
Abstract
We describe an unusual case of total replacement of the exocrine pancreas with fat, which was observed in an autopsy of an assaulted victim. A woman in her early 80s was kicked, stamped and hit several times with firewood. She was hospitalized with disturbance of consciousness, left haemothorax and multiple fractures, and died about three months later. Postmortem examination revealed extensive abrasions and bruises, multiple fractures and internal organ injuries such as contusion and haemorrhage, as well as bronchopneumonia. It was concluded that the cause of her death was hypostatic pneumonia followed by traumatic shock due to multiple blunt injuries. Further, complete replacement of the pancreas with fat was observed in addition to a calculus in the main pancreatic duct and fibrous hypertrophy of the ductal wall. Histopathological examination revealed almost complete replacement of the pancreatic acini by fat tissue, whereas the islets of Langerhans were mostly intact. Antemortem laboratory data showed that serum amylase levels were almost within normal range before hospital admission, but underwent a transient abnormal elevation at admission followed by extremely low levels thereafter. Previous reports suggest that obstruction of both the main pancreatic duct and the artery, due to tumour formation or calculus in combination with arteriolar sclerosis, are necessary to induce total replacement of the pancreas with fat. Since arteriolar sclerosis was not remarkable in this case, we speculated that pancreatic ischaemia due to circulatory disturbance caused by traumatic shock, in combination with pre-existing calculus, may have contributed to the development of total replacement with fat. The temporal alterations in serum amylase levels support our speculation. There are few, if any, reports regarding organ replacement with fat in association with trauma. This case suggests that multiple injuries followed by traumatic shock may advance pre-existing replacement of the pancreas with fat.
Introduction
Mild-to-moderate fatty infiltration into the interlobular or perilobular spaces of the pancreas is not uncommon, and is occasionally encountered in autopsy cases. 1 It is regarded as a normal finding in the obese and the elderly, and appears to be a reversible lesion. 1–3 However, total replacement of the pancreas with fat is extremely rare. Although the mechanism has not been clarified completely, it is considered to be caused by both obstruction of the pancreatic duct and by chronic pancreatic ischaemia. 4–6 In addition, several predisposing factors including alcohol abuse, diabetes mellitus, hepatic disease, dietary insufficiency, viral infection, steroid therapy, haemochromatosis and fibrocystic disease have been suggested. 4,7–9 We describe here an unusual case of total replacement of the exocrine pancreas with calculus by fat, which was observed in an autopsy case of an assaulted victim. We further discuss the aetiology of total replacement of the pancreas with fat and its relationship to the multiple injuries sustained by the victim in this case.
Case report
A woman in her early 80s was kicked and stamped on her chest and abdomen, and hit on her left arm and temporal region of the head several times with a piece of firewood (length 122 cm, diameter 4.5–6.0 cm, weight 1.66 kg) by a member of her family. The accused stated that he assaulted her because she did not satisfy his demands for money. About two hours after the assault, he called an ambulance for her because her consciousness became unclear. Upon arrival at the hospital, she showed a slight disturbance of consciousness and was diagnosed with left haemothorax, multiple left rib fractures and bilateral mandible fractures. In spite of the intensive care, she died about three months after hospitalization. Two days after her death, a medicolegal autopsy was carried out.
Findings at autopsy
The deceased was 157.0 cm tall and weighed 59.0 kg. Multifocal abrasions and bruises remained on the head, face, trunk and extremities (Table 1). All of the injuries were moderately old. The internal examination revealed multiple organ injuries and fractures. In the cranial cavity, old small subarachnoid haemorrhage on the left frontal lobe and contusions on the left frontal and parietal lobes were observed. In the chest, multiple old fractures of the left ribs (IV–X), an extensive fibrous adhesion between upper lobe of left lung and left parietal pleura, and left pulmonary contusions with fibrous thickening of visceral pleura were found. There was a small laceration in the region of the postcaval entry and a subepicardial haemorrhage in the left ventricle, measuring 2.0 × 1.2 cm2. In the upper extremities, there were old fractures of several bones including left humerus, bilateral radius (left 2, right 1), left ulnae and right metacarpal bones (III, IV, V). Moreover, there were old bilateral mandible fractures, one of which (right side) was fixed by surgical metal plates. In addition to the multiple injuries, there was a moderate amount of dark brown-coloured puruloid fluid in the air passage.
