
Abstract
Background
Previous studies of death during law enforcement restraint have focused on lying restraint positions; this study extends this work to seated restraint positions.
Methods
Lung function in a standing control position was compared with lung function in seated positions using 40 volunteers.

Seated, leaning forward, restraint applied

Effect of position on lung function (forced vital capacity – FVC). Notes: position one: standing control (=100%); position two: seated control; position three: seated, leaned forward, no restraint; position four: seated, leaned forward, restrained

Effect of position on lung function (forced expiratory volume in one second – FEV1). Notes: position one: standing control (=100%); position two: seated control; position three: seated, leaned forward, no restraint; position four: seated, leaned forward, restrained
Results
No significant reduction in lung function was detected in an upright seated position. When participants were leant forward while seated, significant reductions in lung function occurred. The application of restraint holds in the seated, leant forward position resulted in a non-significant further reduction in lung function. Reductions in lung function were greater in those participants with higher body mass index (BMI).
Conclusions
Seated restraint positions with the person leant forward may increase the risk of harm or death during prolonged restraint. The risk will be further increased where the person exhibits higher BMI.
Introduction
Manual restraint of violent or resistive individuals may be required in settings such as law enforcement, prisons or mental health services. In a small number of cases such restraint is accompanied by sudden death, either during or immediately following the restraint. 1–3 Although such deaths are numerically infrequent, there may be a substantial degree of controversy, protest and concern that further justifies efforts to minimize the risks involved in restraint. Additionally, those who must investigate such deaths will require the best possible evidence to inform their investigations and conclusions.
Early work on death associated with law enforcement restraint focused on neck holds. 4,5 However, subsequent publications identified cases in which no overtly dangerous restraint technique had been applied and no injury, sufficient to explain death, was identified at postmortem. 3,6 Reay 7 proposed the concept of ‘positional asphyxia’ to explain such deaths, suggesting that body position limits movement of the ribs and diaphragm to such a degree that asphyxia results.
Case reports 3,6,8 and early laboratory work 9 appeared to support this view. However, subsequent studies failed to replicate the laboratory findings 10–12 and researchers expressed doubt that the levels of restriction of lung function demonstrated in their laboratory studies were sufficient to cause death. 10
One team of researchers report studies investigating restraint in prone positions; 10 restraint supplemented by the use of Oleoresin Capsicum spray (‘pepper spray’); 13 restraint supplemented by weight applied to the subject during restraint; 14 and restraint supplemented by physical exertion. 15 In each case, lung function in restraint was compared with a control position. The authors consistently report reductions of lung function in prone restraint positions, but suggest that the reductions are not sufficient to be fatal.
Parkes and Carson 16 report a study of lung function during restraint. Participants restrained flat on the floor, prone or supine, showed non-significant reductions in forced vital capacity (FVC) and forced expiratory volume (FEV1). However, participants restrained prone on the floor in positions that included body weight of restraining persons placed on them and/or a flexed body showed significant decrease in lung function. The authors conclude that some, but not all, prone positions cause significant reductions in lung function.
Much of the work noted above focuses on prone restraint and indeed frequently on the hobble prone restraint prone position (‘hogtie’). However, it is clear that deaths have occurred in other positions. 17 This study was carried out with the intention of applying previously used methodology to seated restraint positions, including examination of the effects of body size and leaning forward during seated restraint.
Materials and methods
Participants
Forty university students. Participants were recruited in two cohorts of 20, cohort 1 having a body mass index (BMI) less than 25 and cohort 2 having a BMI greater than 25. Descriptive data for the two cohorts of participants, BMI < 25 and BMI > 25, are given in Table 1.
Characteristics of the two cohorts based on BMI
Number of participants was set by a power calculation, based on results from a previous study using the same methodology. 16 Twenty participants was calculated to be sufficient to provide a 0.8 probability of detecting a clinically significant (10%) reduction in lung function.
Exclusion criteria were self-declaration of relevant pre-existing ill health, use of prescribed or illicit drugs and a BMI greater than 35. A health declaration was obtained from each participant prior to participation.
Ethical issues
The study was approved by the Coventry University research ethics review procedure. Participants were provided with relevant information verbally and in writing. Written consent was obtained prior to participation.
Conduct of the study
The study compared lung function in four positions:
Position one: Standing control position.
Position two: Seated control position (seated, upright, no restraint holds).
Position three: Seated, leaning forward (seated, participant instructed to lean forward to the furthest point possible without active effort).
Position four: Seated, leaning forward, restraint applied (seated, participant instructed to lean forward to the furthest point possible without active effort. Arms restrained using a double figure of four arm hold. Restraining staff applied no force at rest but resisted the participants' motion during the respiratory test manoeuvre).
The study employed a repeated measures design with each participant providing measurements of lung function in each of the four positions. The order of restraint/control positions was randomized via a Latin square method.
