donor organ and the recipient.
People of BME origin have to wait on average twice as long as a white person for a kidney transplant. White patients wait on average 722 days, Asian patients wait 1496 days and Black patients wait 1389 days. 12 One in eight patients who died waiting for a transplant in 2006 were of African-Caribbean or South Asian origin. 12
Importantly, the BME populations in the UK tend to be younger compared with the white population. Since the prevalence of renal failure increases with age, this will result in a greater need for kidney transplants in the future. Furthermore, the BME population is expected to increase, and within the group there is a greater demand for organ transplantation and a lower propensity to donate organs.
National Potential Donor Audit
NHS Blood and Transplant (NHSBT) have established the Potential Donor Audit which collects information on every single patient in the UK who dies in the ICU. Through the audit, at each possible stage of the process, they try to identify the possible causes for missed opportunities for organ donation. Table 1 shows the summary key percentages resulting from the audit. Potential HB donors are patients for whom death was diagnosed following brainstem tests, and potential NHB donors are defined as patients suitable for NHB donation whose treatment was withdrawn.
Key percentages resulting from the national Potential Donor Audit, 1 January 2007 to 31 December 2008
HB, heartbeating donors; NHB, non-heartbeating donors
Source: NHSBT, Transplant Activity in the UK 2008–2009 9
The Potential Donor Audit showed the following causes as being the most important for missed opportunities for organ donation (see Table 1):
Family refused: The consent rate is the percentage of potential donors whose families gave consent for organ transplant. The overall HB consent rate was 62% (refusal rate 38%), and the overall NHB consent rate was 58% (refusal rate 42%). Family refusal is shown to be an important reason why HB and NHB patients do not go on to donate their organs;
Patient not referred: The referral rate is the percentage of potential donors referred to a coordinator. There were cases where donation appeared not to have been considered at all, or if considered, they were not referred to the donor coordinators every time;
Family not approached: The approach rate is the percentage of potential donors whose family were approached for consent to donation. In some cases the donation was considered, but the family was not approached. Prior knowledge that a family would reject a request to consider donation influenced whether a formal approach was made, and suggests that the actual family refusal rate in the UK is somewhat higher than the quoted figure;
Consent obtained but donation did not occur: Conversion rate is the percentage of potential donors who became actual donors. These are cases where consent was obtained but donation did not to occur for various reasons, e.g. medical unsuitability.
The Potential Donor Audit showed that between 1 January 2006 and 31 December 2007 there was no significant difference in the refusal rate between male and female potential donors or across the age groups. There was a clear difference in the refusal rate between white and non-white patients. The families and friends of African-Caribbean and South-Asian potential donors were more likely to withhold consent for donation to take place than for white donors. The refusal rate for non-white potential donors was 69%, compared with 35% for white potential donors.
10
The current legislation
In England, Wales and Northern Ireland, consent to organ transplantation is governed by the Human Tissue Act 2004, 6 which covers both living and postmortem donation. The 2004 Act was forced into service as a result of the widespread unauthorized retention of tissues following postmortem examination, and the Alder Hey and Bristol scandals where after children had died their organs were retained without the consent or even the knowledge of the family.
The 2004 Act makes consent the fundamental principle underpinning the lawful removal, storage and use of body parts, from the living or the deceased. The 2004 Act states that no organs and tissue for transplantation can be taken without appropriate consent of the deceased or their relatives. 6
The current system for consenting to donate organs is referred to as ‘explicit consent’ or ‘opting-in’. Appropriate consent to donate organs is considered to have come from a deceased person if the person had given explicit consent, by joining the ODR, or by carrying a signed donor card, or by making any other form of advance statement that would be recognized under the terms of the Mental Capacity Act 2005.
If an individual has given prior consent to donation, there is no legal right of veto by the relatives and they cannot over-rule the deceased's wishes. The Act makes it explicit that it is the wishes of the deceased individual that should prevail and not the family's. Nevertheless, the legislation is permissive and does not enforce donation to proceed. In exceptional cases where relatives have strong and sustained objections, doctors do not have to proceed with donation against the strongly expressed views of the relatives, despite consent having been obtained from the deceased.