Injuries observed in the deceased
Furthermore, the pancreas was found to be of normal shape (100 g) with superficial lobular marking, but the similarity in colour made it difficult to distinguish from the surrounding fat tissues. Following sectioning of the pancreas from head to tail after formalin fixation, pancreatic parenchyma appeared to have been almost completely replaced by fat tissue (Figure 1). There was a calculus the size of a red bean in the main pancreatic duct of the head (Figure 1, arrow). The wall of the distal duct from the calculus was remarkably thick (Figure 1, arrowheads). No evidence of haemorrhage was observed in the pancreas.

Serial sections of the pancreas from head to tail after formalin fixation. The arrow indicates pancreatic calculus in the main pancreatic duct of the head. The arrowheads indicate that the wall of the distal duct from the calculus is remarkably thick
Histopathological and physiochemical findings
Histopathological examination revealed congestion in all organs examined. In the corpus callosum and lentiform nucleus, there were a few retraction balls, which suggested damage to axons. In the kidney, myoglobin (Mb) casts were observed in the lumen of the distal tubule. In all lobes of both lungs, there was massive neutrophil infiltration into the bronchiole and pulmonary alveolar spaces.
In the pancreas, there was almost complete replacement of the pancreatic acini by fat tissue, in which scattering of normally preserved islets of Langerhans was observed (Figure 2a). Neither necrotic acinar cells nor inflammatory cell infiltration was found. Immunohistochemical