
Abstract
This case report details the accidental death of an elderly gentleman who was a passenger in a motor vehicle accident, the cause and mechanism of death being determined as cardiac tamponade due to a traumatic laceration of the ventricle. The forensic autopsy revealed as an adjunct finding a mechanical trauma to the descending colon, being a perforation of a colon diverticulum due to an ingested toothpick. The historical aspects of toothpicks, risk factors associated with the accidental ingestion of toothpicks and different clinical presentations associated with ingestion and peristaltic migration of toothpicks as a foreign body are discussed.
Introduction
The toothpick as an implement of dental hygiene has been used for thousands of years dating back to 3500 BC in Mesopotamia, with evidence of toothpicks found in oral hygiene kits with toothbrushes in the Ningal Temple in Ur. 1 Anthropologists have found grooved striated markings in the fossilized teeth of Neanderthals living in Europe and Asia, with similar teeth markings discovered in fossilized teeth of American Indians and Aborigines, the markings considered to be due to the use of heavy primitive toothpicks. 2 Skulls of prehistoric man show holes formed from toothpicks made of bird claws, bone, ivory, quills and walrus whiskers. 3
Toothpicks were introduced into Japan in 584 (the Nara period), arriving with Buddhism via China and Korea. Buddha (500 BC) taught disciples to clean their teeth with tufted toothbrushes. 4 Historically the status of individuals was indicated by the type of toothpicks used, with the aristocracy using ‘designer’ toothpicks made of gold, silver and with precious stone inlays artistically stylized and enamelled. Lower classes of society used wood of various trees, twigs, porcupine quills, shells and feathers; many of the woods were aromatic and contained tannic acid, thought to prevent cavities and gum disease. 1
Toothpicks were introduced for general population use between 1300 and 1600, with the first patented toothpick manufacturing machine being developed by Silas Noble and J P Cooley in 1872, 5 and the first mass-produced toothbrush being developed by Addis in 1870 in England. Levi Parmly, a dentist from New Orleans, is credited with inventing dental floss and recommending the use of silk floss in 1815. 6 Toothpicks are still used today in oral hygiene (although dentists prefer flossing) and also in food preparation for decoration and in assisting as an eating utensil.
Accidental or deliberate ingestion of toothpicks has been reported in medical literature related to various disciplines of medicine depending on the clinical presentation and the medical complications caused as a result of the ingestion, with some toothpick incidents presenting as life-threatening emergencies and causing death.
Most ingested foreign bodies, due to their size and configuration, pass through the gastrointestinal tract uneventfully. Toothpicks, being long and slender with sharp-pointed ends and resistant to digestion, have the potential to perforate particular sites of the gastrointestinal tract, and thereafter due to peristaltic action to exit the wall of the tract at vulnerable sites and penetrate a variety of adjacent anatomical structures, with the injury often being associated with diagnostic difficulties and substantial morbidity and mortality.
Case report
The deceased was a 92-year-old man, described as in relatively good health for age, and was the passenger in the right front seat of a vehicle driven by his spouse, travelling in a westerly direction. The vehicle was involved in a three-vehicle collision resulting from another vehicle travelling in an easterly direction toward them, crossing to the incorrect side of the road where it impacted with the offside part of the car where the deceased was a passenger. Due to the initial collision the vehicle in which the deceased was travelling lost control, and continuing in a westerly direction crossed to the wrong side of the road colliding with another vehicle travelling eastbound. The main impact was on the right-hand passenger side where the deceased was sitting.
At the accident scene the deceased remained in the vehicle, with witnesses describing him as having shallow breathing and appearing unconscious. In the report of the death to the Coroner, the police stated the deceased died at the scene of the accident.
The external autopsy examination revealed extensive abrasions to the left side of the face, cheek, nose and lip, with a bruise abrasion on the lateral aspect of the left supraorbital ridge. Bruising was present on the left wrist with an abrasion on the left side of the knee. The posterior left calf had an extensive superficial laceration as well as a laceration to the medial side of the right lower leg. Surgical scars were present from the right groin to the right lower leg in addition to abdominal surgical scars in the epigastric area and lower abdomen. Evidence of skin grafts was present on the lower right leg.
The internal examination of the thoracic cavity demonstrated moderate congestion and oedema of both lungs. The heart appeared enlarged, weighing 604 g, and was globular in appearance due to distension of the pericardial sac with over 500 g of clotted blood. Serial sections of the coronary arteries revealed moderate atherosclerosis with calcification and an area of short deep plaque of highly calcific occlusive atheroma at the origin of the anterior descending branch of the left coronary artery. There was a 1 cm laceration of the left ventricle on the epicardial surface with adjacent bruising, the laceration penetrating into the right ventricular cavity with extensive disruption of the deeper layers of the right ventricular muscle. There was a transverse fracture of the upper portion of the body of the sternum. The aorta had progressive atherosclerosis inferiorly and the lower abdominal portion of the vessel had been replaced by a trouser graft.