If no prior consent has been given by the deceased, consent may be given or withheld by a nominated representative of the deceased or a person who stood in a qualifying relationship to the deceased. The ranking of qualifying relationships is set out in a strict order of priority in the Human Tissue Authority Code of Practice (highest first):
Spouse or partner (including civil or same sex partner); Parent or child (in this context a ‘child’ can be any age); Brother or sister; Grandparent or grandchild; Niece or nephew; Stepfather or stepmother; Half-brother or half-sister; and Friend of longstanding.
15
The consent of a Gillick-competent child to organ donation after death is valid and should prevail over parental objections. In the absence of consent, or if a child lacks competence to make a decision, authority to consent passes to the person who has parental responsibility, or, failing that, to a person who stood in a qualifying relationship to the child.
A system of presumed consent
Under a system of ‘presumed consent’ or ‘opting-out’, all citizens are presumed to be willing to donate organs after death and are deemed to have given consent to organ donation unless they have specifically ‘opted-out’ by registering their objection to organ donation while alive. Everybody will automatically be viewed as a potential donor unless they had ‘opted-out’ before death. 16
There are two main types of presumed-consent system: ‘hard’ or ‘soft’. Under a ‘hard opt-out’ system, relatives do not have any right of veto and their views are not taken into account. Under a ‘soft opt-out’ system, although the deceased's consent to organ donation is presumed, the relatives' views are taken into account and if the relatives show strong objection to organ donation then organ retrieval cannot take place.
Other jurisdictions
The UK, North America, Australasia and most of Asia have explicit consent systems. Many European countries have a form of presumed-consent system. In general (although there are exceptions), the mainly Catholic countries of Central and Southern Europe which have a legal system based on Roman law and an emphasis on the citizen's duties to the state have presumed-consent systems, whereas the largely protestant countries of Northern Europe which rely more on common law, and place more emphasis on individual rights of determination, have informed-consent systems. 1
Spain and Belgium have soft presumed-consent systems. In both countries, health-care staff can proceed with organ donation unless the deceased has registered to opt-out or the deceased's relatives oppose organ donation. The difference between Belgium and Spain is that in Belgium it is up to the relatives to tell the doctors not to proceed with organ retrieval if they oppose organ donation because the doctors may not ask them, whereas in Spain it is considered good practice for doctors to ask the relatives for their agreement to organ donation at the time of death. 13,14
Austria has a hard presumed-consent system. Also, Singapore has a hard presumed-consent system, which does not cover Muslims, because Muslims chose to opt-out as a group. Therefore, in Singapore, doctors can remove organs from every adult who dies unless the deceased has registered to opt-out or the deceased is Muslim. 13,14
In the Netherlands, under the Organ Donation Act 1998, everyone over the age of 18 is encouraged to register one of four options regarding postmortem donation: a consent to donate any or specified organs, a refusal to donate, delegation of consent to the next of kin or delegation to a nominated person. 17
Family involvement in organ donation
The request for organ donation arises out of situations of very sudden, unexpected and untimely deaths. Although organ donation is usually regarded positively, when families are confronted with the sudden death of a close relative they are in great emotional distress and the decision about organ donation can be extremely traumatic to them.
Supporters of presumed consent argue that under an informed-consent law, the burden of responsibility for the decision is put on the family, whereas under a system of presumed consent the primary responsibility is on the doctors looking after the deceased. In a system of presumed consent, the relatives of a deceased who has not expressed a wish to donate may be relieved of the burden of making that decision at such a traumatic time. 18 By not registering his or her wish, the deceased person has accepted implicitly the possibility of becoming a donor, thus making it easier for the family not to oppose donation and freeing them of any responsibility or remorse. 19
Furthermore, presumed-consent legislation may play an important role in shaping the decision of the families and it has been argued that legislative defaults on organ donation may affect the consent decisions of potential donors and families, even if they are not enforced. 4 In the USA and UK, which are informed-consent countries, approximately 40–50% of relatives who are approached to consent to donation refuse it, compared with around 20% in Spain and around 30% in France which are presumed-consent countries. 4
On the other hand, a system of presumed consent may result in undue pressure being placed on families, by ignoring their wishes and proceeding to organ donation without their consent. To proceed with organ donation against the strongly expressed views of the relatives would be inappropriate, counterproductive and could harm the transplant programme. Furthermore, it would damage the vital relationship of trust between clinicians caring for people at the end of life, their patients and their families.