analysis for insulin revealed that the number of β cells in the islets was preserved normally (Figures 2b and c). Consistent with the macroscopic observations, remarkable fibrous hypertrophy of pancreatic ductal wall was observed (Figure 2d). Arteriolar sclerosis was neither remarkable in the pancreas nor in other organs.
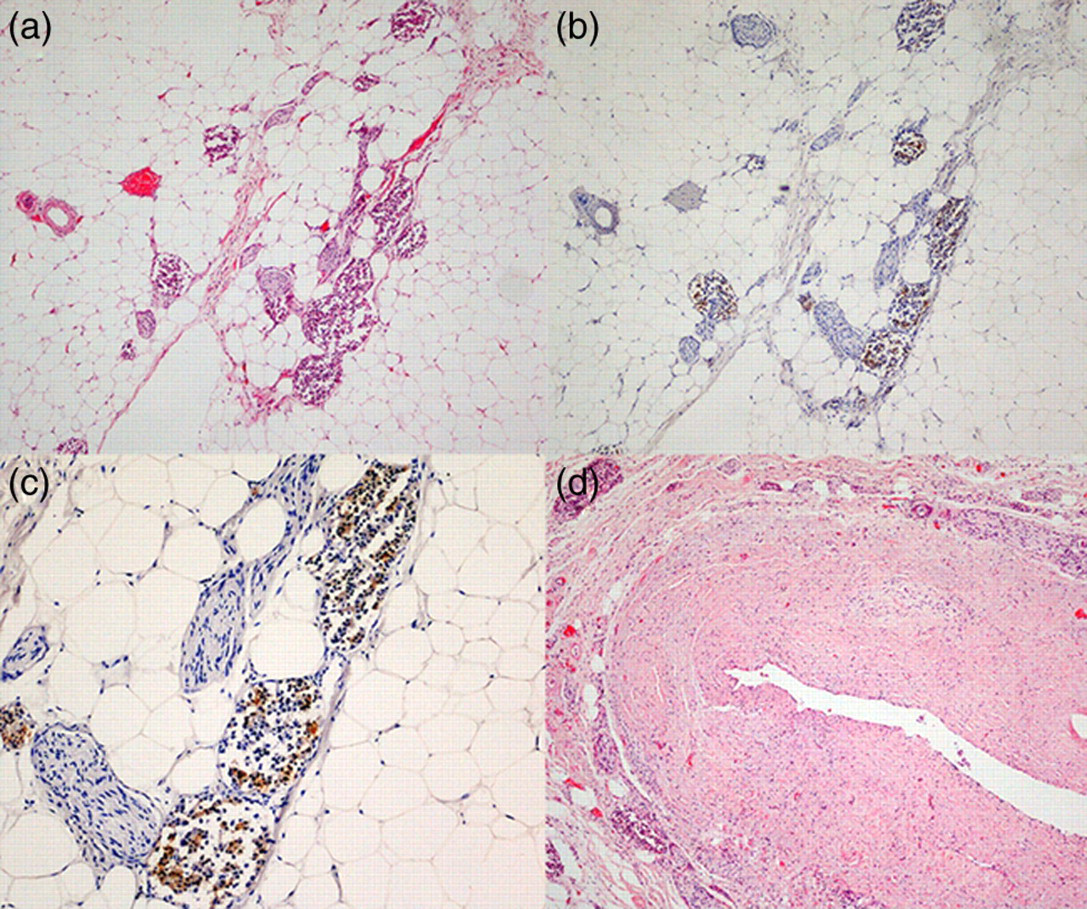
Histopathological examination revealed replacement of the pancreas with fat (a) and remarkable fibrous hypertrophy of pancreatic duct (d) (haematoxylin and eosin; original magnification, 40×). Immunohistochemical analysis for insulin demonstrated that the islets of Langerhans were scattered among the fat tissue and that the number of β cells in the islets was preserved (b, 40×; c, 200×)
HbA1c (forms of glycosylated haemoglobin) level in postmortem cardiac blood obtained at autopsy was estimated to be 6.9% (normal range 4.3–5.8%).
Data from medical records
Abdominal computed tomography (CT) scan, which was performed when the deceased was initially admitted to hospital, revealed a calculus in the pancreatic head and that the whole pancreas had the same intensity as fatty tissue (Figure 3). Assessment of the function of the pancreatic exocrine system showed that serum amylase levels were almost within normal range before hospitalization. However, it showed a transient abnormal elevation (232 IU/L) at admission and thereafter became extremely low (Figure 4). The deceased had mild impaired glucose tolerance, but was not diagnosed with diabetes mellitus before hospitalization. Blood HbA1c level was 5.6% on admission to hospital.

