
Abstract
Introduction
This study was carried out to evaluate data about trauma-related winter sports, including risk factors such as high speed, gender, age, alcohol consumption, details about the accident and snow conditions.
Methods
A retrospective review was conducted to determine the injury patterns and crash circumstances in holiday skiers and snowboarders. The data recorded were obtained from the database of the Pre-Hospital Emergency Registry of six skiing areas in the Dolomite mountains during the winter seasons November 2004–May 2009, injury data for major traumas from Ski Patrol Injury reports (helicopter, ambulance or ski slopes' patrol reports), and intrahospital Emergency Department data. Alcohol concentration in blood was detected in 200 individuals suffering from major trauma.
Results
A total of 4550 injured patients, predominantly male (69%), mean age 22 years (range 16–72), were included in the observational analysis. Knee, wrist and shoulder injuries were frequently associated with major thoracic, abdominal or head traumas (64% of cases). Suboptimal technical level, high speed, low concentration, snow or weather conditions, faulty equipment and protective devices were among the various causes of accidents. The analysis revealed that high alcohol blood concentration was present in 43% of 200 patients.
Conclusions
Even though the major causes of accidents were excessive speed, excessive fatigue, technical errors and bad weather conditions, alcohol abuse was often discovered. Random sampling and a non-systematic detection of alcohol blood levels likely led to an underestimation of alcohol consumption-related injuries. It is recommended that investigations into alcoholic intoxication in injured skiers should be carried out on a large scale.
Introduction
Previous studies have evaluated the severity of skiing and snowboarding injuries. 1 Over the past decade snowboarding has rapidly grown in popularity particularly among young people, and has been accompanied by increasing reports of snowboard-related injuries, especially in the upper limbs, and more severe injuries caused by impacts. 2,3 A variety of factors influence the survival of trauma patients including the severity and site of injury, and the timing and quality of care. Alcohol intoxication plays a significant role in trauma pathogenesis and severity not only in drivers' injuries; so this study has evaluated skiing and snowboard injuries and in particular we have considered the effects of alcohol in winter sports and the association of alcohol with trauma winter recreation activities. Alcohol intoxication, a central nervous system depressant, is reported to be present in 35–50% of traumatic brain injuries (TBIs) and a quarter to a half of patients with acute TBI are intoxicated at the time of injury. 4
A physiological measure of level of consciousness, the Glasgow Coma Scale (GCS), is commonly used to assess severity of TBI. A GCS score of 13–15 is considered as a mild head injury, scores between 9 and 12 are considered moderate and a score of 8 or less is considered severe TBI. A patient's GCS already depressed by brain injury could be further depressed because of the additive effects of intoxication.
In this preliminary study, we have tried to investigate a possible relationship between winter injuries and alcohol use, whether intoxicated patients are more exposed to a risk of injuries of a different severity, and what the mechanisms of injuries are.
Materials and methods
In this study we evaluated 4450 patients with ski and snowboard injuries. Data were obtained from consecutive ski patrol injury reports from a part of the Dolomitic ski area, prehospital rescue care and documentation, and intrahospital care. The reports were gathered during the ski seasons from 2004 to 2009.
With the aim of investigating whether a relationship exists between winter sports accidents and alcohol in a sample of patients with major injury trauma, the following data were collected: age, gender, injury profile, site, mode and mechanism of injury, the severity of injuries (the scores were calculated for the Simplified Injury Severity Score [ISS]), the skill level, type of snow, equipment, weather visibility, month, day of the week on which the injury was sustained, the degree of incline of the slope where the accident occurred, technical ability and physical condition, speed and type of care. Skill levels were investigated by self-declaration or – when the patient was not able to respond – by friends, relatives or other people. Skill levels were assigned according to three levels: beginner, little experience, middle level or intermediate, and expert or advanced ability. The technical factors were categorized as excessive speed with respect to skill ability, safe speed with control of ski or snowboard, poor ability, high speed or excessive speed out of control. The mechanism of injury was categorized as fall, jump, collision with object or person, fall and jump. The documentation of alcohol concentration was possible in only 200 victims of major injuries that required medical attention in prehospital care; injuries not requiring medical treatment such as minor contusions, abrasions and cuts were not included.