In practice, regardless of the type of legislation and of whether a deceased individual is registered as a donor, in most countries families are allowed to have the last word on whether organs will be donated. Donor families often find great comfort in being an active part of the decision to donate. Before donation would go ahead, the support of the relatives for organ donation is needed in order to ensure the quality and safety of donated organs. Through a detailed discussion with the donor's relatives, it is necessary to obtain a full medical history of the donor, social and sexual history, and discuss the possible previous use of intravenous recreational drugs. The relatives of potential organ donors must always be involved in the donation process and should be approached by transplant coordinators who have all the necessary training and skills. Securing the relatives' support is a key part of the donation process.
A positive experience of organ donation by the relatives has the added advantage of increasing donation rates through the educational role they play within their own communities and the formal roles they sometimes adopt to help educate health-care professionals and bereavement support groups. 7 Relatives receive some comfort and become motivated by what their deceased family member achieved through donation, and a heroic status is often attributed to the organ donors.
A system of decision-making which is based on respecting the known wishes of the patient and the wishes of the family is required in order to maintain the integrity of the relationship between doctors and the public, and maintain trust and confidence in the donation system. Over-riding relatives' wishes or cutting them out of the decision for organ donation completely, as happens under a presumed-consent system, would probably be unacceptable by society.
A soft presumed-consent system may be more acceptable by the public and physicians, where the relatives of a deceased potential donor would be consulted, and donation would not go ahead if it became evident that to do so would cause severe distress to the relatives.
Nevertheless, some groups do not agree with a soft opt-out system because they believe that already with the present system the relatives are asked if they are aware of any objections by the deceased to organ donation, rather than a positive wish to donate organs. As a result, a soft opt-out system has nothing more to offer compared with the current system, and the public debate needed to achieve it could backfire with reduced donations.
Measures to increase organ donation
No transplantation law can operate efficiently without acceptance by the public. The public remembers the emotional tension caused by the scandals surrounding organ retention which led to the change in legislation and the current Human Tissue Act 2004. 6 Imposing a presumed-consent law without first building sufficient social support could generate an adverse response to organ procurement efforts.
Before resorting to controversial changes in legislation to address the problem of organ shortage, the Government should identify the causes for the low donation rate in the UK and take appropriate measures to target them. According to surveys, there is a very high degree of public support for donation, with 90% of the UK population in favour of organ donation in principle, but in practice only 26% of the population has joined the ODR. 9 Furthermore, the actual donation rate remains poor, and in part this is a consequence of the 40% of relatives who refuse to give consent to organ donation.
One important cause for the low donation rate could be ignorance of the transplantation issues. Also, people may not be aware of how to register their wishes to become organ donors after death, or they just never get around to registering. Furthermore, giving consent to donate organs after death dictates a conscious effort that many healthy or young persons may find difficult to make. In a survey performed by the Organ Donation Taskforce (ODTF), a number of barriers to donation were identified, including lack of awareness, laziness, unwillingness to think about death and concerns about donation in practice. 13,14
The gap between the numbers of people registered on the ODR and those who say they support donation exposes the inadequacies of the current system of registration of preference. The ODTF identified the following inadequacies: lack of awareness about the ODR, a low budget for promotion of the ODR, confusion among individuals as to whether they have actually registered or not, the incorrect assumption that having a donor card is the same as being on the register and inadequate control over data input. 13,14 There is a need to publicize the register and to make the process of registering easier and more widely understood.