Examination of the abdominal organs revealed a minor degree of diverticular disease. In the lower descending colon, a diverticulum had a mechanical perforation evident, with the blunt end of a foreign body – being a wooden toothpick – still in situ and protruding to the exterior. There was little local reaction, or evidence of peritonitis (Figure 1).
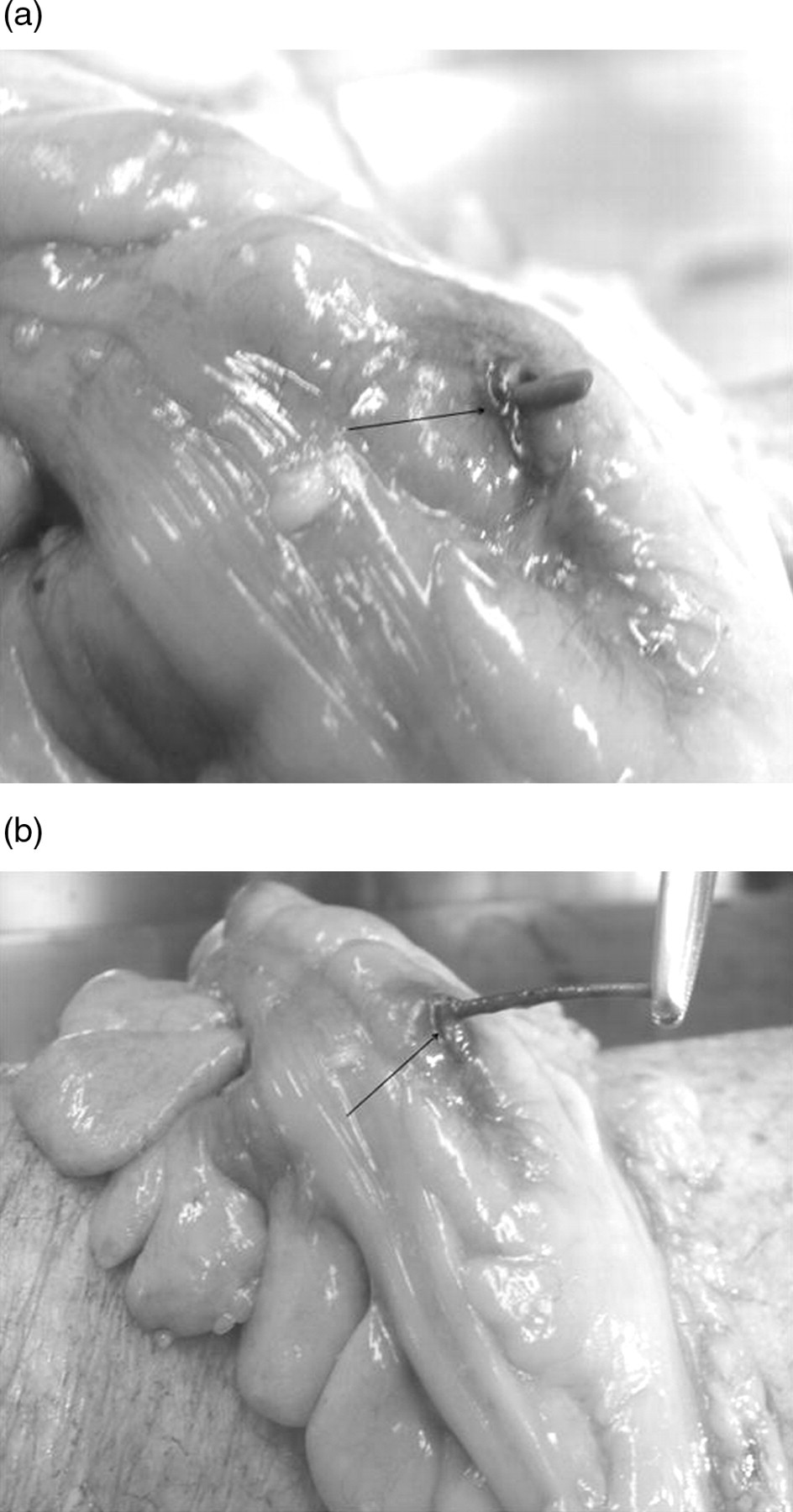
(a) Toothpick protruding (arrow) from a perforated descending colon with minimal local reaction, and absence of peritonitis. (b) Toothpick being extracted (arrow) from the colon diverticulum, illustrating resistance to effects of digestion
The cause and mechanism of death was a cardiac tamponade due to a traumatic laceration of the ventricular muscle associated with the fractured manubrium due to the vehicular impact.