Data collected by the rescue teams served by different Emergency Medical Services (SUEM 118) were retrospectively analysed. Cardiopulmonary parameters, clinical findings, body temperature and the severity of injuries were recorded on the arrival of the medical rescue on the scene. The severity of injuries was graded in prehospital care according to GCS, ISS, Revised Trauma Score and Trauma Injury Severity Score. Blood samples were taken directly in the emergency room and determination of blood alcohol concentration (BAC) was done in the Hospital Central Laboratory (ALC – Dimension method sensibility ≥0.1 g/L). To facilitate prehospital medical intervention in the mountain regions, three Helicopter-Transported Medical Teams (HMTs) were introduced in the Dolomite areas. The HMT crew with special education and training in prehospital mountain emergency care consists of an anaesthesiologist, a nurse and the pilot. The HMT is activated by the Emergency Medical Services 118 or by emergency paramedic services at the scene of the accident. The prehospital chart reported all clinic notes, date and time of injury, mode of transportation to the emergency department, all operative reports, prehospital rescue and onboard helicopter interventions.
Results
A total of 4550 injuries were reviewed from six winter seasons (2004–2009). Injured skiers and snowboarders were predominantly male (69%); the snowboarding patients' mean age was 22 years (range 12–38) and the skiing patients' mean age was 33.5 years (range 16–72). In a population of 84 skiers and 116 snowboarders who were reported to have severe injury requiring immediate medical advanced evaluation and treatment, BAC was