An online survey commissioned by NHSBT to measure public attitudes towards the ODR and barriers to joining it showed that the most common reasons for not joining the ODR were concerns about the level of respect given to a deceased person's body and whether doctors make every effort to help a patient if they are identified as a potential organ donor. 8
One possible reason for relatives refusing to give consent to organ donation may be that they are not fully aware of the wishes of the deceased. According to the Potential Donor Audit report, if the deceased was registered on the ODR, 90% of families consent to donation, compared with a general consent rate of 61%.
Moreover, the relatives may not be aware of the deceased's wishes because most people are reluctant to talk about death even with those closest to them. If uncertain the relatives may feel that the ‘safest’ decision would be to refuse consent to organ donation. People should be encouraged to discuss the issue of organ donation with their families and friends, and ensure that their relatives are aware of their wishes about organ donation.
Another reason for the relatives' refusal may be that in general within society there exists a culture of distaste to having the body interfered with after death and relatives may fear that retrieval of organs would mean the ‘mutilation’ of the deceased. More public education is required on organ retrieval procedures in order to dispel any fears people may have based on misconceptions about organ donation.
It is important to identify the reasons for non-donation, and encourage consent to organ donation from all sections of society, particularly from the BME population. Instead of changing the legislation, maybe much more effort should be put into identifying the most effective ways to promote public awareness, public understanding and acceptance of organ donation.
It is clear that better public education about organ donation and transplantation is essential. Public awareness should be raised by improving the knowledge of both health professionals and the media. The Government should fund a campaign with big media coverage to increase public awareness and understanding of organ donation and transplantation. Education on organ donation could also be introduced in schools, perhaps as part of personal and social education issues. Such efforts to raise awareness should be accompanied by research and auditing to assess their effectiveness in increasing donation rates within the current opt-in system.
The ODTF performed an analysis of the likely costs of setting up the necessary infrastructure and communications strategies required to implement a presumed-consent system. Communications are the costs required to educate the public of the new legislation and inform them how they can opt-out if they wish to. The costs were calculated to be around £45 million in set-up costs for IT and communications, then £2 million per year in IT running costs and £5 million every few years to refresh public messages. The Taskforce concluded that the resources would be better prioritized if they were directed towards raising public awareness and understanding about organ donation. 13,14
BME groups
It is not clear how acceptable a system of presumed consent would be by people of BME origin. However, it has been suggested that BME groups may not agree with a system of presumed consent and its enforcement could backfire and reduce donations by BME groups.
There is a need to develop a more detailed understanding of the barriers to donation within BME communities and find the most effective ways to overcome them in order to promote organ donation from BME groups within the current legal framework.
Education level and social status are important factors affecting organ donation, because they influence the amount of information people are exposed to and their ability to understand that information. Moreover, organ donation decisions within BME groups may be influenced by cultural barriers and their broader experiences of, and attitudes to, the health service system more generally. 7
It is important to consider whether issues of alienation and inequality might have an impact on a willingness to donate among BME communities. People from BME groups often feel that the process of organ donation is not something in which everybody is dealt with equally, and that they are treated unfairly. 7
There is an urgent need to address the number of BME patients requiring organ transplants otherwise the human and economic costs will be severe. In the short term, there needs to be a greater number of donors coming forward from these communities to increase the supply of organs. Before changing the legislation, the Government should consider other measures to increase organ supply which may be more acceptable by BME communities. The Government should organize locally led educational programmes, tailored to the attitudes and beliefs of BME groups, and engage actively with BME communities, in order to promote awareness on transplant-related issues and increase the level of organ donation from those communities.
In the long term, there needs to be greater attention on preventive strategies to reduce the number of patients from BME origin requiring organ transplants due to organ failure. The Government should address the problem of poor access to services for BME groups and resources should be directed to improving the quality of preventive care in primary care settings and to public health interventions. Patients of BME origin should be educated on lifestyle changes to prevent diseases leading to organ failure, and screening programmes should be established in the community to diagnose and treat these diseases at an early stage before they cause organ failure.
