
Abstract
Purpose
Sudden unexpected death autopsy is sometimes non-conclusive both from a macroscopic and from a histological point of view, even if carried out according to the guidelines for sudden cardiac death examination. Molecular biology techniques are required in this setting and may play a crucial role in reaching the final diagnosis.
A case report
The postmortem examination and toxicology findings of the body of a young monk found dead in his cell were negative. Rare focal myocardial lymphocytic infiltrates were seen microscopically, associated with interstitial oedema. The findings were not sufficient to diagnose a myocarditis as the certain final cause of cardiac arrest. According to the recent guidelines for sudden cardiac death, a molecular investigation by polymerase chain reaction analysis was performed on samples of myocardium and spleen, with detection of parvovirus B19 DNA in the myocardium. Accordingly, a diagnosis of parvovirus B19 borderline acute myocarditis was put forward as the possible cause of sudden cardiac death.
Conclusion
In sudden death cases in which there is lack of a cause-effect relationship with the postmortem findings, the final report should be expressed as a descriptive association of evidence, not providing unreliable certainty, as the Association for European Cardiovascular Pathology recommends.
Introduction
A case of sudden death (SD) in which a detailed postmortem investigation, including molecular pathology tools, revealed a parvovirus B19 (PVB19) borderline myocarditis as the most reasonable cause of electrical instability is herein reported. This case offers the opportunity to review the criteria and the methodology to be used to diagnose myocarditis at postmortem and the significance of the molecular pathology results when looking for a cause-effect relationship.
SD is defined as natural, unexpected death occurring within one hour of the beginning of symptoms in an apparently healthy subject or whose disease was not so severe as to predict an abrupt outcome. 1
Cardiovascular diseases are by far the leading causes of SD in all communities of the USA and of the European Union, and among them coronary artery disease ranks first.
From a forensic point of view, it is mandatory to rule out unnatural causes, such as external responsibility and drug abuse, which represent the crucial points for the magistrate who actually has no interest in a definitive diagnosis if the hypothesis of a crime can be ruled out.
Nevertheless, even when unnatural causes of death are excluded, the forensic pathologist should proceed further to search for the cause of SD.2–4 When the autopsy carried out according to the best standard of practice remains non-conclusive after a detailed macroscopic and a histological investigation, molecular biology techniques may be useful and may help in reaching the final diagnosis. 5
Case report
A 33-year-old Italian monk was found dead in his cell at 7.30 hours. He had retired the evening before at 23:00, without complaining of any symptoms. The parents reported negative family history of SD, healthy past medical history and no alcohol, smoking or drug addiction. No 12-lead electrocardiogram tracing was available for revision.
The autopsy was carried out four days after the discovery of the corpse.
There were no remarkable external findings presented. Macroscopic findings were negative, except for multiorgan congestion and pulmonary and cerebral oedema. The heart was removed in toto for detailed examination. Tissues, blood and other fluids for toxicology and molecular pathology were taken before fixing the tissues and the whole heart in formalin 10%, as suggested by the European guidelines for autopsy investigation of SD. 5 The heart weight (360 g), dimensions (transversal diameter 10.5 cm and longitudinal diameter 9 cm, respectively) and wall thicknesses (left ventricle 10 mm, septum 12 mm, right ventricle 3 mm) were within normal limits.
Origin and course of the coronary arteries were regular, with a non-obstructive eccentric plaque in the left anterior descending branch. Atrioventricular and semilunar valves were normal.
Multiple 10 mm-thick transverse short axis slices of the heart were examined from the apex to the mid-ventricular level without abnormalities.
According to the aforementioned protocol, mapped labelled blocks were obtained circumferentially from a transverse slice and included the left ventricular free wall(anterior, lateral and posterior wall), the interventricular septum (anterior and posterior) and the right ventricular free wall (anterior and posterior). After formalin-fixation and paraffin-embedding, the routine staining (haematoxylineosin and Heidenhain trichrome) were performed. At histology, rare focal inflammatory infiltrates .14 cells/mm2, mostly consisting of T-lymphocyte at immunohistochemistry (CD43 and CD3 positive), were found, in the absence of clear-cut evidence of myocyte necrosis, small vessel disease and fibro-fatty replacement (Figure 1). Myofibre waviness was an additional finding. A toxicological sample was tested to rule out drug addiction.
Histological sections of the left ventricular myocardium, showing focal lymphocyte infiltrates. Haematoxylin and eosin: (a) × 320 and (b) × 250
Molecular analysis revealed the presence of PVB19 DNA in the myocardium, whereas it was negative on extracardiac samples (spleen and blood), thus excluding a contamination (Figure 2). Negative polymerase chain reaction (PCR)/ reverse transcriptase (RT)-PCR results were obtained for other cardiotropic viruses.
