
Abstract
Understanding sexual dimorphism is very important in studies of human evolution and skeletal biology. The ability to determine sex from unknown skeletal remains is vital and methods to do this on the various bones of the human skeleton have been researched extensively especially in the studies related to forensic anthropology. The distinctive morphology and clear sexual dimorphism of the hip bone makes it an ideal bone for sex determination. Whereas the roles of the parameters of its posterior border (including the greater sciatic notch) are well established, those of the anterior border are not much explored. The present study was designed to establish the morphometric pattern of the anterior border of the hip bone and its role in sexual dimorphism. Material for the current investigation comprised 100 hip bones belonging to 50 cadavers ([M:F = 80:20] and [R:L = 50:50]) obtained from the Department of Anatomy, Government Medical College, Amritsar, Punjab, India. Sixteen parameters of the anterior border were taken and three indices were calculated. Eight parameters were significantly greater in males: (i) straight distance anterior superior iliac spine (ASIS)–symphyseal surface (SS); (ii) straight distance ASIS–pubic tubercle (PT); (iii) straight distance anterior inferior iliac spine (AIIS)–SS; (iv) straight distance AIIS–PT; (v) arch of anterior interspinous notch (ASIS–AIIS); (vi) arch between AIIS and ilio-pubic (IP); (vii) depth of notch between AIIS and IP; (viii) arch of anterior border (ASIS–SS). The results of the present study could be helpful in pronouncing an opinion, for a single specimen, about its origin in general terms or sex.
Introduction
It has long been customary among anatomists, anthropologists and forensic experts to judge the sex of skeletal material by non-metric observations. A number of recommended methods ranging from a simple physical examination to a detailed dissection procedure are in practice to determine sex in the living or the dead. Lately, sexual divergence has been based on actual measurements in different bones. 1 This minimizes the difficulties with quantification and interobserver bias.
As far as sex differences and sex determination are concerned, it has been universally accepted that the pelvic girdle or hip bone is the most important part of the skeleton 2,3 since the pelvic girdle has functional differences between the two sexes. The distinctive morphology and the clear sexual dimorphism of the hip bone make it of interest from anatomical, anthropological and forensic points of view. 4 Sex differences of the hip bones are present right from fetal life onwards. 5
A great amount of work has been done regarding the total size, the greater sciatic notch, the acetabulum, the obturator foramen and the pubis of the hip bone. 6–12 However, the role of the anterior border of the hip bone in sexual dimorphism remains largely unexplored because it does not make any contribution to the inlet or outlet of the true pelvis.
Aims and objectives
In the present study an attempt has been made to study the morphometric features of the anterior border of the hip bone in both sexes and to provide baseline data for the North Indian population.
Materials and methods
The material for the present study comprised 100 hip bones of known sex (male:female = 80:20) and side (right:left = 50:50), belonging to 40 male and 10 female individuals, obtained from the Department of Anatomy, Government Medical College, Amritsar, Punjab, India, during the period 2007–2009. The bones were undamaged and showed no pathological changes.
For each of the hip bones, the 16 variables confined to the anterior border were measured (see Table 1) (Figure 1). For measuring these variables the following instruments were used:
Vernier callipers by the company Aerospace with a least count of 0.02 mm; Ruler with a least count of 1 mm; Doctor's tape. Showing various parameters of the anterior border of the hip bone: A, anterior superior iliac spine; B, anterior inferior iliac spine; C, ilio-pubic eminence; D, pubic tubercle; E, superior end of the symphyseal surface; x, depth of the notch between ASIS and AIIS; y, depth of the notch between AIIS and IP; and z, depth of the notch between ASIS and SS Showing different measurements of the anterior border of the hip bone and landmarks for their measurements ASIS, most prominent point on anterior superior iliac spine; AIIS, most prominent point on anterior inferior iliac spine; IP, most prominent point on ilio-pubic eminence; PT, most prominent point on pubic tubercle; SS, most prominent point on superior end of symphyseal surface

The linear measurements were taken with the help of sliding Vernier callipers by keeping the calliper ends between the designated points (see Figure 3).