Religious groups
The decision for organ donation by potential donors or their relatives may be affected by their religious beliefs and the perceptions of the views of the faith group to which they belong. Most faith groups within the UK support organ donation in principle and the six major faiths – Christianity, Judaism, Islam, Hinduism, Buddhism and Sikhism – have all explicitly endorsed organ donation.
Faith groups express a range of views to the idea of changing the legislation to a system of presumed consent to organ donation. While some faith groups would be content with a system of presumed consent, most religious groups have significant doubts and concerns about the concept and others express outright opposition. 7 According to the ODTF, the majority of the religious groups oppose the introduction of an opt-out system. 13,14 Some faith leaders warned of the potential for provoking antidonation feelings and even active antidonation campaigning. 13,14
A variety of views may exist within the scope of a single faith. Also, an individual may decide on the basis of a personal interpretation of the religion and at odds with the official orthodoxy. The views of most faith groups differ about the degree to which a decision regarding donation is to be seen as a matter of religious doctrine or one of individual conscience. Furthermore, it is not clear whether a decision for organ donation is based solely on faith, or culture, or ethnicity, or a combination of these.
Under a system of presumed consent it may be possible for people to opt-out or be opted out as a group. For example in Singapore, where they have a presumed-consent system, Muslims opted out as a group. Nevertheless, this may not be advisable in the UK because of the societal divisions this may create and the general belief that opting out should be a matter of individual choice.
The Government should encourage the development of programmes which work at a local level with faith and community groups to clarify and communicate issues relating to organ donation. Local faith leaders have an important part to play using their considerable influence in order to promote support for organ donation in their communities, particularly given that opinion at grassroots does not always reflect the official view of the faith. Furthermore, faith groups should be invited to advise on the development of national and local policies relating to organ donation and transplant in order to help ensure that these are sensitive to the needs and concerns of members of such groups.
Autonomy
It has been argued that cadaver organs should be seen as a community asset and that it is immoral to allow them to go to waste. Emson 20 justifies the latter view by seeing the human body – as opposed to the human spirit – as being ‘on extended loan from the biomass to the individual of which it forms a part’. On the same note, Truog 21 argues that, while alive, people's organs should be considered their personal property, but after death their organs should be considered a societal resource. In Harris' view, organ donation is no more than an example of a ‘small but significant class of public goods, participation in which [should be] mandatory’. 22
Some groups support the routine recovery of cadaveric organs for transplantation without the need for consent, because they believe that the requirement for consent, whether explicit or presumed, is responsible for patients' deaths. In their opinion, ‘non-consent leads to non-procurement of potentially life-saving organs, and non-procurement limits the number of people who could have been saved through transplantation; therefore, non-consent results in loss of life’. 18 Emson 20 argues that it is immoral to require consent for cadaveric organ procurement because this practice leads to an unnecessary loss of life.
One of the major reasons for insisting on explicit consent is to show respect for autonomy which is central to modern medical ethics and law. However, Beauchamp and Childress 23 pointed out that although autonomy is important, it ‘has only prima facie standing and can be over-ridden by competing moral considerations’. It is thought that the obligation to respect someone's autonomy is not absolute, and that it ceases to exist when the cost is unnecessary loss of human life, which is what happens when permission for organ recovery is denied.
Individual autonomy is a major principle of biomedical ethics, and proper consent in the context of organ donation is of great importance. Any process by which people register their willingness to donate must be judged in terms of whether that process allows individuals to make a valid and ethically defensible statement of consent. Any move away from a system relying on expressed consent must be shown to be a justifiable exception to the current ethical norms.
Not respecting the autonomy and the wishes of the deceased may result in disrespect for religious or other moral convictions of the deceased or his/her relatives, and offend or harm the relatives of the deceased. In addition, not respecting the deceased's autonomy and the wishes of the family in order to increase organ donations will result in public upset and outrage which will backfire and damage the organ transplant programme.