Abdominal computed tomography scan at initial admission to the hospital. The arrow indicates a calculus in the pancreatic head
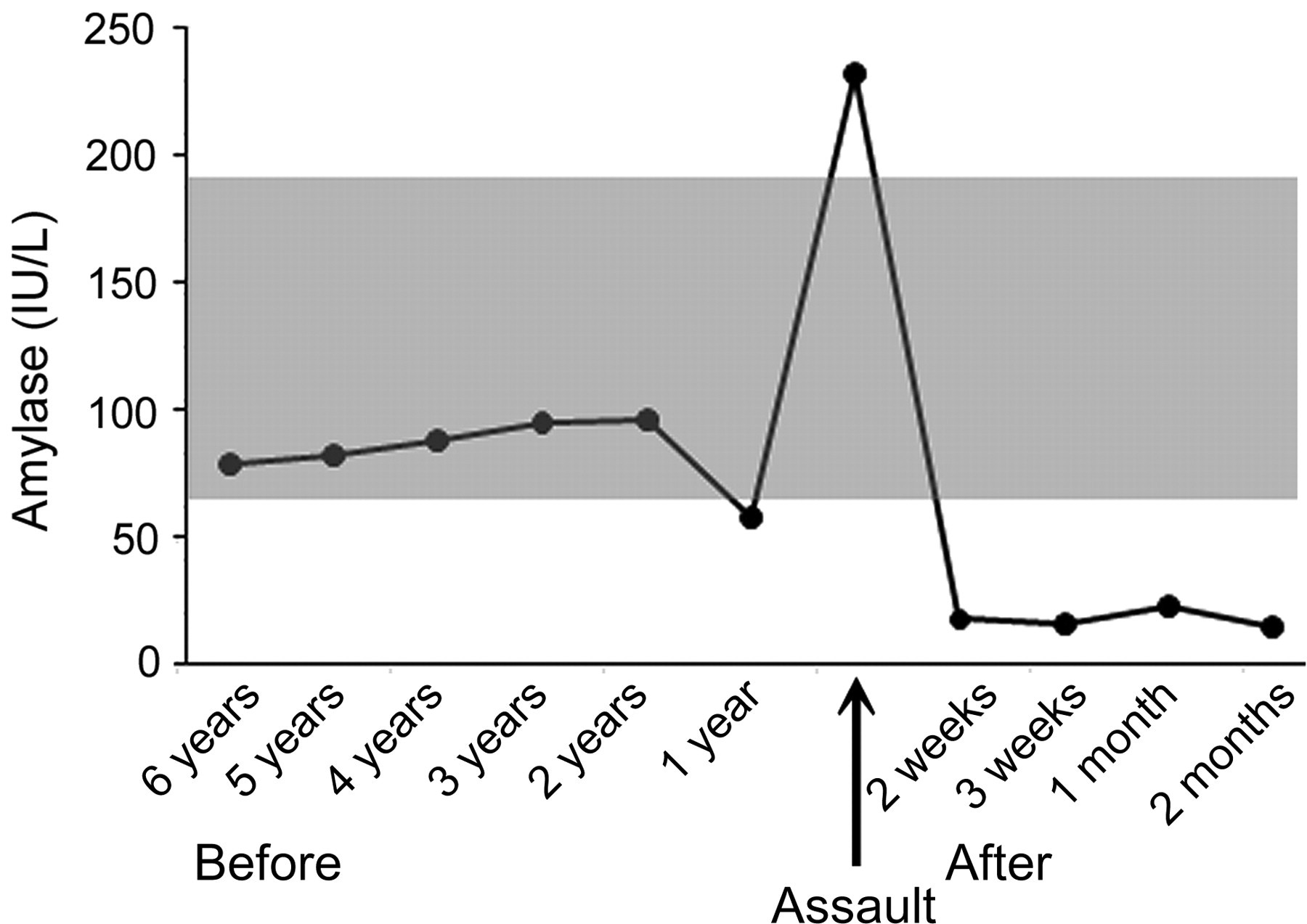
Temporal changes in serum amylase levels from six years before hospitalization until death. The grey zone indicates normal range
Discussion
The victim had a large number of moderately old organ injuries and fractures. According to the wound examinations, all of them were considered to have been sustained during the assault by the accused. Of the injuries observed, the multiple fractures of the left ribs and left pulmonary contusions were sufficient to cause severe respiratory disturbance in the deceased. The cardiac lacerations and cerebral contusions with possible accompaniment of axonal injury were small, but might have had an adverse effect on haemodynamics and consciousness, respectively. Moreover, the multiple fractures could cause not only massive bleeding, but also surrounding muscle detritions, which were evidenced by the presence of Mb casts in the renal tubules. Accordingly, those injuries were considered to be sufficient to cause lethal traumatic shock to the deceased, if intensive in-hospital care was not provided.