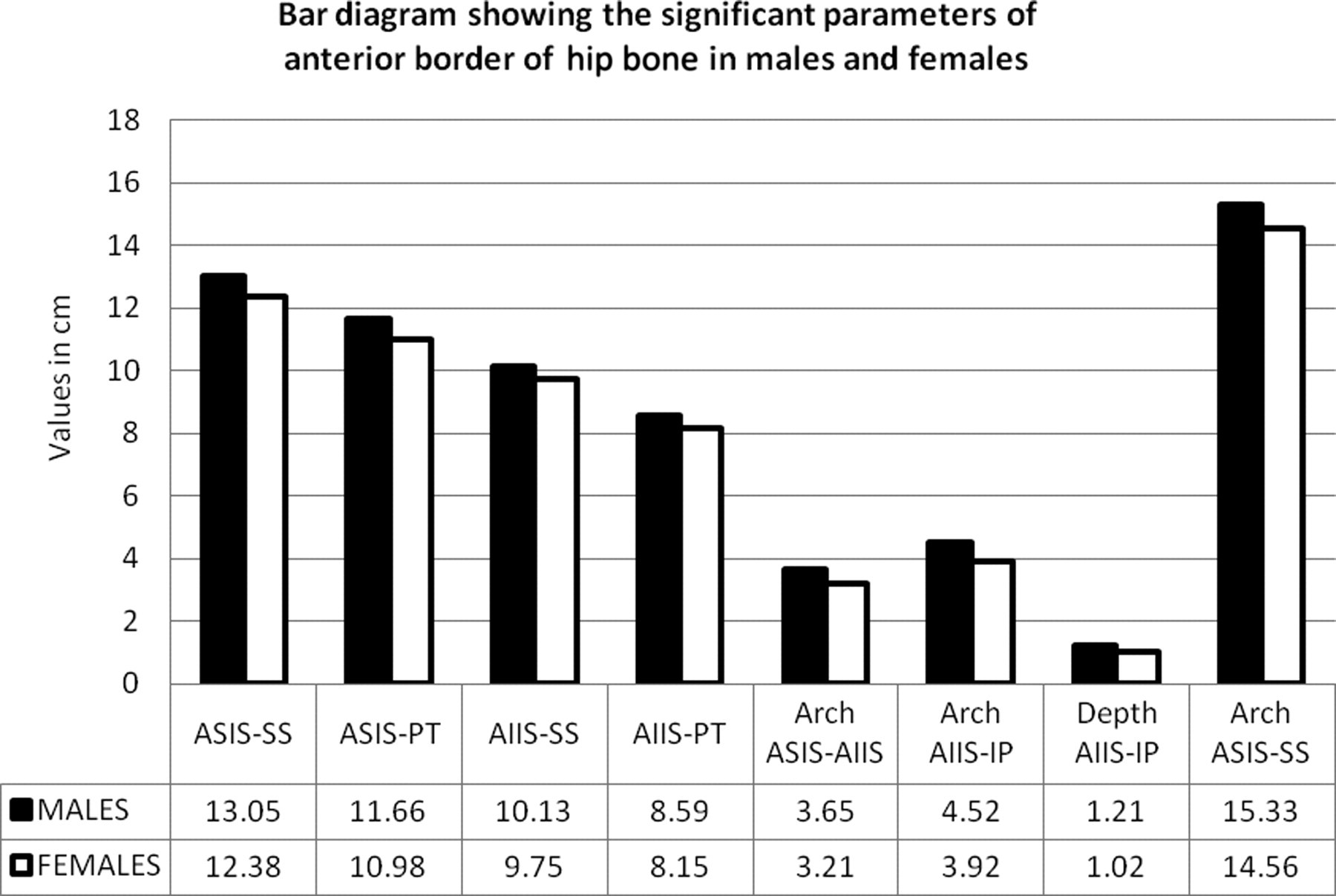
Bar diagram showing the significant parameters of the anterior border of the hip bone in males and females

Method to measure distance from the anterior superior iliac spine to the anterior inferior iliac spine (ASIS-AIIS)
To measure the curved distances, doctor's tape and a ruler were used, e.g. to measure the anterior interspinous notch (arch anterior superior iliac spine [ASIS]–anterior inferior iliac spine [AIIS]), doctor's tape was plastered against the anterior interspinous notch. Then the tape was marked at the designated points (i.e. ASIS and AIIS), lifted off the bone and measured along the scale of the ruler. Other arches were measured in a similar way (see Figure 4).

