
Abstract
Aim of study
Psychic trauma is described as the action of ‘an emotionally overwhelming factor’ capable of causing neurovegetative alterations leading to transitory or persisting bodily changes. The medicolegal concept of psychic trauma and its definition as a cause in penal cases is debated. The authors present three cases of death after psychic trauma, and discuss the definition of cause within the penal ambit of identified ‘emotionally overwhelming factors’.
Materials and methods
The methodological approach to ascertainment and criterion-based assessment in each case involved the following phases: (1) examination of circumstantial evidence, clinical records and documentation; (2) autopsy; (3) ascertainment of cause of death; and (4) ascertainment of psychic trauma, and its coexisting relationship with the cause of death.
Results
The results and assessment of each of the three cases are discussed from the viewpoint of the causal connotation of psychic trauma. In the cases presented, psychic trauma caused death, as deduced from assessment of the type of externally caused emotional insult, the subjects’ personal characteristics and the circumstances of the event causing death.
Conclusions
In cases of death due to psychic trauma, careful methodological ascertainment is essential, with the double aim of defining ‘emotionally overwhelming factors’ as a significant cause of death from the penal point of view, and of identifying the responsibility of third parties involved in the death event and associated dynamics of homicide.
Aim of study
The term ‘psychic trauma’ is used here to indicate the action of an emotionally overwhelming factor capable of causing neurovegetative alterations leading to transitory or persisting bodily changes. The neurovegetative changes deriving from a situation of stress and including haemodynamic response, autonomic dysfunction, neuroendocrine activation, inflammatory response and prothrombotic response 1 have a potentially negative influence on the cardiovascular system.
Clinically, the topic has been extensively debated, with the description of instances such as increased mortality during popular football or soccer matches 2 or the risk of cardiovascular events during unforeseen catastrophes such as an earthquake or a terrorist bombing attack,3–6 which are believed to demonstrate a relationship between sudden death and emotional factors. Both acute and chronic psychic stress appear to play a role in causing disorders in cardiac rhythm, potentially correlated with cardiac death.7,8 Also of interest is the work by Engel 9 who, examining 170 case-histories of sudden death associated with emotional factors, showed that intense emotions such as rage, fear or grief on hearing of the death of a close relative or friend were noted in the period immediately preceding death.
The relationship between the precipitation of ischaemic cardiopathy and psychic stress has been experimentally studied and tested.10–14 Psychic stress has been compared with physical exercise, cigarette smoking and intake of drinks containing caffeine. 14 From the pathogenetic profile, the activation of the sympathetic15–16 and parasympathetic nervous systems 17 may be involved in both psychological and physical stress, and responsible for myocardial ischaemia. Some authors15,16,18 believe that the ischaemia induced by psychological factors is due to the sudden presentation of a stressful factor without any period of gradual ‘warm-up’, as in the case of physical exercise.
Experimental clinical assessments of the role of psychological stress factors in causing myocardial ischaemia mainly have a structure in common,19,20 shown below in simplified form:
Selection of patients with coronary sclerosis or positive history of previous episodes of myocardial infarct; Induction of a condition of psychic stress, or classification of several activities of daily living according to differing levels of stress intensity induced; Instrumental assessment of ischaemia or cardiopathological alterations induced.
Chronic stress-inducing events (e.g. situations at work, matrimonial unhappiness, etc.) have been examined, mainly in epidemiological studies, as possible factors causing cardiac disease. 21 In particular, such psychosocial factors as chronic stress exposure in the workplace, social isolation, low social support, emotional factors including depression, anxiety, anger and hostility have been related to the development of coronary heart disease.22–24
In the light of clinical observations made until now, it is clearly admitted in a general sense that the existence of psychically stressful events may indeed play a role in causing cardiac death. However, the extent of the potentially fatal stress factor giving rise to cardiac alterations and thence to death cannot be quantified, in view of the enormous number of factors involved. In other words it is difficult to demonstrate a clear-cut cause/effect relationship between psychic trauma and cardiopathological alterations. From the clinical viewpoint, in standardized conditions, problems of interpretation emerge and can be identified in the different negative psychic responses to the same event in two different people, in the impossibility of excluding the existence of interfering factors not reported by the patient or in the differing instrumental measurement technique. 1
It is even more difficult, if not impossible, to carry out such a task in the extremely variable conditions involved in the penal setting. The debate in penal cases regarding the existence of psychic trauma and its qualification is based on the above premises.
