
Abstract
Objectives
The study aimed to assess the extent of knowledge of the Mental Capacity Act (MCA) (2005) among new recruits to a National Health Service (NHS) Trust.
Design
Respondents were assessed before and after a brief training experience.
Setting
Data were collected while respondents attended their mandatory Trust induction training.
Main outcome measure
Assessment was by means of a 16-item true–false questionnaire.
Results
While respondents' knowledge appeared reasonably good for some important features of the MCA, these results may have been exaggerated by a strong tendency to respond ‘true’, which persisted despite instructions intended to counteract it. Some significant areas of ignorance were also identified. Scores showed a small but significant improvement when participants were reassessed following a 10-minute talk on the MCA; the improvements were specific to certain items that were included in the training presentation. There were no significant differences in performance between non-clinical staff, naïve clinicians and clinicians who reported having previously received training on the MCA.
Conclusions
Knowledge of the MCA among newly appointed NHS staff is patchy, with some strengths but also significant weaknesses. The results demonstrate a benefit of the brief training experience, but also question how much information is retained by participants in MCA training.
Introduction
The Mental Capacity Act 1 (MCA) was implemented in 2007. The MCA requires all professionals to assess capacity and make proxy decisions where capacity is lacking; they may if necessary commission a specialist assessment, but retain individual responsibility for the decisions they take. The MCA creates a legal presumption in favour of capacity, provides a functional definition of capacity (‘the ability to understand, retain and evaluate the relevant information, and communicate the decision’), endorses the right to make ‘unwise’ decisions and stipulates that people may not be assessed as lacking capacity until all reasonable steps to support them have proved unsuccessful. Proxy decisions on behalf of persons who lack capacity must be made in their best interests, after consulting ‘anyone engaged in caring for the person or interested in his welfare’; and where there are no family or friends to be consulted, an Independent Mental Capacity Advocate (IMCA) must be involved in decisions about serious medical treatment or changes of long-term accommodation. Some topics fall outside the MCA, including decisions about personal relationships.
Guidance on the MCA has been produced by the British Medical Association, 2 the General Medical Council, 3 the British Psychological Society 4 and the Department of Constitutional Affairs. 5,6 However, a study by the Mental Health Foundation conducted shortly before the Act was implemented reported that there was widespread confusion about the meaning of mental capacity, the criteria for assessment and the purpose of assessment. 7 A number of other studies, conducted both before and after the implementation of the MCA, have reported a generally poor state of knowledge regarding consent to medical treatment, and other mental capacity issues, among doctors and other health-care workers, 8–14 though two recent studies, of consultant old age psychiatrists 15 and of specialist staff in palliative and neurological care settings, 16 were more encouraging.
One important feature of the MCA is that while some mental capacity issues are of such complexity that a specialist assessment may be needed, any health or social care worker could be in a situation where they are dealing with a member of the public whose capacity is uncertain, and where it would be necessary for them to assess capacity and, potentially, to make a decision in the person's best interests if capacity is assessed as lacking. It is therefore important to know how well mental capacity issues are understood among National Health Service (NHS) and social care staff generally, not simply in specialist services. Furthermore, the importance of training on the MCA for NHS and social care staff has been highlighted, 7,17 and all NHS Trusts and Local Authorities have been provided with funding to deliver such training. However, the effectiveness of MCA training is unknown.
The present study was part of a larger project exploring the extent to which NHS and social care staff understand the requirements of the MCA. The participants in this study were recruited from among newly appointed staff attending their Trust induction training. As there is turnover and recruitment in all sectors of the NHS, this approaches a representative sample of NHS employees, albeit confined to newly appointed staff. We wished to establish what general knowledge about the MCA new appointees were bringing to the Trust, and whether their knowledge increased as a result of the very brief presentation on the MCA that they received as part of their induction training.
Methods
Participants and setting
The participants were new recruits to the Trust attending their mandatory induction training. Questionnaires were distributed at four induction sessions, involving a total of approximately 150 participants. Respondents included both clinicians and non-clinicians. The clinicians spanned the full range of seniority, from health-care assistants to medical consultants; however, there were too few clinicians in any category to attempt to analyse the data by subgroup. A total of 116 valid questionnaires were returned (a response rate of approximately 75%); a further 17 questionnaires were returned that could not be analysed either because they were incomplete or because the pretraining questionnaire had been completed but the post-training questionnaire had not.