Method to measure the arch of the anterior interspinous notch
The various depths were also recorded with the help of Vernier callipers, e.g. the depth of the anterior interspinous notch (depth of notch ASIS–AIIS) was taken by keeping a steel bar at the designated points (i.e. ASIS and AIIS) and measuring the perpendicular distance between the bar and the deepest point of the notch with the help of Vernier callipers. Other depths were measured in a similar way (see Figure 5).

Method to measure the depth of the anterior interspinous notch
Also three indices pertaining to the anterior border of the hip bone were calculated:


Observations and discussion
Table 2 compares the mean values and range of different measurements pertaining to the anterior border of the hip bones as observed in the present study and their comparison with the only other study conducted on these measurements by Pellico and Camacho 4 in the Spanish population. It is evident from this table that in the present study, all these measurements are longer in the males except for the depth of the anterior border (Sr. No. 16) which is equal in both the sexes (2.82 cm). However, out of the total of 16, in eight measurements (Sr. No.s 1, 2, 5, 6, 10, 12, 13 and 15), these differences were statistically significant (P value <0.05) (see Figure 2).
Comparison of parameters of the anterior border of the hip bone with respect to sex
ASIS, most prominent point on anterior superior iliac spine; AIIS, most prominent point on anterior inferior iliac spine; IP, most prominent point on ilio-pubic eminence; PT, most prominent point on pubic tubercle; SS, most prominent point on superior end of symphyseal surface; CI, confidence interval
Interpretation P value <0.05 = statistically significant, >0.05 = statistically insignificant
The values marked as bold were found to be significant by Pellico and Camacho 4
*P value calculated by Independent t-test
In contrast, in the only other study conducted on these measurements by Pellico and Camacho
4
in the Spanish population, the following measurements were longer in females:
Distance ASIS–AIIS (Sr. No. 4) Straight distance IP–symphyseal surface (SS) (Sr. No. 8) Arch of the anterior interspinous notch (ASIS–AIIS) (Sr. No. 10) Length of the border between IP and SS (Sr. No. 14) Depth of the anterior border (ASIS–SS) (Sr. No. 16)
Also they found only four measurements (Sr. No.s 2, 6, 7 and 12) to be statistically significantly longer in males, out of which three (Sr. No.s 2, 6 and 12) overlap with the present study.
A higher value in males as seen in the present study is easily explainable on the basis of male robusticity and the fact that the anterior border of the hip bone does not form part of the true pelvis, which is supposed to be wider in females for obvious reasons. On the other hand, higher values of some measurements in Spanish females (vide supra) may be attributed to differences in ancestry.
If we compare our male and female values from Table 2 with those of Pellico and Camacho 4 separately, it is seen that most of our values are smaller than those in the Pellico and Camacho 4 study, except for the straight distance AIIS–IP, the depth of the anterior interspinous notch (ASIS–AIIS) and the depth of the notch between AIIS and IP (Sr. No.s 7, 11 and 13), which are longer in both sexes in the present study, while the straight distance IP–pubic tubercle (PT; Sr. No. 9) is the same in both sexes in both the studies. Apart from this, the straight distance IP–SS (Sr. No. 8), the arch between AIIS and IP (Sr. No. 12) and the length of the border between IP and SS (Sr. No. 14) are longer in our males and the straight distance AIIS–PT (Sr. No. 6) is longer in our females.
From all these results, it can be interpreted that the notch between the AIIS and IP is both wider (Sr. No. 7) and deeper (Sr. No. 13) in the North Indian population in the present study as compared with the Spanish population. But the notch between ASIS and AIIS is wider in the Spanish population (Sr. No. 4) while it is deeper in the Indian population (Sr. No. 11). The other measurements show inconclusive results.