The aim of this study is to present three cases of death after psychic trauma, and to discuss the qualification of cause within the penal ambit of clearly identified ‘emotionally overwhelming factors’, according to a protocol prepared by the authors.
Materials and methods
The methodological approach to ascertainment and criterion-based assessment in each case involved the following phases: (1) examination of circumstantial evidence, clinical records and documentation; (2) autopsy; (3) ascertainment of cause of death; and (4) ascertainment of psychic trauma, and its coexisting relationship with the cause of death.
The protocol used by the authors to classify cases of sudden cardiac death due to arrhythmia in subjects with ischaemic cardiopathy involves three levels of actions or events responsible for mental reactions and thus potentially also responsible for causing acute psychic trauma (Table 1).
Actions or events classified by level of intensity

The first level includes situations of daily living which, although giving rise to emotional reactions, independent of the subject's personality, would never be qualified as psychic trauma. The second level involves situations in which psychic trauma may be described as including preexisting chronic psychic stress, mood/affect alterations, a subject's intense psychic response to the negative event, intense physical activity during the event (prolonged physical effort, with increased arterial pressure, frequency and contraction force, etc.). The third level includes situations of psychic trauma independent of the subject's pre-existing psychic state.
Results
The results and assessment of each case are discussed from the viewpoint of the causal connotation of psychic trauma.
Case 1
A severely obese, 46-year-old man rammed the car in front of him in a traffic jam. His car stopped at a point in the road where there was the risk of other cars ramming his. The man was taken to the emergency room, where he died of ventricular fibrillation. Autopsy revealed cardiomegaly, aortic insufficiency, slight atherosclerosis and myocardiosclerosis, with a previous myocardial infarct (Figure 1). The cause of death was ‘ventricular fibrillation in ischaemic cardiopathy and aortic insufficiency’.
Case 1 - postinfarct scar (in colour online)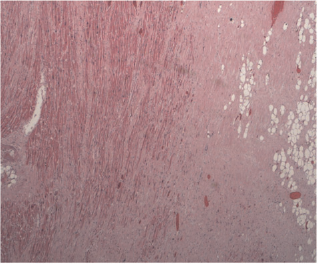
Case 2
During a quarrel for family reasons, a man of 72 felt violent chest pain, fell to the floor and died a few minutes later. The quarrel arose in a context of prolonged family disagreement and continual wrangling. Autopsy showed cardiomegaly, dilated left ventricle (Figure 2), slight atherosclerosis, diffuse myocardiosclerosis and undulating myocardial fibres. The cause of death was ascertained as ‘ventricular fibrillation due to acute postero-septal myocardial infarct, with hypertensive-dilatative cardiopathy’.
Case 2 - dilation of left ventricle (in colour online)
Case 3
A man of 48 suddenly died during a quarrel which had been going on for 15-20 minutes and involved physical violence. External examination prior to autopsy showed complex ecchymoses and abrasions, mainly around the eyes and cheekbones. Cardiac dissection revealed multivascular obstructive atherosclerosis, without occlusive thrombosis, and concentric hypertrophy of the left ventricle of hypertensive cardiopathic type. Histopathological examination of the median descending branch left coronary artery showed eccentric plaque, fibroatheromatous calcification, which had caused stenosis of about 85%, complicated by rupture of the capsula fibrosa, which was freely floating in the residual lumen, suspect platelet aggregates near the point of rupture, exit of most of the atheromatous pulp from the lipid core, with plaque haemorrhage (Figures 3 and 4). Histological examination of the antero-septal myocardium showed obvious interstitial oedema, intramyocardiac vessels filled with neutrophilic granulocytes, diapedesis and undulating myocardial fibres (Figure 5). Histopathological examination showed that the subject was already suffering from an acute myocardial infarct, which had commenced 4-6 hours previously. The cause of death was ascertained as ‘ventricular fibrillation due to acute antero-septal myocardial infarct, multivascular obstructive coronary atherosclerosis, rupture of the capsula fibrosa, plaque haemorrhage and subocclusion of the anterior descending coronary branch’.