Questionnaire
The questionnaire consisted of 16 true/false statements, half true and half false (Table 1). It was created in a series of meetings involving researchers, clinical psychologists, advocates and Trust MCA implementation leads. The version of the questionnaire used here was an expansion of a shorter (10-item) questionnaire used in an earlier study. 14 The expansion to 16 items was intended to equalize the number of true and false statements (which in the 10-item version were mainly ‘true’), and to provide a comprehensive coverage of those aspects of the MCA that are relevant to health services. The questionnaire was not designed specifically for this study and includes eight items that were covered explicitly, albeit very briefly, in the presentation and eight items that were not. The included items are shown in bold type in Table 1.
Questionnaire and the proportion of participants responding correctly before and after the training session
The T/F column indicates whether the statement is True or False. The right-most column shows significant changes from before to after training (McNemar tests); the entry in parentheses represents an item where performance became significantly worse. Items in bold type are those that were addressed in the training session, as identified from a copy of the PowerPoint presentation
Examination of the data from the first two cohorts of participants (n = 57) revealed a strong bias towards ‘true’ responses. In an (ultimately unsuccessful) attempt to counteract this bias, a prompt was added for the second two cohorts (n = 59) stating that: ‘It may help you to know that approximately half of the statements are true and approximately half are false’.
Procedure
The induction training programme included, among many other presentations, a 10-minute presentation by the Trust MCA implementation lead. On arrival, participants were issued with a pack consisting of an information sheet and some demographic questions, and two copies of the questionnaire, one for immediate completion and the other for completion at the end of the day.
Statistical analysis
Total scores were analysed by analysis of variance or t-tests. Performance on individual items was analysed by χ 2 or McNemar tests.
Results
The effect of the prompt to make ‘roughly equal’ true and false responses was examined separately for total questionnaire scores and for true and false statements, and for questionnaires completed before and after training and for the pre–post difference. All nine of these comparisons were non-significant (max t[114] = 1.05). Therefore, this factor was ignored in subsequent analyses. At the level of individual questions, one of the 32 comparisons (i.e. 16 questions, before and after) was significant at the P < 0.05 level, which would be expected by chance. However, responses to one question (Q2, post-training) differed between the prompt and no-prompt groups at the P < 0.001 level; this result is considered further below.