On arrival at the laboratory height, weight and seated waist measurement of each participant were recorded. BMI was calculated. Lung function was measured via a Powerlab data acquisition system running the Chart version 4 software with the spirometry extension (AD Instruments Ltd, Chalgrove, UK). The inspired and expired flow rate was measured via an MTL1000L respiratory flow head (pneumotachograph), connected to a Spirometer Pod, a Powerlab 2/20 and a Windows compatible computer (AD Instruments Ltd). A rubber mouthpiece connected to the pneumotachograph was used to ensure a good seal and nose-clips were worn during spirometry. Flow was integrated by the software to measure inspired and expired volume. The flow head was calibrated across the analytical range using known flows of compressed gas measured via a rotameter (Kobold, UK). All participants had quiet breathing at rest measured initially in a standing position to allow for habituation to the equipment. Maximum forced inspirations and expirations were performed initially in the standing position as practice manoeuvres. All participants were verbally encouraged during spirometry in all positions to inhale and exhale maximally, as the measurements are effort-dependent. Each measurement was based on three respiratory manoeuvres, with a period of quiet breathing of approximately five minutes between each attempt, in each position.
Oxygen saturation was not measured as a variable in this study since previous studies had demonstrated that oxygen saturation does not show significant changes during laboratory simulation of restraint. 10,12
The recorded data were subsequently analysed using the Chart software with the Spirometry Extension. FEV1 in the first second (FEV1), FVC, FEV1/FVC ratio, peak expiratory flow and peak inspiratory flow were calculated.
Statistical analysis
Statistical analysis was performed using the SPSS version 16 software. Data are expressed as mean ± 1 standard deviation.
Results
See Table 2.
Effect of position/BMI on lung function
Results expressed as percentage of position one (standing control)
(position one = 100%). All results are mean (sd).
Results in bold are statistically significant, P < 0.01
Effect of BMI/seated waist measurement on restriction of lung function
The effect of body size characteristics on the reduction in lung function in position four was analysed using linear regression. There was a significant relationship between the decrease in FVC in position four and BMI for the whole group (r = 0.634, P < 0.05; Figure 4). There was also a significant relationship between the decrease in FVC in position four and seated waist girth (r = 0.480; P < 0.05; Figure 5).
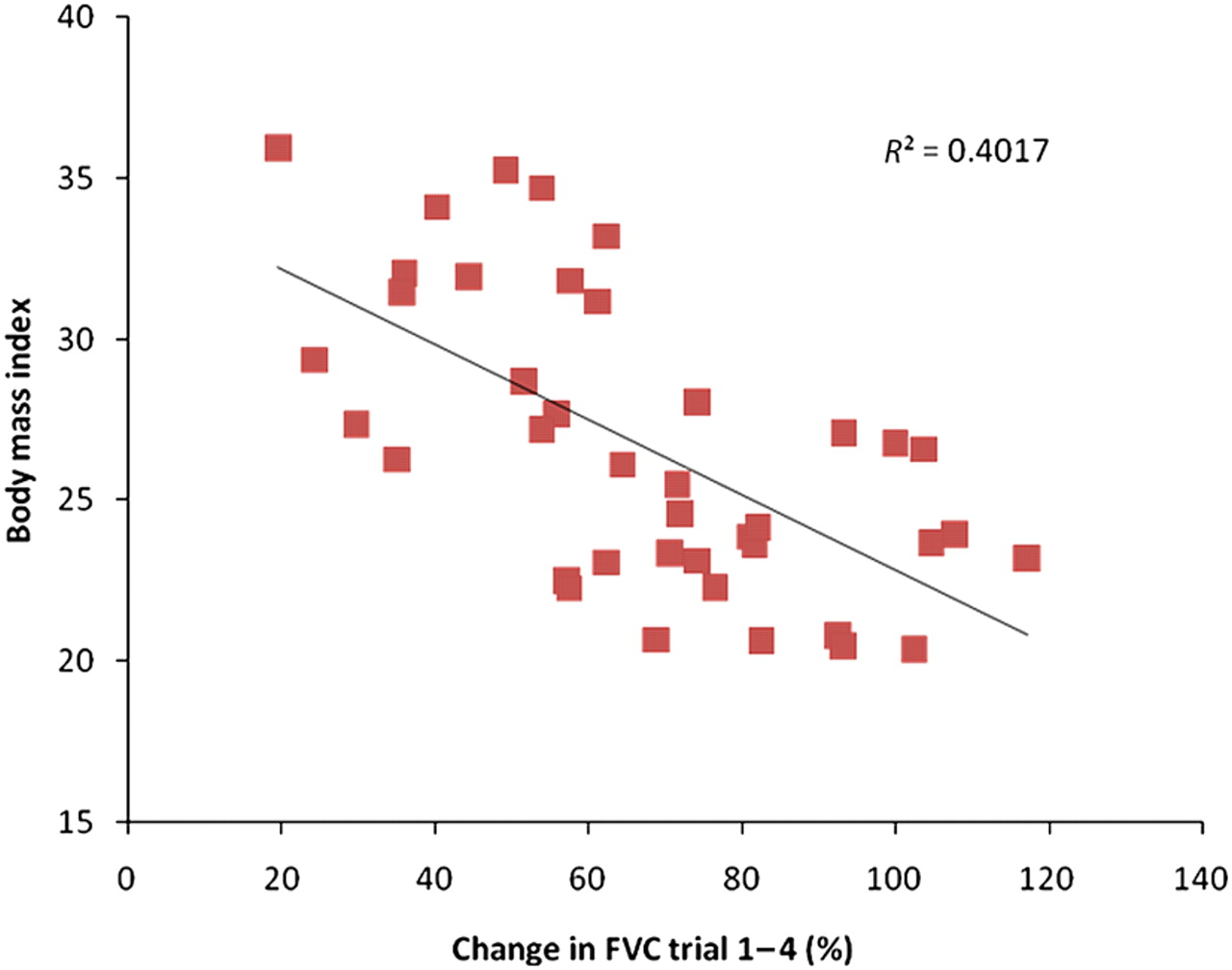
Change in FVC in relation to BMI. FVC, forced vital capacity; BMI, body mass index

Change in FVC in relation to seated waist girth. FVC, forced vital capacity
Figures show change (reduction) in lung function, comparing position one with position four, against BMI (Figure 5) and seated waist measurement (Figure 5).