Gel electrophoresis: lane 1: marker VIII; lane 2: PCR of PVB19 positive control (218 base pair); lane 3: PCR of PVB19 negative control; lane 4: PCR of parvovirus B19 (PVB19) in myocardium (218 base pair); lane 5: PCR of PVB19 in spleen; lane 6: PCR of PVB19 in autoptic blood. PCR, polymerase chain reaction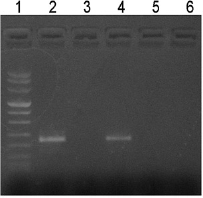
A final diagnosis of ‘borderline’ PVB19 acute myocarditis was put forward as a possible cause of SD.
Discussion
Up to 20% of SDs among young adults and athletes are the consequence of acute myocarditis.6,7 Cardiac manifestations range from subclinical disease to SD, with new-onset atrial or ventricular arrhythmias, complete heart block, or an acute myocardial infarction-like syndrome. In the most severe forms, acute myocarditis may present with congestive heart failure, left ventricular dysfunction and cardiogenic shock. Many patients have a complete recovery, but sometimes they progress towards dilated cardiomyopathy. 8 From a clinico-pathological viewpoint, focal inflammatory infiltrates can be associated with major arrhythmias, while diffuse acute myocarditis is able to sustain a dramatic ventricular dysfunction (‘fulminant myocarditis’). The frequent patchy distribution of inflammatory infiltrates at postmortem underlies the need to perform extensive myocardial sampling covering circumferentially both the entire left and the right ventricle in transverse section, as suggested by the Association for European Cardiovascular Pathology (AECVP) guidelines for SD investigation and confirmed by the case herein reported. 5
According to the Dallas criteria for diagnosis and classification of myocarditis in endomyocardial biopsies from affected patients, 9 myocarditis is diagnosed by traditional haematoxylin–eosin staining in the setting of an inflammatory infiltrate of the myocardium with necrosis and/or degeneration of adjacent myocytes not typical of the ischaemic damage associated with coronary artery disease. However, Dallas criteria apply strictly to endomyocardial biopsy in living patients and their sensitivity has often been questioned. 10 Immunohistochemical techniques allow more sensitive detection and characterization of inflammatory infiltrates. 11 The major pending issue is the differential diagnosis between ‘physiological’ and ‘pathological’ inflammatory cell infiltrates in the myocardium. 5 The presence of inflammatory cells infiltrates in the interstitium of ‘normal’ myocardium is still a controversial issue. A cut-off of five lymphocytes per high power field has been proposed for positive inflammatory cell infiltrate. The Marburg group suggested 14 cells/mm2 at immunohistochemisty as a quantitative criterion for inflammation. 12 In the case herein reported the histopathological findings are scanty and a diagnosis of borderline myocarditis could have been put forward.
We then applied molecular biology tools, which are useful in cardiac SD investigation both for the gene mutational analysis in the setting of inherited cardiovascular disorders and for the search of viral genomes, in the setting of inflammatory cardiomyopathies.
The presence of PVB19 genome in the myocardial specimen and not in the spleen and in the blood samples was suggestive of viral myocarditis, ruling out a contamination.
Different cardiotropic viruses have long been recognized as the most common infectious cause of myocarditis. Among infective agents the enterovirus and adenovirus are the most frequently implicated. More recently, several studies reveal a significant prevalence of PVB19 ranging from 2.5% to 60%13–15 also in the immunocompetent adult. However, the PVB19 was detected also in healthy transplant donors, 16 in autoptic samples without myocarditis 17 and in patients undergoing myocardial biopsy for other reasons 18 or cardiac surgery for conditions not associated with viral infections, 19 possibly as a consequence of previous infection. Overall, PVB19 infection has been linked to a variety of human diseases based on the detection of viral DNA by PCR in the tissue, but the biological and clinical relevance of the presence of PVB19 in tissue remains incompletely understood. In fact, the viral genome has been shown to persist in various human tissues over long periods of time in the absence of clinical symptoms and productive viral replication. 19 Some authors suggest that PVB19 causes myocyte damage indirectly: in situ hybridization revealed PVB19 infecting endothelial cells of myocardial vessels, inducing endothelial dysfunction and migration of inflammatory cells into the myocardial interstitium with subsequent myocyte damage.14,20 Alternatively, it has been proposed that myocarditis arises from immunological cross-reaction to epitopes shared between the virus and the myocardium. 21 Since PVB19 is a frequent and common infection while myocarditis is a rare event, the involvement of other factors, both host- and virus-related, should be investigated to address the true causal role of the virus.
Thus, although PVB19 acute focal myocarditis seems the most reasonable cause of SD due to ventricular arrhythmias in the case herein reported, the scanty histological features in keeping with ‘borderline’ myocarditis and the debatable significance of PVB19 DNA in the myocardium suggest a descriptive diagnosis instead of a definitive one, according to the AECVP guidelines. 5