There was a strong tendency for participants to respond ‘true’, even when prompted that half of the statements were false (Figure 1). Overall, correct answers were slightly above the chance level (8) and there was a small but significant improvement with training (from mean ± SEM 8.62 ± 0.17 to 9.83 ± 0.16 correct responses). Analysis of variance (Anova) confirmed a more accurate response to true statements than to false statements (F[1,115] = 417.1, P < 0.001) and that performance improved significantly following training (F[1,115] = 43.3, P < 0.001), with no significant interaction between these two factors (F[1,105] = 1.76, NS).
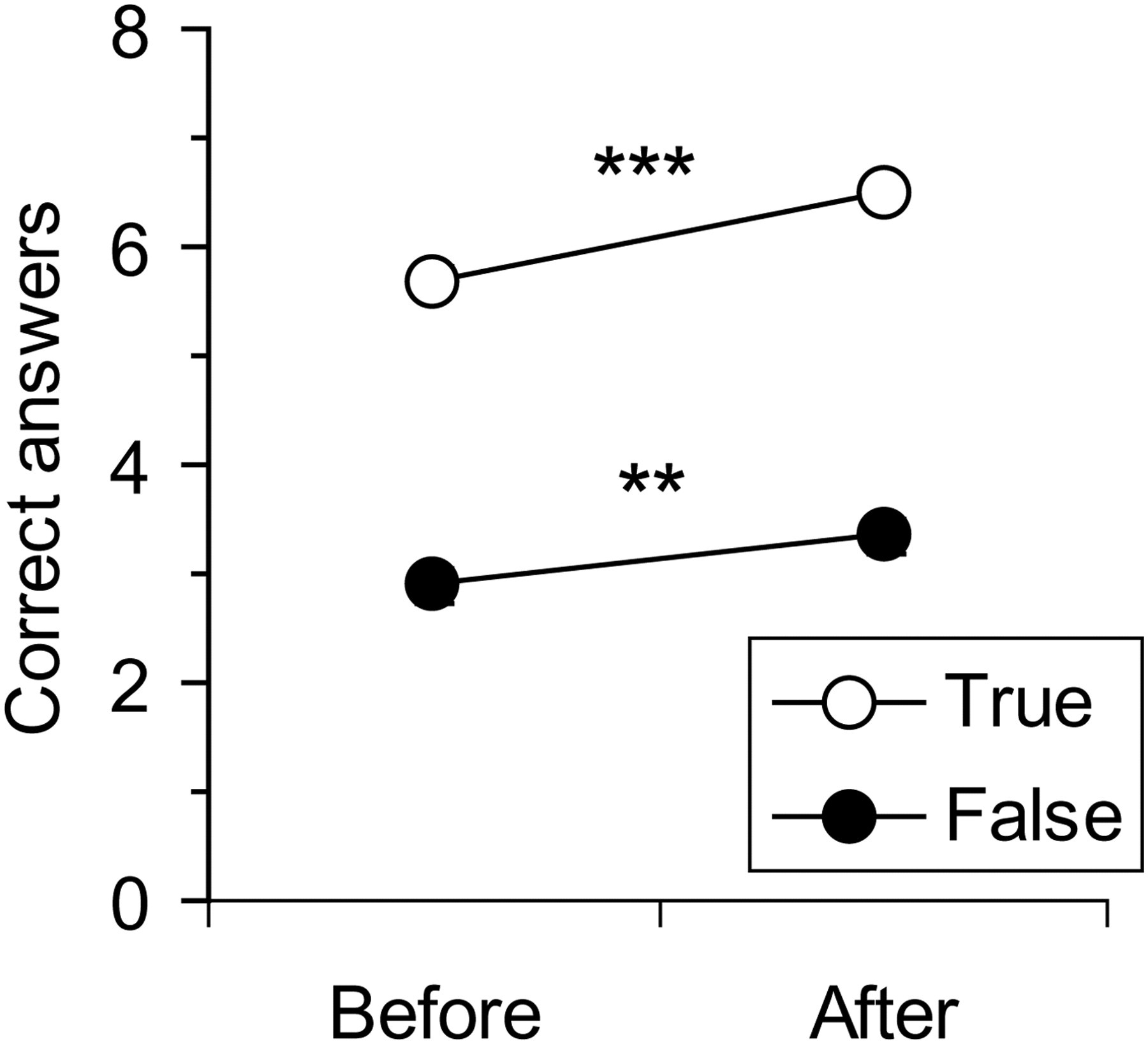
Correct true and false responses before and after training. Values are means; standard errors are contained within the symbol. **P < 0.01, ***P < 0.001 for before–after comparison
Before the training, items that were included in the training session were answered better than those that were not (Figure 2), but this reflects simply that 6/8 of the included items were ‘true’ while 6/8 of the excluded items were ‘false’. Anova of these scores showed a significant question type by training interaction (F[1,115] = 418.2), reflecting the fact that, as expected, participants' scores improved only on the items that were covered in the presentation.
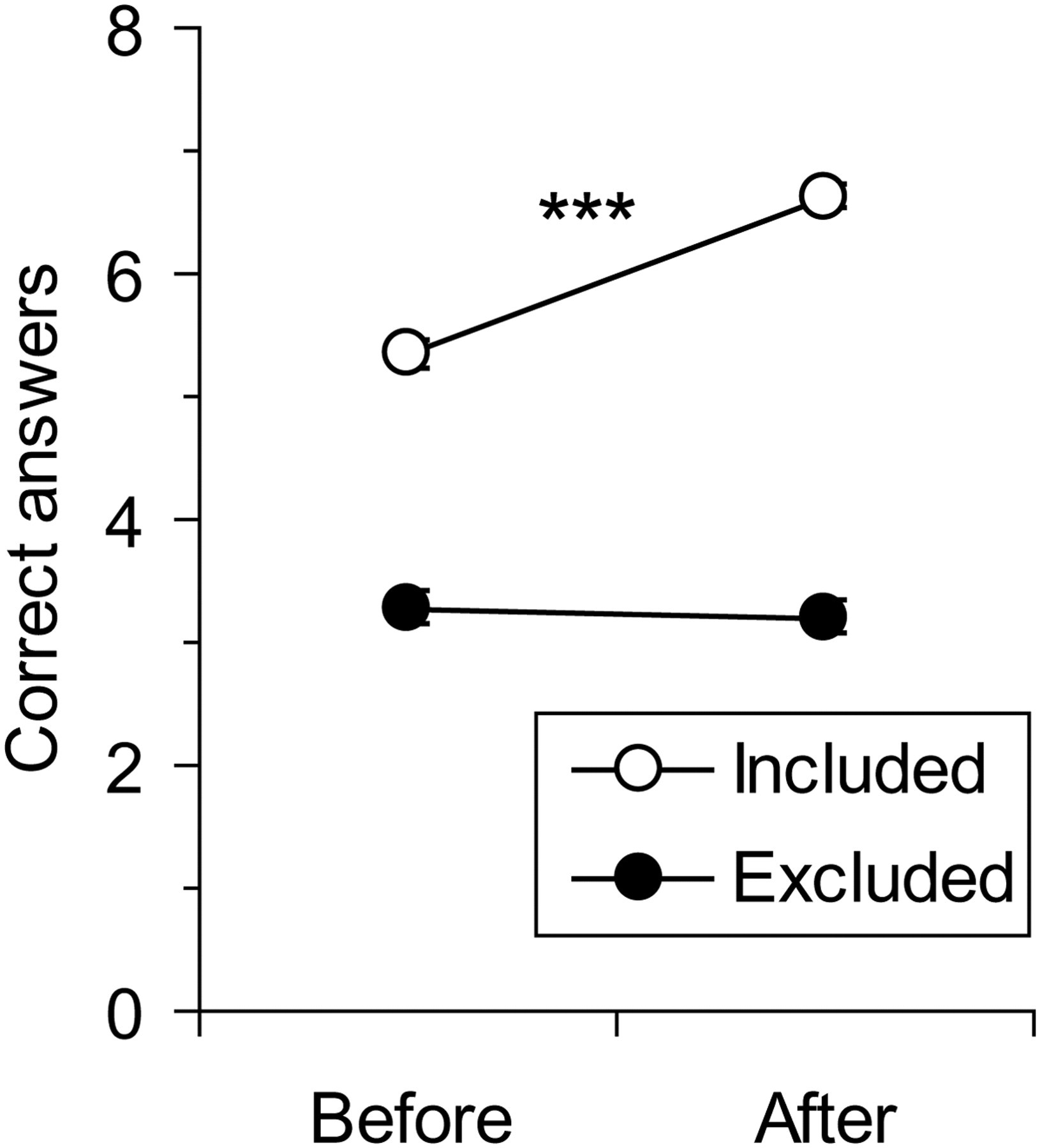
Correct responses before and after training for items included in or excluded from the presentation. The difference in pretraining scores reflects the fact that 6/8 of the ‘included’ items were ‘true’, while 6/8 of the excluded items were ‘false’. Values are means; standard errors are contained within the symbol. ***P < 0.001 for before–after comparison
There was no significant difference between clinicians (n = 64) and non-clinicians (n = 52) on any of the nine comparisons outlined above (max t[114] = 1.45). Neither was there any significant difference, between those clinicians who reported having received prior training (n = 24) and those who did not (n = 40) (max t[62] = 1.29), though trained clinicians performed slightly better on all pre and post measures. There were also no individual items on which trained and untrained clinicians differed significantly (max χ 2 = 1.93).