Discussion
We examined two hypotheses:
Hypothesis one
Participants placed in a seated position, leant forward, will have significantly reduced lung function compared with a standing control position.
Hypothesis two
The above reduction in lung function will be greater in participants with higher BMI.
Both hypotheses are supported by the results reported here.
A seated position, with the participant leant forward, had a substantial effect on lung function. Across all participants lung function (FVC) was reduced to 67.4% of the standing control (P < 0.01). A seated position, sat up straight, had no significant effect on lung function. On most measures of lung function the addition of restraint holds to the seated, leant forward position, had no significant additional effect. It is concluded that it is the leant forward position, not the restraint holds, which is causal. (It should be noted that the level of force applied by the restraining staff during the measurements was slight compared with what might be applied during a resisted, real-world, restraint. Therefore, it remains possible that substantial additional force might result in further reduction in lung function.)
The effect of body size, defined by BMI and seated waist measurement, was also studied. Data were analysed in terms of two cohorts with a cut-off point of BMI 25, an arbitrary cut-off level that differentiated larger participants from smaller, but does not imply that clinical obesity is required to demonstrate an effect. Body size had little effect on lung function in standing or seated (upright) positions. In the seated, leant forward position larger body size made a significant additional contribution to the reduction in lung function caused by position. This suggests that the risk caused by the seated, leant forward position would be further increased where the restrained person was larger. The effect of waist measurement is noted and it is suggested that waist size is readily observable, as a risk increasing factor, to restraining personnel in a real world setting. Persons subject to restraint who have a large waist are likely to be at increased risk during seated restraint. The risk increasing effect of larger size has been noted elsewhere. 18
Substantial effects on lung function were observed in the seated, leant forward positions. For the BMI >25 group the mean lung function (FVC) in position four was 55.3% of standing control, a 44.7% reduction in lung function. This is both statistically and operationally significant. Previous research 16 using the same methodology examined the ‘figure four leg lock’ restraint position and demonstrated a mean reduction in FVC of 27.4% in this position. The ‘figure four leg lock’ is a restraint position that has been associated with death during prolonged, resisted restraint, 1 yet it is noted that a substantially greater effect on lung function was demonstrated in seated positions during this study.
The maximum effect on lung function (FVC, position one compared with position four) for any individual participant was a measurement of 19.6% of standing control, a reduction of 80.6%, with five participants showing reductions greater than 50%. Death during restraint is a rare phenomenon and is likely associated with worst-case scenarios. The worst-case scenario in a seated, leant forward position is a very substantial reduction in lung function.
The subjective experiences of participants are also noted. Participants repeatedly reported that they ‘cannot breathe’ in the seated, leant forward positions. One participant felt obliged to abort the procedure. This is the first time this has occurred during our work on restraint. It is noted that a subjective experience of being unable to breathe may cause a restrained person to panic and attempt to break out of the restraint, inducing restraining staff to apply greater force, thereby further increasing the level of risk.
Our overall conclusions are as follows:
A seated, upright position does not cause significant reductions in lung function; Seated, leant forward positions cause reductions in lung function that are both statistically and operationally significant; The addition of restraint holds to a person in the seated, leant forward position does not create a significant additional effect when restraint is applied with limited force; In seated (leant forward) positions, greater body size (BMI/waist girth) results in a greater reduction in lung function; The level of reduction in lung function in the seated, leant forward position is sufficient that it should be considered a potential risk of harm or fatality during prolonged restraint. This risk would be increased where the restrained person had a large waist girth.
In order to reduce risk, these findings should be taken into account in the development of restraint training and relevant personnel should be made aware of the key issues during training. The substantial reductions in lung function demonstrated in some individuals should be taken into consideration during future investigations of restraint-related deaths.