The end result does not justify the means, and it is important not to lose the values we have built as a society. Autonomy is important and should always be central in patient care. People should have the right during their lifetime to set out their wishes about what should happen to their bodies after death, in the expectation that those wishes will be respected. In addition, in attempting to increase the supply of organs for donation, it is important not to lose sight of the needs and concerns of the family of the deceased. As already discussed, securing the support of the donors' relatives forms a key part of the donation process.
A system of presumed consent is thought to undermine the principle of informed and freely given consent. Presumed consent is seen by some as ‘no consent at all’, and it is believed to be unethical to presume someone's consent to such an emotive procedure. It is argued that explicit consent, obtained either by the person registering on the ODR or by signing a donor card, could provide the best unambiguous evidence that a person wanted and had decided to donate.
Moreover, it is thought that presumed consent would turn us from volunteers into conscripts and presuming consent would turn donation into an action by default, rather than something freely gifted. Many transplant recipients have argued that a donated organ is more easily accepted because they know it has been freely given by the donors and their families.
It has been reported in surveys that 90% of the UK population are in favour of organ donation, yet only 26% have registered their wishes on the ODR. 8 An important reason for this gap is inertia, i.e. people not getting around to registering their wishes on the ODR. It has been argued that having a presumed-consent system would more accurately reflect the wishes of the majority, allowing donation to become the default position.
On the other hand, there is the concern that people would not get around to registering their objection to donation under a presumed-consent system, and could mistakenly be considered as willing donors. In addition, if an individual does not register an objection, it is possible that their silence may indicate a lack of understanding rather than agreement with the policy. It is because of these concerns that in the majority of countries operating a presumed-consent system, doctors still consult the family to establish consent.
Does presumed consent increase organ supply?
Abadie and Gay 4 of Harvard and Chicago Universities studied 22 countries during the period 1993–2002 to analyse the impact of presumed-consent laws on donation rates. They obtained information on a number of factors that are thought to affect donation rates and legislative defaults on organ donation, such as per capita gross domestic product, health expenditures per capita, religious beliefs, the legislative system and the number of deaths caused by motor vehicle accidents and cerebrovascular diseases. They used regression analysis to study how presumed-consent legislation is related to cadaveric organ donation rates, after controlling for other determinants of organ donation. They demonstrated that while differences in other determinants of organ donation explain much of the variation in donation rates, after controlling for those determinants presumed-consent legislation had a positive and sizeable effect on organ donation rates. They showed that, once other determinants of organ donation are accounted for, presumed-consent countries have roughly 25–30% higher cadaveric donation rates, on average, than informed-consent countries.
A review paper by Rithalia et al. 24 analysed the results of five studies comparing donation rates before and after the introduction of legislation for presumed consent (‘before and after studies’). All five studies reported an increase in donation rates after the introduction of presumed consent, but there was limited exploration of other changes such as increased publicity and organizational and infrastructure changes that might have taken place at the same time as the change in legislation. As such factors can potentially influence donation rates, it was unclear to what extent the increases found were directly attributable to the change in legislation.
The review also analysed eight studies comparing donation rates in countries with and without presumed-consent systems (‘between-country comparisons’). All eight studies were based on secondary analyses of published data, therefore any relation found between presumed consent and organ donation rate was associative and could not show whether the effect was directly attributable to the intervention. In the four best-quality ‘between-country comparisons’, presumed-consent law or practice was associated with increased organ donation (increases of 25–30%, 21–26%, 2.7 more donors pmp and 6.14 more donors pmp in the four studies). Other factors found to be important were mortality from road traffic accidents and cerebrovascular causes, transplant capacity, gross domestic product per capita, health expenditure per capita, religion (Catholicism), education, public access to information and a common law legal system. 24
The reviewers concluded that it is difficult to assess the exact contribution of presumed-consent legislation alone, and that presumed-consent alone is unlikely to explain the variation in organ donation rates between countries. They also concluded that legislation, availability of donors, organization and infrastructure of the transplantation service, wealth and investment in health care and public attitudes to and awareness of organ donation may all play a part, but their relative importance is unclear. 24
Transplant services organization
Spain now has the highest organ donation rate in the world. But 15 years ago, before the Spanish began systematically to address barriers to organ donation, they had a rate similar to that of the UK today. Although Spain has an opt-out system, in practice their system is very similar to an opt-in system. Organs are not taken against the wishes of the deceased's family. The relatives are always approached to ascertain the wishes of the deceased about organ donation, or if the wishes of the deceased are unknown, the relatives are approached to give their permission to proceed with organ donation.