Prior to the brief training experience, participants displayed a relatively good understanding (>75% correct responses) on six questions (five of them ‘true’ statements); the maximum rate of correct answers on the other 10 questions was only 56% (Table 1). The questions that were answered well related to: the requirement not to infer incapacity on the basis of unwise decisions (Q3) or personal characteristics (Q14), the desirability of consultation (Q4), the requirement to take steps to support capacity (Q6), the best interests principle (Q9) and what information to consider when assessing best interests (Q13).
When re-tested following the training session, there were significant improvements on three questions (one true, two false) (Table 1). These related to the non-specialist nature of capacity decisions (Q2), the limited role of the IMCA (Q8), and the requirement to choose a less restrictive option (Q12). On Q2, the improvement following training was significantly greater (P < 0.001) in the non-prompted group (56% increase) than in the prompted group (22% increase). While the correct response rate on Q8 remained relatively low despite the increases, the final scores on Q2 and Q12 were relatively high. However, on Q16, relating to Deprivation of Liberty Safeguards (which were mentioned in the presentation but not discussed), there was a small but significant deterioration in performance following training.
Discussion
Principal findings
The results give grounds for both optimism and concern. Participants showed a relatively good understanding of some aspects of the MCA, and there were discernible improvements following a very brief training experience. On the other hand, significant limitations on participants' understanding of the MCA were discernible both before and after the training event. These issues are discussed further below.
Strengths and weaknesses of the study
The main strength of the study is that it had an adequate sample size and a high response rate. The main weaknesses of the study are that it took place within a single NHS Trust, and participants were found to have a strong bias to respond ‘true’, even when prompted that half of the statements were false.
Interpretation of the results
Participants were told that they would be required to attend further mandatory training on the MCA (and on Deprivation of Liberty Safeguards), so there was no expectation that the information presented during Trust's very busy induction programme would meet all of their training needs in this area: indeed, the experience could be viewed more as a taster than a serious training event. Nevertheless, this very brief (10 minutes) presentation did produce a significant, albeit small (14%), increase in the number of correct responses. We were able to identify that the improvement was primarily in the answers to two of the 16 questions (Q2 and Q12).