analysed upon arrival in hospital. The mean BAC was high in patients injured in violent accidents (Figure 1). When considering the ability level of those injured, a high percentage of injuries involved beginners (43%) and intermediate (45%) skiers and snowboarders (Figure 2).
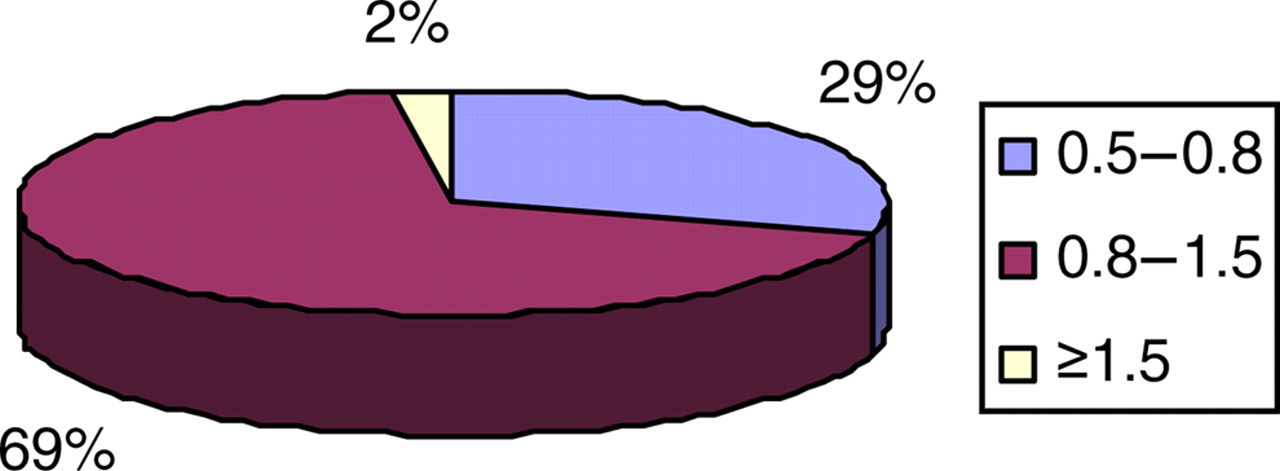
Alcohol-positive patients (BAC ≥ 0.5 g/L). BAC, blood alcohol concentration
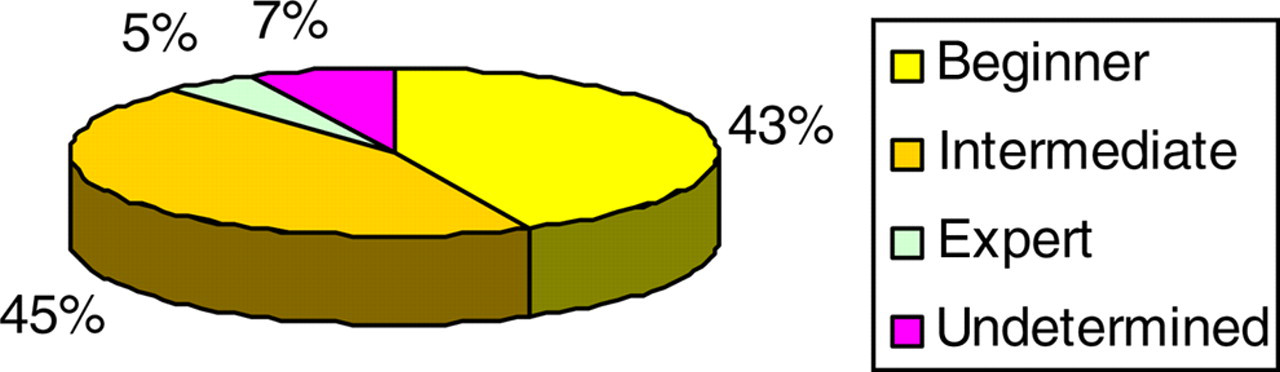
Skill level and injuries
The mechanism of injuries is reported in Figure 3. The causes of accidents were fall (32%), collision with object (protective fence, snow bank, signboard, guidepost, tree) or a person (17%), or fall during jumping (39%). The most frequent situation resulting in an impact or collision was the loss of control of the skis or snowboard. Especially in snowboarding, the risk of injury associated with jumping is significant. Looking at the weekly distribution (Figure 4), no significant differences were found in the rate of injuries during workdays, with only a slighter higher incidence on Sundays. Regarding the length of time the person had been skiing or snowboarding before the injury (less than 2 hours, 3–6 hours, more than 6 hours), most people were injured in the afternoon (Figure 5). The anatomical location and frequency of injury in the population studied is shown in Figure 6. The injuries were classified as head, thorax, abdomen, upper and lower extremity fractures. Knee, wrist and shoulder injuries were frequently associated with major thoracic, abdominal or head traumas (64% of cases). The major head injuries were the result of falling to the ground on icy, hard-packed snow. GCS of the study population at a prehospital evaluation is reported in Figure 7. The type and percentage of winter sports requiring medical care are reported in Figure 8.