Histopathological findings revealed severe bronchopneumonia in all lobes of the bilateral lungs. The bronchopneumonia of the deceased may have represented a hypostatic pneumonia that developed as a result of decline of pharyngeal reflux caused by unconsciousness and pulmonary congestion due to long bed rest. The deceased exhibited loss of consciousness and was prescribed long bed rest due to multiple injures followed by traumatic shock. Thus, we concluded that the cause of her death was hypostatic pneumonia followed by traumatic shock due to multiple blunt injuries.
In addition, the present case exhibited complete replacement of the exocrine pancreatic acini by fat tissue. Although partial (patchy) interlobular or perilobular replacement of the pancreas with fat tissue is common and is considered to be related to ageing or obesity, total replacement of the pancreas with fat is an extremely rare entity. One previous experimental study showed that obstruction of both the pancreatic duct and artery was necessary to induce total replacement of the pancreas with fat. 6 That study emphasized that pancreatic ischaemia was an important factor for replacement by fat. Similarly, in clinical and autopsy case reports of total replacement of the pancreas with fat, obstruction of both the main pancreatic duct and artery by tumour in the pancreatic head was present. 10–12 In cases with obstruction of pancreatic duct by a calculus, pancreatic ischaemia due to capillary disturbance caused by diabetes mellitus contributed to development of total replacement of the pancreas with fat. 4,5
In our case, there was a calculus in the main pancreatic duct and fibrous hypertrophy of the ductal wall, which indicated long-term obstruction of the pancreatic duct. Histopathologically, arteriolar sclerosis in the pancreas as observed in the cases of diabetes mellitus was not remarkable. Moreover, abdominal CT scan upon admission to the hospital already indicated replacement of the pancreas with fat, although serum amylase levels were almost within normal range before the hospitalization. Previous reports suggest that the exocrine pancreas has a great reserve capacity and that exocrine functions are well maintained even when under 5–10% of the entire pancreas is functioning. 13,14 Accordingly, in our case it is considered that the long-term obstruction of the pancreatic duct by a calculus caused partial replacement of a large part of the pancreas with fat even before the present episode occurred.
We speculate that pancreatic ischaemia due to circulatory disturbance caused by traumatic shock may contribute to the development of total replacement of the pancreas with fat. The temporal changes in serum amylase levels (Figure 4) provide evidence in support of our speculation, since a transient abnormal elevation on admission followed thereafter by extremely low levels may indicate release of amylase from necrotic acinar cells caused by ischaemia and near complete destruction of acini, respectively. As necrotic acinar cells may have been eliminated during hospitalization (about 3 months), neither necrotic cells nor inflammatory cells were expected to be observed in the pancreas.
While the exocrine pancreas was almost completely replaced by fat tissue, normally preserved islets of Langerhans were scattered among the fat tissue. Moreover, immunohistochemical analysis showed that the number of β cells in the islets was preserved normally. In most of the previously reported cases of total replacement of the pancreas with fat, the islets were also found to be scattered throughout the fat tissue and kept intact. 4,5,8,10,12 These findings indicate that the islets are resistant to replacement by fat, since the islets are supplied by the first branch of the pancreatic artery and cell viability of islets is greater than that of acinus. While the number of β cells in the islets was maintained at near-normal levels in our case, blood HbA1c level was increased from 5.6% to 6.9% during hospitalization. We speculate that blood HbA1c level was increased due to traumatic stress-induced hyperglycaemia and subsequent release of glycogenolytic hormones such as cortisol, glucagon and epinephrine. Thus, we conclude that replacement by fat was not a contributory factor to her death even from the viewpoint of endocrine function.
In conclusion, we present here a rare case of total replacement of the pancreas with fat, probably caused by circulatory disturbance due to traumatic shock in addition to long-term obstruction of the pancreatic duct by a calculus. Antemortem CT scan and biochemical data provided the supportive findings of the diagnosis. There are few, if any, reports showing total replacement with fat in association with trauma. This case suggests that multiple injuries followed by traumatic shock may further advance pre-existing replacement of the pancreas with fat.