After the training session, high rates of correct responses (>85%) were seen on six questions that include some of the most important features of the MCA, such as not making assumptions based on unwise decisions (Q3) or personal characteristics (Q14), supporting capacity (Q6), and the principles of best interests (Q9) and less restrictive options (Q12). In the case of the less restrictive option (Q12), this was something that many participants had clearly learned from their training. However, the six well-answered items were all true statements, and despite our best efforts, respondents displayed a strong response bias that may well have inflated correct response rates for ‘true’ items. Therefore, respondents' actual knowledge of the MCA may be significantly lower than it appears from this survey. The tendency for respondents to endorse statements about the MCA should be taken into account in designing studies in this area.
The other lesson that people clearly learned from the training was that capacity assessment is not the preserve of specialists (Q2). The figure in Table 1 of 75% correct responses for this question actually represents 93% of the first cohort, but only 53% of participants who were prompted to make more ‘false’ responses, a curious finding considering that ‘false’ is the correct answer to this question. It may be that this anomaly reflects the fact that the question came very near the beginning of the questionnaire and respondents were seeking to equalize their responses (after most of them had given incorrect ‘true’ answers to Q1). However, there was no evidence of such strategic thinking later in the questionnaire, as the proportion of ‘true’ and ‘false’ responses did not differ between the two subgroups on other questions.
Set against the relatively high scores in some areas, for the majority of questions, rates of correct responding were unacceptably low. Considering the types of issues that might face a NHS employee, four such questions stand out. First, fewer than 30% of respondents recognized that the outcome of a decision has no relevance to assessment of the mental capacity to make it (Q5). Whereas outcome has been considered in the past to bear on capacity, the MCA explicitly rejects this position: ‘What matters is (the) ability to carry out the processes involved in making the decision – and not the outcome’ (MCA Code of Practice, s.4.2). Second, participants showed a relatively poor understanding of the two-stage test for mental capacity (Q7: 66%), suggesting that they might overlook the MCA requirement to demonstrate ‘an impairment of or disturbance in the functioning of mind or brain’ before proceeding to a capacity assessment. Third, even taking into account that performance improved as a result of the training, fewer than 50% of respondents demonstrated an understanding of the role of the IMCA service (Q8), which is only required to be involved in relation to certain specific best-interest decisions relating to serious medical treatment and long-term housing. Finally, only 25% of respondents understood that for the vast majority of best-interest decisions there is a single decision-maker, whom others advise (Q15). It is perhaps less of a concern for the time being that on Q16 (Deprivation of Liberty Safeguards) respondents were less clear about the answer after training than before. While dealing with an important issue, this question reflects very recent legislation (the 2007 Mental Health Act 18 ) that is still relatively unfamiliar to most NHS employees. The topic was addressed very briefly in the presentation, and staff were reminded that they would be required to attend further mandatory training.
Implications for policy and future research
Perhaps the most disconcerting finding was that there were no differences between the three cohorts of respondents: non-clinical staff, naïve clinical staff and clinical staff who reported having received prior training on the MCA. The fact that clinical staff, who meet patients and therefore encounter potential mental capacity issues in the course of their day to day work, were no more knowledgeable than non-clinical staff, who on the whole do not, suggests that the relatively high level of knowledge in many areas reflects information about the MCA that has diffused out into the general culture, rather than information that has been acquired specifically for its relevance to the respondent's work. And against this background, whatever training it was that some clinicians had previously experienced, it appears not to have provided any discernible benefit. The study involved a relatively small sample size and a single NHS Trust, but nevertheless, the results raise cause for concern. In a comparable study of specialist learning disability professionals, it was similarly noted that knowledge of mental capacity issues appeared to be no greater in the majority of respondents who had undergone MCA training than in the minority who had not. 14 Similar failures of training have been noted in other areas. 19 In the present study no details were collected of respondents' earlier training experiences. Considering that in excess of £12m has been invested in MCA training for health and social care staff, 20 it will be important to evaluate the impact of defined training experiences. A study of this kind is currently in progress.
DECLARATIONS
There are no conflicts of interest. The study was supported by a small grant from the Welsh Office for Research and Development in Health and Social Care (WORD). It was deemed by the Local Research Ethics Committee not to need ethical approval; the study is sponsored by ABMU Health Board and guaranteed by PW. The study was designed by PW and SD and implemented by JB and GL.