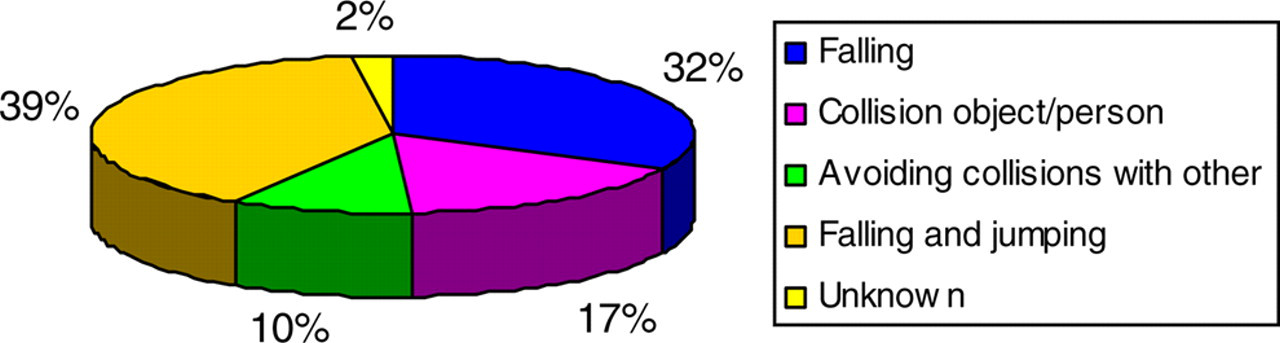
Mechanism of injuries

Occurrence of injuries on different days of the week

Injuries in relation to the hour of occurrence

Anatomical regions of the injured body
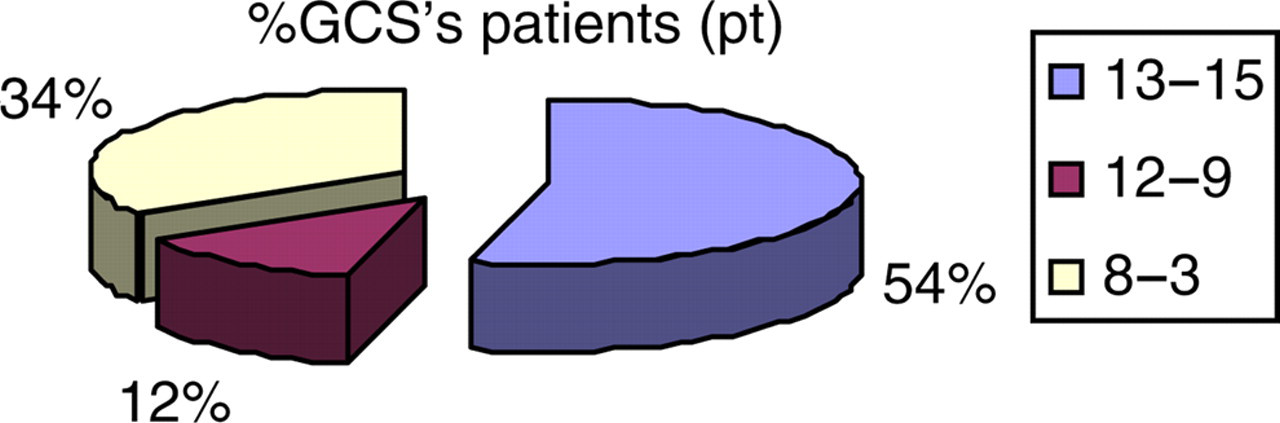
GCS in the field and during emergency treatment. GCS, Glasgow Coma Scale
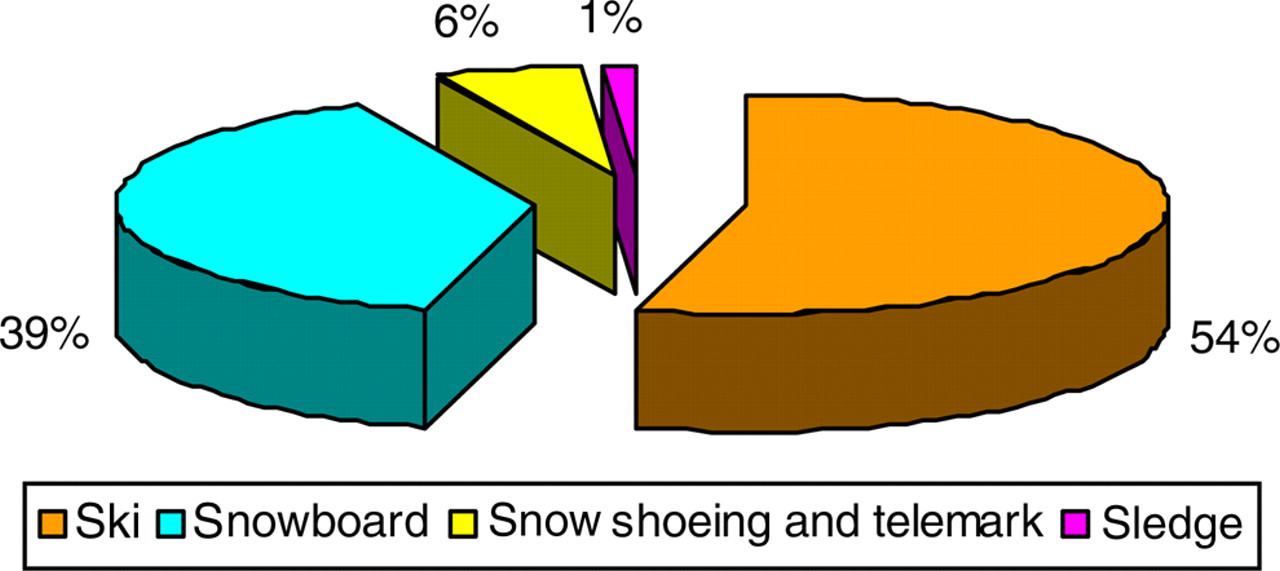
Percentage of winter sports requiring medical care
On-site intensive medical treatment and monitoring with airway management and intubation were required in 24% of patients. Six victims were declared dead on site and therefore were not included in this analysis.
Discussion
A continuing increase in the number of people practising winter sports, such as skiing and snowboarding, along with heedless behaviours (unawareness, excessive high speed on the ski run, lack of accurate monitoring of undisciplined users, etc.) have led to a significant increase in the injury rate and fatal accidents . 2,5 Even though according to the previous literature a fatal accident during winter sports is a relatively rare event, 6,7 a relevant impact trauma may often be responsible for severe brain damage, cardiogenic or haemorrhagic shock.
The presence of alcohol in the blood is among the important causes of accidents, with unpredictable and indefinite influence on technical ability or ski control. Moderate-to-high BAC could be a serious danger especially for beginner skiers who lose their balance quickly and are unable to compensate in time the heavy impact of a fall onto the snow surface.