Discussion
There are several predisposing factors associated with accidental toothpick ingestion, with the potential for significant morbidity and mortality. Clients in institutional and residential psychiatric and developmental disability facilities with behavioural disorders often swallow foreign bodies and consume food without chewing; this is associated with gluttony, poor deglutition and mastication, and altered oral sensation.
The serving of inappropriate food types for the type of disability is a potential for food asphyxiation, as also are medications patients are receiving that may be sedative or have side-effects such as excessive salivation, inhibiting effective swallowing.
Habitual chewing on toothpicks and/or using the toothpick as a fashion accessory by chewing on it are potentially hazardous as well as prisoners swallowing toothpicks and other foreign objects for secondary gain for access to a medical facility.
Edentulous individuals wearing dentures experience a decrease or elimination of tactile sensitivity of the palatal surface required for identification of small and sharp items such as toothpicks 7 as well as decreased sensitivity with the ingestion of hot and cold foods and fluid, and with rapid ingestion of food 8,9 increasing the potential for accidental swallowing of toothpicks.
Excessive consumption of alcohol with food at social functions not only increases the risk of the ‘café coronary’ phenomena reported in the literature 10 but also the potential for ingesting toothpicks with various finger foods, without recollection of the event until signs and symptoms become evident days, months or years later. A case of a plastic cocktail toothpick ingested accidentally 15 years previously presented clinically as microscopic haematuria and a right hydroureteronephrosis. 11 The toothpick exiting the caecum formed an abscess, and then migrated posteriorly to the right ureter causing an obstruction.
Associated with the failure of the patient to remember the event are the diagnostic difficulties associated with toothpicks accidentally ingested, with perforations along the tract presenting clinically as peritonitis with localized infection and pyrexia, as well as mimicking other medical conditions due to the migration of the object affecting other anatomical systems.
Toothpicks being mostly made of wood are radiolucent and therefore not detected on plain radiographs, while computed tomography is of low sensitivity diagnostically. Most cases of accidental toothpick ingestion are diagnosed definitively by laparotomy, followed by endoscopy and various imaging studies. 12
Due to the tortuous anatomy and angulations of the gastrointestinal tract various points of the tract are more susceptible to perforation with long, sharp migrating objects, especially the duodenum, 13 ileocaecal area and appendix, 14 the splenic flexure and sigmoid colon as well as anatomic anomalies such as Meckel's diverticulum. 15
Unusual cases reported in the literature demonstrate the seriousness of migrating toothpicks after perforation of the gastrointestinal tract, affecting the cardiovascular system and accompanying diagnostic elusiveness causing significant morbidity and death in some cases. 16–18 A toothpick perforating the gastric wall and entering the pericardium caused a constrictive pericarditis, 19 while a patient suspected of having a postinfarction rupture of the ventricle was found at surgery to have a perforation of the right coronary artery. 20 The perforation resulted in a cardiac tamponade due to a 3.5 cm wooden toothpick swallowed at a barbecue the previous night. Cockerill et al. 16 reported a ruptured sigmoid diverticulum, with a communicating fistula with the right hip, resulting in osteomyelitis due to a toothpick in the mid-portion of the fistulous tract.
In the present case the blunt end of a toothpick entered the orifice of a descending colon diverticulum causing a perforation, and was discovered as an adjunct finding unrelated to the primary cause and mechanism of death due to the motor vehicle accident. Consultation with the deceased's family in this case failed to confirm any previous history of the deceased person mentioning ingestion of a toothpick, attending functions where such implements were part of the food presentation, any prepared meals or food purchases where toothpicks were utilized, and no complaints of any abdominal discomfort by the deceased.
The deceased person also had his own natural dentition, eliminating the wearing of dentures and associated lack of tactile sensitivity as a predisposing factor to ingesting the toothpick.
The absence of signs and symptoms of peritonitis associated with an infection was probably due to the toothpick only protruding slightly and forming a seal around the perforation, minimizing the local reaction and potential for significant medical problems and possible diagnostic difficulties in the future, if the deceased had survived the motor vehicle accident.
Footnotes
Acknowledgements
I would like to acknowledge Professor John Hilton who performed the coronial postmortem examination and the NSW Deputy State Coroner, Carl Milanovich, Westmead Hospital/Coronial Morgue jurisdiction, who gave permission to publish details of this case.