Furthermore, although Spain has had an opt-out system since 1979, the figures for donation started to improve only 10 years after the introduction of the Spanish National Transplant Organisation (ONT) in 1989 which resulted in an increase in the organ donation rate from 14.0 to 35.1 pmp. Dr Rafael Matesanz, the director of the national transplant organization in Spain, acknowledged that the increase in organ donation during the 1990s could not be attributed to a change in legislation, but to changes in the organization of transplantation services to address barriers to organ donation. 3
The Spanish success is the result of an integrated and systematic approach to organ donation. Donation activity is coordinated at national, regional and local levels.
3
The key elements of the Spanish model can be summarized as follows:
A well-structured national transplant coordination network exists and there is a competent authority which supports the whole system; In every hospital with critical care facilities there is a transplant coordinator who belongs to the staff of the hospital and is responsible for the organ donation in that hospital; Transplant coordinators are qualified physicians who are trained to detect potential organ donors at an early stage, approach his/her family, monitor the medical progress through to a diagnosis of brain death, and follow up the necessary procedures to organ donation; It is recognized that organ donation can be stressful and transplant coordinators are changed regularly before they ‘burn-out’; The burden of organ procurement is taken away from transplant surgeons and treating physicians; The organ retrieval teams are fully resourced and efficient; All hospitals with critical care facilities are committed to ensure that all potential organ donors are identified and notified to the donor coordinator network. Donation is seen as an integral part of end-of-life care for all suitable patients; Hospitals are compensated for the effort and resources they put into organ donation. Reimbursements are provided to incentivise hospitals to consider organ donation more as an incentive rather than as a burden, in order to promote organ donation; Each step of the donation process, and the performance of individual hospitals, are continuously monitored and audited; There is strong political leadership and high-level political commitment; The public supports organ donation and trusts the system in place; The support of the public has been partly built by establishing a permanent contact with the media and by improving the media skills of the health professionals who are part of the system; Organ donation features as a main part of doctors' training.
2,3,7
Italy is another example where organ donation rates increased after organizational measures were implemented. Italy changed their legislation in 1999, introducing both presumed consent and an organization similar to the Spanish ONT, with national, regional and local coordinators.
16
Although the presumed-consent system applied throughout Italy, not all regions implemented the organizational changes. Only those regions that have implemented changes in the infrastructure and organization of their organ transplantation services showed a sustained increase in organ donation rates. In Tuscany, one of the regions that implemented changes in the organization of their organ transplantation services, the rate of deceased organ donations doubled in just one year to a rate of 26.9 pmp.
25
Tuscany saw an overall increase from a rate of 10 donors pmp in 1997 to over 40 pmp in 2006.
16
The ODTF drew considerably on the Spanish experience in formulating their recommendations to the Government in order to increase organ donation and procurement within the current legal framework. With the implementation of their recommendations, the Taskforce estimated a 50% increase in organ donation over five years, which would enable an additional 1200 transplants a year, resulting in thousand of lives being saved and significant cost-savings. 11,12
Furthermore, the ODTF recommended that an opt-out system should not be introduced in the UK at the present time, and that an opt-out system should be reviewed again in five years' time in the light of success achieved in increasing donor numbers through implementation of their recommendations. 13,14
Between 1 April 2008 and 31 March 2009, compared with the previous 12 months, there was an 11% increase in the number of deceased organ donors, a 12% increase in the number of living organ donors, a 9% increase in both the number of solid organ transplants and the number of cornea transplants carried out across the UK and a 7% increase in the number of people joining the ODR. 9 These increases are probably related to the implementation of the recommendations of the ODTF and the organizational and infrastructure changes that have taken place. Also, they may be related to the increased publicity created by the public debate on whether to change the legislation to a system of presumed consent.