A comparison with respect to sex and side in the two studies (Table 3) shows that while Pellico and Camacho 4 could not find any significant difference between the two sides in both sexes, the same was true for only females in the present study. In males, statistically significant differences were seen in the straight distance AIIS–PT (Sr. No. 6), the arch between AIIS and IP (Sr. No. 12) and the arch of the border between IP and SS (Sr. No. 14) (vide supra).
Comparison of parameters of the anterior border of the hip bone with respect to sex and side
ASIS, most prominent point on anterior superior iliac spine; AIIS, most prominent point on anterior inferior iliac spine; IP, most prominent point on ilio-pubic eminence; PT, most prominent point on pubic tubercle; SS, most prominent point on superior end of symphyseal surface; CI, confidence interval
The values marked as bold were found to be more on the left side
*P value calculated by paired t-test
Interpretation P value <0.05 = statistically significant**, >0.05 = statistically insignificant
Index I – Index of widening of the anterior border
As can be seen in Table 2, Index I was deeper in females in both the ancestries but the mean difference was insignificant in both (P value in present study = 0.131). The difference in the values of the two studies is most likely due to ancestral influences.
Further, on comparing the index on two sides, it was slightly deeper towards the left side in both the sexes. But the difference was statistically insignificant (P value = 0.961 and 0.260 in males and females, respectively).
Index II – Index of widening of the anterior interspinous notch
Looking at Table 2, it can be clearly stated that this index is highly under the influence of ancestral variation as the values in the two ancestries are not comparable. This may be due to the fact that the anterior interspinous notch is deeper in the Indian population but wider in the Spanish population, thus increasing the value of Index II in the former and decreasing the same in the latter. If compared between the two sexes, while Pellico and Camacho (Spanish) 4 calculated Index II to be higher in males, the reverse was true in the present study. However, the results were statistically insignificant in both the studies (P value in present study = 0.268).
On comparing the index on two sides (Table 3), it was higher towards the left side in both the sexes, the difference being statistically insignificant in males (P value = 0.071), but highly significant in females (P value = 0.005).
Index III – Index of widening of the notch between the anterior inferior iliac spine and the IP eminence
As can be seen in Table 2, while Pellico and Camacho (Spanish) 4 found Index III to be higher in females, the reverse was true in the present study which also may be due to ancestral variation. The results were statistically insignificant in both the studies (P value in present study = 0.059).
On comparing the index on two sides, it was deeper towards the left side in both the sexes, the difference being only statistically significant in males (P value = 0.032 in males and 0.238 in females).
The different results in the two studies may be undoubtedly attributed to the ancestral influences as both the studies are based on entirely different sets of populations, i.e. Spanish and North Indians (present study).
Summary and conclusions
Among the 16 morphometric measurements and three indices pertaining to the anterior border of the hip bone, eight were found to be significantly longer in males. These were (i) straight distance ASIS–SS, (ii) straight distance ASIS–PT, (iii) straight distance AIIS–SS, (iv) straight distance AIIS–PT, (v) arch of the anterior interspinous notch (ASIS–AIIS), (vi) arch between AIIS and IP, (vii) depth of the notch between AIIS and IP and (viii) arch of the anterior border (ASIS–SS). This may be attributed to the male robusticity and to the fact that the anterior border of the hip bone does not form a part of the true pelvis which is supposed to be wider in females for obvious reasons.
On the other hand, when the two sides were compared, the differences were statistically insignificant in all the morphometric measurements and indices in females, while in males the straight distance AIIS–PT (Sr. No. 6) and the arch between AIIS and IP (Sr. No. 12) were significantly longer on the right side and the arch between IP and SS (Sr. No. 14) was significantly longer on the left side.
Thus, it can be put forward that even the anterior border of the hip bone may serve as an important indicator for sexual dimorphism. However, owing to the scanty literature available for comparison, more elaborate studies and baseline data are required for different populations.