
Abstract
We report an unusual death of a seemingly healthy 26-year-old man due to diffuse metastasization of adrenal paraganglioma caused by rupture of the primitive tumour with subsequent massive haemorrhage after a relatively minor trauma. Our report describes the results of forensic investigation and discusses the possible mechanisms of metastasization.
Introduction
Retroperitoneal haemorrhage can be either spontaneous or post-traumatic. The most common reported causes of retroperitoneal haemorrhage include rupture of abdominal aortic aneurysm, adrenal bleeding, haemorrhagic pancreatitis and renal causes of spontaneous haemorrhage. 1–4 The kidneys are involved in about 25% of abdominal traumas. Pathologically altered kidneys, as in hydronephrosis, cysts and tumours, are more likely to be associated with retroperitoneal haemorrhage. 5,6
Although trauma-induced adrenal haematoma was first reported in 1863, this particular cause of adrenal bleeding is considered to be an unusual one, 7 and almost only ever associated with pathologies that cause an enlargement of its volume, such as cysts. 8
We report an unusual death of an apparently healthy 26-year-old man due to metastasization of adrenal paraganglioma caused by rupture of a primitive adrenal mass possibly after a relatively minor trauma.
Case report
A 26-year-old single man with an unremarkable medical history was taken to hospital after a blunt back trauma caused by a fight with his brother. He was kicked and punched repeatedly in several parts of the body, in particular in the region of the left kidney in the lower back, which caused a subcutaneous haematoma. Computerized tomography (CT) of the abdomen, performed at the local Emergency Department, showed a large retroperitoneal haematoma (14 × 11 cm2). The results of abdominal angiography were essentially normal, except for some abnormalities in minor lumbar vessels which may have contributed to internal bleeding. The patient underwent a successful embolization procedure of these lumbar vessels, and a few days later he was discharged from the hospital in seemingly good condition. Two months later, he woke up with a progressively worsening discomfort in the lower left quadrant of the back, which eventually became frank pain. He returned to the hospital and a CT of the abdomen showed now a large mass in the left retroperitoneum (23 cm in diameter), round in shape, with central fluid content and a solid periphery. The mass was located behind the body of pancreas and pushed the spleen upward and forward, thus moving forward stomach and pancreas as well. It extended up to the superior pole of the left kidney, forcing it to descend below its normal position. A biopsy was performed and histological examination showed that the neoplasm had a biphasic component: one component was represented by lobular areas consisting of clearly granular cytoplasm cells, lacking in frank cytological atypia. The second component consisted of perivascular cells with a haemangiopericytoma-like pattern. This second cell population showed frank atypia, along with high mitotic index (expression of Mib1 = 50%). The first cellular component stained positively for neuroendocrine–neuroectodermal markers by immunohistochemistry as follows: synaptophysin, Leu 7 (CD57), protein S-100, CD99 and chromogranine. The same cells are also usually positive for vimentine and sporadically positive for BCL-2 and calretinine. They were negative for: cytokeratin pool, haema, actin, CD34, CD117, PLAP, HMB45 and Melan. The second cellular component, frankly atypical, appeared undifferentiated from an immunophenotypical point of view as well, as the cells showed only focal expression of vimentin, CD99 and actin; they stained negative for all other markers among the above mentioned. These data are strongly suggestive of a biphasic retroperitoneal neoplasia with a paraganglioma-like neuroectodermal-derived cellular population and a component with differentiated sarcoma features.
That very night, the patient's general condition rapidly worsened with progressive respiratory failure, until he died.
Since the man was originally admitted to hospital following a fight, a penal trial began, and the judge of the criminal division of the court of first instance competent for the case requested a postmortem examination. Autopsy was performed 48 hours after the man's death. The body was 179 cm high and weighed 70 kg. External examination of the body revealed peripheral cyanosis. No evident signs of trauma could be observed.
Internal examination led to the following findings: lungs displayed marked congestion, mainly at the bases, and bilateral apical oedema. White nodular formations were found at the left pulmonary bases. Such formations appeared to be in continuity with analogous formations, which appeared to adhere to the upper surface of the left side of the diaphragm; these structures weighed 120 g. Perioesophageal metastatic lymph nodes were also found, mainly in the lower third of the oesophagus.
The left hemiabdomen was infiltrated by whitish neoplastic material with necrotic elements. The mass involved the retroperitoneal region and surrounded most of the small bowel. Neoplasia infiltrated the abdominal wall as well. The neoplastic mass took on a frankly haemorrhagic appearance on the omentum. The abdominal organs were in normal position.
Microscopic examination of several fragments taken from sites involved by the neoplasm (retroperitoneal masses, lymph nodes below and above the diaphragm, periaortic neoplastic tissue, neoplastic infiltration of the left lung and the liver) showed the same histological features as the first histopathological examination. The morphological and immunophenotypical findings point to a malignant neuroendocrine neoplasia that, if considered in conjunction with clinical history, can be identified as a malignant paraganglioma (Figure 1).