Case 3 - antero-median descending branch of left coronary artery, with eccentric plaque, fibroatheromatous calcification, giving rise to stenosis of about 85%, complicated by rupture of capsula fibrosa, freely floating in residual lumen (in colour online)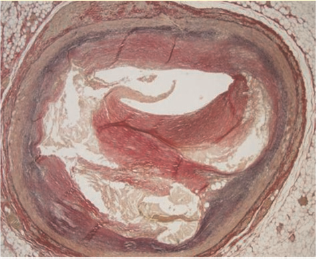
Case 3 - antero-median descending branch of left coronary artery, with eccentric plaque, complicated by rupture of capsula fibrosa, freely floating in residual lumen - histological section distal to the section of Figure 3 (in colour online)
Case 3 - interstitial oedema, intramyocardiac vessels filled with neutrophilic granulocytes, with diapedesis, and undulating myocardiac fibres (in colour online)
In these three cases, psychic trauma caused death, as deduced from the type of externally caused emotional insult, the subjects’ personal characteristics and the circumstances of the event causing death. Following the classification proposed by the authors, the event described in case 1 was of medium intensity. It was held that the event involved psychic trauma causing death, due to the severely negative psychic effect it may have had, for the deceased subject only, and in the circumstances of the accident. In particular, it was deemed that the subject's severe obesity, which meant that it was difficult if not impossible for him to abandon his car in a situation of potential danger, may have triggered a state of anxiety and fear sufficient to cause a fatal arrhythmic event.
The event causing death in case 2 was again of medium intensity. Again, a causal link - an acutely stressful event in the context of a state of chronic psychic stress (protracted family disagreement) - was ascertained to exist.
In case 3, the events indicated a level of maximum intensity (level 3, i.e. danger of personal injury, or grievous bodily harm) in a subject involved in a prolonged quarrel, with consequent significant cardiovascular alterations (increases in arterial pressure, frequency and cardiac contraction). In this case too, a causal link was deemed to exist.
Conclusions
Both acute and chronic stressful psychic factors may contribute to causing death in subjects suffering from ischaemic cardiopathy. 25 The etiopathogenetic complexity of the cardiopathological picture and interindividual differences of a highly negative psychic response to a triggering event mean that it is difficult to establish to what extent these factors contribute towards causing death, 14 especially in penal cases, since the two factors cannot be compared experimentally. However, although these causal elements can only be quantified approximately, some judicial questions arising regarding a death in a penal setting can be answered.
It should be noted that, in Italian law, a nexus is deemed to exist between the immediate cause of death and any preexisting and/or previously ascertained pathological condition that may have had a direct or indirect effect on the immediate cause of death - whatever the extent, great or small, of such a factor.
The methodological approach to ascertainment proposed here is one way of answering judicial questions in cases of cardiac death after psychic trauma in subjects suffering from ischaemic cardiopathy. In order to establish any coexisting cause of death, the extent of the event or action - with its possibly extremely negative psychic effect on the subject -must be assessed in relation to the gravity of the cardiopathological picture.
The authors propose a classification of psychic stress-inducing events according to the principle that the greater the objective severity of the situation or stimulus, the less the subjective cognitive assessment made by the individual involved. That is, in the case of extremely serious events, instant assessment of a threat to life leaves little margin for highly variable processes of cognitive evaluation, 1 with stereotypical attempts, for instance, at escape, search for shelter, etc. Faced with stimuli of objectively lesser severity, like most psychosocial stimuli, interindividual variability is greater, and reactions to stress tend to be more subjective. The context of the events with extreme psychic effects presented here are to be found in the DSM-IV (Diagnostic and Statistical Manual of Mental Disorders): 26 in particular, level 2 events occur in cases of adaptive disorders, and level 3 events may give rise to posttraumatic stress disorder. Our cases 1 and 2 are examples of the importance of contextualization of psychic stress within the subject's personality structure and the particular circumstances of how the event occurred. Case 3 exemplifies the existence of an emotional factor of such severity that psychic trauma ensued, independent of the subject's cognitive assessment.
With the aim of verifying or excluding the existence of a causal relationship between psychic trauma and death, the classification of emotional factors proposed here must be made at the same time as the cardiopathological picture, as severe cardiopathology may cause death autonomously, excluding the coexisting role of any accompanying psychic trauma.
In conclusion, although sometimes insuperable difficulties in assessment arise, in cases of presumed death after psychic trauma, careful methodological ascertainment is essential, with the double aim of verifying its ‘emotionally overwhelming factors’ as a penally important cause and of identifying the responsibility of third parties involved in the death event and its homicidal dynamics.