The Legal Working Group advice
The Legal Working Group of the ODTF advised that a presumed-consent system needs to provide for the right of individuals to opt-out in order to be compliant with the European Convention on Human Rights (ECHR). Otherwise, if it is it too administratively difficult for people to opt-out there would be breaches of articles 8 (right to respect for private and family life) and 9 (right to freedom of thought, conscience and religion) of the ECHR. 14
The Legal Working Group suggested that before changing the legislation to a system of presumed consent there must be considerable widespread public consultation, public awareness should be raised and sufficient time should be allowed after the introduction of the new legislation to enable people to adjust to it. 14
The Legal Working Group advised that it is necessary to seek evidence from the family about the deceased's wishes and beliefs, whether the system stays as opt-in or changes to opt-out, because the evidence from the register regarding the deceased's wishes is insufficient to ensure compliance with the ECHR. This is because under an opt-in system, people who registered their wish to donate organs a long time ago may have since changed their minds, but never got around to removing their name from the register. Under a system of presumed consent there is the concern that organ retrieval may take place from people who did not register their objection to organ donation for various reasons: they never got around to registering their objection due to being lazy or disorganized, or they have learning difficulties, or English is not their first language. 14 Therefore, whatever the consenting system is, doctors must always consult the family before progressing with organ donation in order to avoid the risk of a successful legal challenge under the ECHR.
The Legal Working Group advised that a hard opt-out system which did not seek evidence from the deceased's family about the potential donor's wishes regarding organ donation could be open to a successful legal challenge under ECHR, because the evidence from the register regarding the deceased's wishes would be insufficient. 14
The Legal Working Group concluded that it would be legally possible to introduce a soft presumed-consent law where the family of the deceased would be involved in providing evidence of the deceased's wishes and beliefs after their death. It was agreed that such a system would be compatible with the ECHR if it allowed adequate provisions for a person to opt-out or change their registered decision. 14
Conclusions
The principal problem in organ transplantation is the discrepancy between supply and demand, resulting in a significant loss of life and suffering. Changing the legislation is an attempt to address the problem of organ shortage. A change in the legislation will have significant effects on the individual, on society and on patients waiting for a transplant.
A change in the legislation to a system of presumed consent may result in an increase in organ donations, but there is no convincing evidence to suggest that the increase in organ transplants, as a result of a change to a system of presumed consent, would be significant enough to counterbalance the public upset and debate that would result from such a system. Furthermore, it may not generate additional donors in sufficient numbers to justify the significant investment needed to put a presumed-consent system in place.
One of the major reasons for insisting on explicit consent is to show respect for autonomy which is central to modern medical ethics and law. Also, explicit consent ensures the support of the deceased's family which forms a key part of the donation process.
It is unlikely that an event as complex as donation will be uniquely influenced by a single action such as a change in legislation. An increase in organ donation cannot be achieved by ‘changing one single aspect of the organ donation system in isolation, but rather by addressing each piece in the complex jigsaw of interdependent elements that make up a successful donation programme’. 13,14
Based on the current evidence, a convincing case has not yet been made for an immediate move to a presumed-consent system, and it may be premature to adopt a system of presumed consent before attempting to improve the effectiveness of the current system.
There are multiple measures that could be adopted by the Government aiming to improve the public's attitude towards organ transplantation in order to increase organ donations. Through national and targeted campaigns, the Government should enhance the operation of the existing system of donor registration by raising public awareness and understanding of organ transplantation issues.
Furthermore, the Government's top priority, in seeking to increase the supply of organs, should be to implement the re-organization and improvement of organ donation and transplantation services. This type of approach should be considered initially before resorting to controversial changes in legislation to address the problem of organ shortage.
None declared.