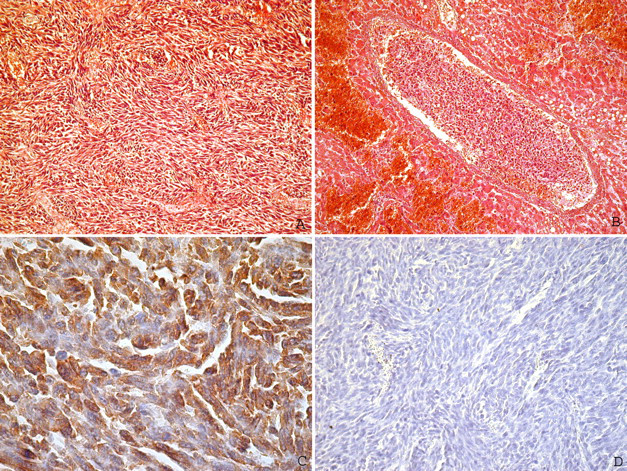
(A) Microphotograph in haematoxylin–eosin of the neoplastic population, (B) neoplastic embolus in the hepatic circulation, (C) immunohistochemical positivity for synaptophysin and (D) immunohistochemical negativity for cytokeratins
The cause of death was determined to be multiorgan failure secondary to metastasis of adrenal paraganglioma. Whether the rupture mechanism of the capsulated adrenal paraganglioma was spontaneous or traumatic remained unclear, but since a post-traumatic rupture was more likely, death was classified as an accident.
Discussion
This report summarizes a case of solitary adrenal paraganglioma complicated by retroperitoneal haemorrhage with the possible spread of the neoplastic cells in the abdominal cavity after a trauma, which did not initially raise specific suspicions. Left retroperitoneal haemorrhage and physical rupture were the main clinical findings at the time of hospital admission, while whitish and diffusely necrotic neoplastic material in the retroperitoneum, in the left abdomen and around the small bowel, was the main autopsy finding.
Adrenal haematomas are associated with injury of several non-adrenal organs, especially liver, spleen, kidney, chest and spine. As a consequence, although isolated adrenal haematomas may occur, the presence of an adrenal haematoma should require a careful search for other injuries. In fact, even if the exact mechanism of adrenal gland injury has not been proved, the fact that the adrenal glands are small, relatively well-protected structures in the retroperitoneum makes it not surprising that these injuries only occur in patients who have sustained very severe traumas. Sevitt proposed two mechanisms of injury – severe hyperextension and lateral compressive force – either of which can result in direct injury that is probably due to compression against the spine. 7
Trauma may have direct effects on the clinical course of cancer by directly enhancing its invasion and dissemination, but in most cases these are more likely to be due to post-traumatic inflammation and to be only indirectly linked to trauma. In particular, post-traumatic inflammatory response may promote the growth of micrometastases by enhancing intraneoplastic neovascularization. Direct or indirect effects on invasion and metastasis probably do not follow an ‘all or nothing’ rule, but they are rather the result of the acceleration of processes that would still have taken place even if the trauma had not occurred. From a medicolegal viewpoint, it is exceptionally difficult to estimate the acceleration of a process whose natural rate of progression is unknown in individual cases.
Literature reports have clearly shown that the entry of cancer cells into lymphatic and blood vessels may be enhanced by mechanical trauma, which may be associated with increasing intratumoral pressures, with accidents, or with traumatic diagnostic and surgical procedures. 9
The forensic interest of this case is related to the eventually voluntary nature of the injury. Although the case emphasizes that even seemingly insignificant trauma could trigger lacerations of a capsulated adrenal neoplasm with possible release of neoplastic cells into the abdominal cavity and initiation of a metastatic diffusion, the culprit was not indicted with the charge of voluntary manslaughter.
In fact, in the area of the Italian criminal law, it is absolutely essential to demonstrate that there is a causal link, because in order for a fact to be considered a crime it must invariably be based on an unquestionable and proven causal link; the fact must be evaluated in terms of certainty and not merely in terms of lesser or greater probability; between the fact and the violation of the law which, in the case of personal injury must consist in the fact of having caused such injury concretely, as a direct cause of a given injury-causing action. The Court of Cassation has often specified that the causal link in technology-related diseases may be assessed in terms of ‘reasonable certainty’ whenever there is a ‘high degree of probability’ and of ‘qualified probabilities’.
Footnotes
Acknowledgements
This study was supported by Fondi di Ateneo, Linea D1, Università Cattolica del Sacro Cuore. Francesco Ausania and Fabio De Giorgio contributed equally to this work.