TBI remains the leading cause of death and disability in young adults. The wearing of helmets is actually becoming more socially acceptable among young people and several reports have documented that helmets may be beneficial, particularly for children and adolescents. 8,9 However, some authors have reported that if helmets are not properly designed, they may interfere with hearing and sight and may increase the risk of other injuries. 8
The availability of a helicopter medical service reduces mortality by extending rapid rescue and emergency medical care to victims. Because of their geographic location, the helicopter rescue teams of the Dolomite area serve different hospitals within a 15–18-minute flight distance. Medical doctors able to provide for advanced life support on the scene and trained in the field of emergency medicine receive ski courses from professional ski instructors in order to improve their skiing technique and skills on different slopes and off-piste places. They provide for basic and advanced life support on the scene and organize hospitalization. The use of a prehospital database chart is particularly advantageous; actually, the diagnoses are usually made by medically qualified personnel (mainly interviewers) and only rarely by ski patrol or first-aid trained personnel.
In the present study, 12% of injured individuals were found to have a GCS between 12 and 9, and 34% between 8 and 3. It is commonly assumed that alcohol intoxication reduces the GCS, which is widely used for clinical decision-making and triage in prehospital settings and to guide diagnosis and management of TBI. A history of alcohol abuse limits GCS utility in head trauma patients. The decrease in the level of consciousness observed in our injured patients with high BAC could also have been the result of factors other than alcohol intoxication, the most important of which is the severity of brain injury. Other factors that may depress the level of consciousness include hypothermia, hypoxia, hypercarbia, the presence of shock, the concomitant use of other central nervous system depressants and other severe non-neurological injuries.
In epidemiological studies the incidence of injury rates is expressed in two ways:
In terms of injuries per 1000 skier-days (IPTSD) = (number of injuries)/(number of skier-days) per 1000. As reported in Table 1 some authors evaluated ‘skier-day’, others ‘skier-visit’. There is a subtle difference between the two terms: ‘skier-visit’ actually stands for the number of people who visited the ski area, but not necessarily all skied. Recent studies report the injury rate calculated on skier-days. In terms of mean days between injury (MDBI) = (number of skier-days/total number of injury reports) injury rates are usually reported per 1000 skier-days (the number being determined by the number of lift tickets sold on a given day.
9
Injury rates for alpine skiing and snowboarding in the international literature vary from 7 to 2 injuries per 1000 skier-days (Table 1). Deibert et al.
8
reported that before 1975 the rate of injury in alpine skiers ranged from 5.0 to 7.6 injuries per 1000 skier-days; by 1982 the rate had decreased to 3.0–3.5 injuries per 1000 skier-days; in 1989 the rate was 2.0 injuries per 1000 skier-days; and in 1994 the rate was 4.27 per 1000 children skier-days compared with 2.69 injuries per 1000 adult skier-days.
8
Warme et al.
10
reported 3.7 injuries per 1000 skier-days in a large study. The number of skier-visits was calculated on the basis of the total number of sales of ski-lift tickets. In 1999 O'Neil and McGlone
3
reported an incidence of 4% of injuries in first-time participants in both snowboarding and skiing.
Descriptive statistics of frequency of injuries (per 1000 skier-days)
Our data from 2004 through 2009 reveal an injury incidence of 3.4 per 1000 snowboarder-days, and 2.6 per 1000 skier-days. We tried to calculate the rate of injuries per skier hour but it was very difficult to determine how long they had been skiing or snowboarding.
The risk of injury often increases dramatically during competition, but the people in the present study were participating in winter sports at a non-competitive level. This study is an observational study which documented the BAC only in individuals with severe ski-related injuries, a minor proportion of the population of trauma patients. Further evaluation and comparison with other epidemiological data in these recreational activities are required.
Conclusion
Even though the major causes of accidents were excessive speed, fatigue, technical errors and bad weather conditions, alcohol abuse was frequently reported. Random sampling and a non-systematic measurement of blood alcohol levels is likely to have led to an underestimation of alcohol consumption-related injuries. Extending BAC determination also to individuals with minor trauma might have led to better discrimination of the real impact of alcohol on physical performance. Jumping after alcohol consumption consistently increases the risk of underestimation.
The strict implementation and enforcement of legislation along with health education will help to prevent snow-sport trauma. Prevention strategies should include the use of protective equipment (helmets, back protectors, wrist guards, padded gloves), regular exercise and proper gymnastic training to prepare for jumping. Alcohol abuse during winter sports is still largely underestimated and very difficult to demonstrate.
Footnotes
Acknowledgements
The authors gratefully acknowledge the support of Mariaelena Molinari for her contribution to the manuscript translation.